
+91 6002993949
submission@iarconsortium.org
Open Access
ISSN (Print) : 2709-1872
ISSN (Online) : 2709-1880
Introduction: Laryngoscopy and tracheal intubation is a noxious stimulus, leading to a marked sympathetic response. Patients with cardiovascular or cerebral disease are at increased risk. Various drugs and laryngoscopy methods are used to effectively attenuate this response. The aim of the study was comparing the clinical efficiency in attenuation of hemodynamic response provided by Tab pregabalin 200mg given 2 hours pre-emptively with that of IV lignocaine given 90 seconds prior to intubation and to study the side effects of the drug if any. Materials and Methods: After Ethical Committee Clearence from the institute and written informed consent. 30 patients, aged 18–60years, ASA grade I and II, of both genders were randomized into two groups of 15 each. Group I received Tab pregabalin 200mg 2 hours prior to surgery, Group II received Inj lignocaine 1.5mg/kg IV 90 seconds prior to intubation. Anaesthetic technique was standardized to both the groups. The statistical software namely SPSS 22.0, and R environment ver.3.2.2 were used for the analysis of the data and Microsoft word and Excel have been used to generate graphs, tables etc. Hemodynamic parameters were observed at baseline, pre-induction and 1,2,4,6,8,10 and 15 minutes after laryngoscopy and intubation along with sedation score and post-operative side effects. Results: The mean basal and pre-induction heart rate, systolic, diastolic and mean arterial pressure was comparable between 2 groups (p-value >0.05). The patients had significant attenuation in heart rate with (p-value <0.05) at 1,2,4,6, and (p-value <0.01) at 8,10,15 minutes in pregabalin group compared to lignocaine group, systolic, diastolic and mean arterial pressures were too significantly lower at 1,2,4,6,8,10 and 15minutes in pregabalin group. Conclusion: Pregabalin 200mg as premedication is more effective in attenuating hemodynamic response to laryngoscopy compared to IV lignocaine with no significant side effects.
The act of laryngoscopy and intubation results in cardiovascular changes like tachycardia and hypertension, though this stress response is transient, it can cause undesirerd effects on cardiovascular system like dysarrhythmias and myocardial ischemia [1]. The various pharmacological methods to attenuate hemodynamic stress response to laryngoscopy and tracheal intubation [2,3], includes the use of beta receptor blocking drugs [4], calcium channel blocking drugs [5], topical or parenteral local anaesthetics, opioids like fentanyl or remifentanil [6], vasodilating drugs [7], deepening the level of anesthesia.
Gabapentenoid group of drugs includes gabapentin and pregabalin. They are structurally related to the inhibitory neurotransmitter Gamma Amino Butryric Acid (GABA). Pregabalin has similar structure and mechanism of action as gabapentin. Recent studies have evaluated the role of pregabalin premedication on anxiolysis, opioid sparing effect and attenuation of stress response to laryngoscopy [7-9], by blunting the release of excitatory neuro amino acids, due to blockade of alpha2 delta subunit of neuronal calcium channels [8].
This prospective randomized study was done to compare the clinical efficiency in attenuation of hemodynamic response provided by Tab pregabalin 200mg given pre-emptively with that of IV lignocaine given 90 seconds prior to intubation and to study the side effects of the drug if any.
After institutional ethical committee clearance, thirty patients posted for various elective surgeries under general anesthesia were recruited for the study after they fulfilled below mentioned criteria.
Inclusion Criteria
Patients who give informed written consent.
Patients above 18 years of age
Patients belonging to ASA Grade I and Grade II
Patients posted for elective surgeries under general anesthesia
Exclusion Criteria
Patients who refuse to give informed written consent.
Patients with systemic disorders- uncontrolled hypertension, ischemic heart disease, cerebrovascular disease, uncontrolled diabetes mellitus, renal and hepatic disease, bronchial asthma.
Patients taking sedatives, antidepressants, anxiolytics, anticonvulsants or any other contraindication for the use of patient-controlled analgesia.
Patients with known history of allergy to any drugs
Anticipated difficult airway
Patients were recruited following their preoperative assessment and randomly assigned into two groups of 15 each using computer generated number. Group I received tablet pregabalin 200mg 2hr prior to surgery and Group II received Inj lignocaine 1.5mg/kg IV 90 seconds prior to intubation. Anaesthetic technique was standardized to both the groups. Hemodynamic parameters were observed at baseline, pre-induction and 1,2,4,6,8,10 and 15 minutes after laryngoscopy and intubation. All patients were premedicated with Inj glycopyrrolate 0.004mg/kg, Inj midazolam 0.02mg/kg, Inj fentanyl 2mcg/kg and Inj ondansetron 0.08mg/kg intravenously. After pre-oxygenation for 3 minutes, anaesthesia was induced with intravenous Inj propofol 2mg/kg. Following successful trial of ventilation, intravenous Inj vecuronium bromide 0.1mg/kg was given to facilitate laryngoscopy and intubation.
Patients were mask ventilated for 3 minutes. At the end of 3 minutes, direct laryngoscopy was performed using appropriately sized curved macintosh blade (No. 3 or 4) and endotracheal intubation done with appropriately sized cuffed oral endotracheal tube. Anesthesia was maintained with 50% nitrous oxide, 50% oxygen and 1% Isoflurane. At the end of surgery, patients were reversed with Inj neostigmine 0.05mg/kg, Inj glycopyrrolate 0.005mg/kg and were extubated and shifted to Post-Anesthesia Care Unit (PACU) and monitored for at least 3 hours. Drug induced side effects were recorded if any.
Statistical Methods
Descriptive and inferential statistical analysis has been carried out in the present study. Continuous variables were expressed as Mean±SD. Continuous variables were evaluated by student test or Mann Whitney U test. Categorical variables were assessed using Chi-squared test or Fisher Exact test. P less than 0.05 was taken as significant.
Statistical Software
The Statistical software namely SPSS 22.0, and R environment ver.3.2.2 were used for the analysis of the data and Microsoft word and Excel have been used to generate graphs, tables etc.
The patients in both the groups were comparable with respect to demographic data.
The mean duration of intubation in group I and II were 15.08±2.35 and 15.40±2.29 seconds respectively.
This was not significant statistically (p-value >0.05).
Both the groups are comparable in the basal and preinduction mean heart rate.
Pregabalin and IV ligncaine both have statistically significant effect on heart rate at all times following laryngoscopy and intubation (p-value <0.01).
Clinically the heart rate at 1 minute had increased by 6 beats in the pregabalin group and by 15 beats in the lignocaine group from the basal value.
Table 1: Comparison of Baseline Variables
| Variables | Pregabalin 200 | IV Lignocaine | Total | p-value |
| Age in years | 31.08±8.23 | 33.27±10.05 | 32.3±9.18 | 0.549 |
| Weight | 62.58±5.3 | 63.27±10.77 | 62.96±8.63 | 0.843 |
| Height | 153.17±15.71 | 161.67±12.49 | 157.89±14.39 | 0.130 |
| Height in MTS | 1.53±0.16 | 1.62±0.12 | 1.58±0.14 | 0.130 |
| BMI | 27.49±6.63 | 24.63±5.63 | 25.9±6.15 | 0.236 |
Table 2: Intubation Duration (In Secs)
| Intubation Duration (in secs) | Pregabalin 200 | IV lignocaine | Total |
| <15 | 7(46.7%) | 5(33.3%) | 10(37%) |
| 15-20 | 8(53.3%) | 10(66.7%) | 17(63%) |
| Mean ± SD | 15.08±2.35 | 15.40±2.29 | 15.25±2.28 |
p = 0.727, Not Significant, Student t Test
Table 3: Heart Rate (Per Min)- Comparison Between Two Study Groups
| Heart Rate | Pregabalin 200 | IV Lignocaine | Total | p-value |
| Basal | 87.17±8.99 | 86.8±8.2 | 86.96±8.39 | 0.913 |
| Pre-induction | 93.67±8.87 | 92.27±8.86 | 92.89±8.72 | 0.687 |
| 1 Min | 93.5±8.7 | 101.8±9.1 | 102.56±8.8 | 0.043* |
| 2 Min | 93±7.65 | 102.4±9.24 | 100.11±8.45 | 0.02* |
| 4 Min | 92.33±8.52 | 102.33±9.15 | 92.56±9.07 | 0.036* |
| 6 Min | 92.17±10.18 | 98.4±9.39 | 87.52±9.86 | 0.023* |
| 8 Min | 89.08±10.07 | 98.93±9.18 | 85.67±9.9 | 0.01* |
| 10 Min | 89.75±9.45 | 98.6±9.16 | 83.33±9.62 | 0.01* |
| 15 Min | 84±7.75 | 97.6±10.71 | 90.8±9.88 | 0.004* |
Table 4: Systolic Blood Pressure (mmHg)- Comparison Between Two Study Groups
| SBP (mm Hg) | Pregabalin 200 | IV Lignocaine | Total | p-value |
| Basal | 120.8±5.44 | 121.33±6.17 | 117.7±6.56 | 0.37 |
| Pre-induction | 122.93±4.33 | 121.5±5.27 | 117.85±5.74 | 0.8 |
| 1 Min | 120±4.07 | 126.67±4.85 | 122.96±5.5 | <0.001* |
| 2 Min | 120.67±4.32 | 126.58±4.8 | 123.3±5.36 | 0.002* |
| 4 Min | 115.87±3.6 | 118.33±5.97 | 116.96±4.86 | 0.196 |
| 6 Min | 113.87±4.16 | 117.5±6.82 | 115.48±5.69 | 0.100 |
| 8 Min | 111.73±4.06 | 117.17±6 | 114.15±5.63 | 0.010* |
| 10 Min | 107.33±8.74 | 115.42±4.94 | 110.93±8.26 | 0.009* |
| 15 Min | 107.67±18.45 | 110.33±6.54 | 110.52±14.19 | 0.053* |
Table 5: Diastolic Blood Pressure (mmHg)- Comparison Between Two Study Groups
| DBP (mm Hg) | PREGABALIN 200 | IV LIGNOCAINE | Total | p-value |
| Basal | 81.5±7.91 | 81.2±9.1 | 81.33±8.43 | 0.92 |
| Pre-induction | 80.33±8.17 | 81.73±8.58 | 81.11±8.27 | 0.65 |
| 1 Min | 86.83±7.93 | 88.47±8.16 | 87.19±7.91 | 0.58 |
| 2 Min | 84.5±7.04 | 90.93±7.17 | 86.74±6.98 | 0.01 |
| 4 Min | 75.67±12.21 | 86.33±6.87 | 77.7±9.59 | 0.006 |
| 6 Min | 72.33±10.78 | 86.27±6.51 | 73.96±8.61 | 0.0002 |
| 8 Min | 69.58±9.2 | 83.2±6.22 | 71.59±7.75 | 0.0001 |
| 10 Min | 67.5±7.44 | 77.87±3.6 | 73.37±5.77 | <0.0001 |
| 15 Min | 65.33±7.15 | 77.8±3.45 | 73.37±5.98 | <0.0001 |
Table 6: Mean Arterial Pressure (mmHg)- Comparison Between Two Study Groups
| MAP (mm Hg) | Pregabalin 200 | IV Lignocaine | Total | p-value |
| Basal | 94.6±6.12 | 94.56±6.95 | 94.58±6.58 | 0.98 |
| Pre-induction | 94.52±6.22 | 94.98±5.95 | 94.75±5.99 | 0.83 |
| 1 Min | 97.88±6.1 | 101.18±5.8 | 99.53±5.88 | 0.14 |
| 2 Min | 96.53±5.63 | 102.78±5.19 | 99.66±5.35 | 0.03 |
| 4 Min | 89.04±8.76 | 96.99±4.95 | 93.01±6.8 | 0.04 |
| 6 Min | 86.15±8.71 | 96.68±4.53 | 91.41±6.58 | <0.001 |
| 8 Min | 83.62±7.45 | 94.5±4.24 | 89.06±5.77 | <0.001 |
| 10 Min | 80.76±6.29 | 90.38±3.51 | 85.57±4.84 | <0.001 |
| 15 Min | 79.42±6.41 | 86.63±5.66 | 84.02±6.18 | 0.002 |
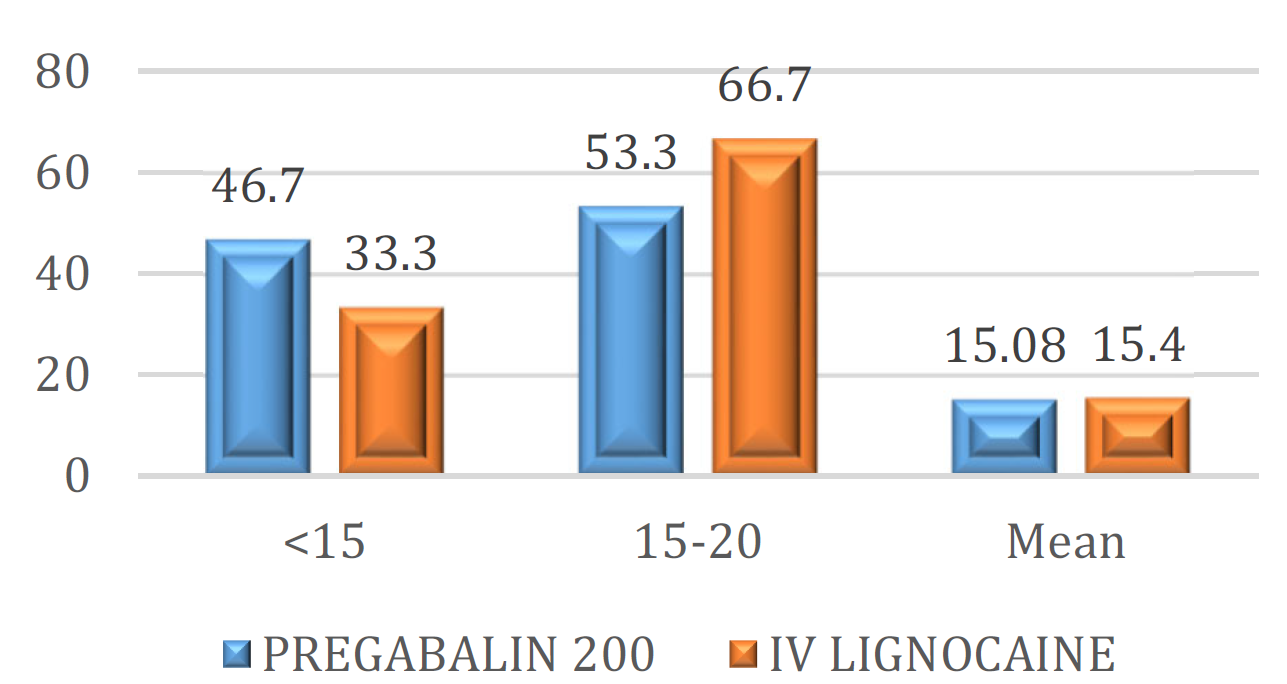
Figure 1: Intubation Duration (In Secs)
The magnitude of rise in heart rate was lower and falling to less than the basal value by 15 minutes in the pregabalin group. However, the rise in heart rate in the lignocaine group was sustained and had not reached the basal value even by 15 minutes following laryngoscopy and intubation.
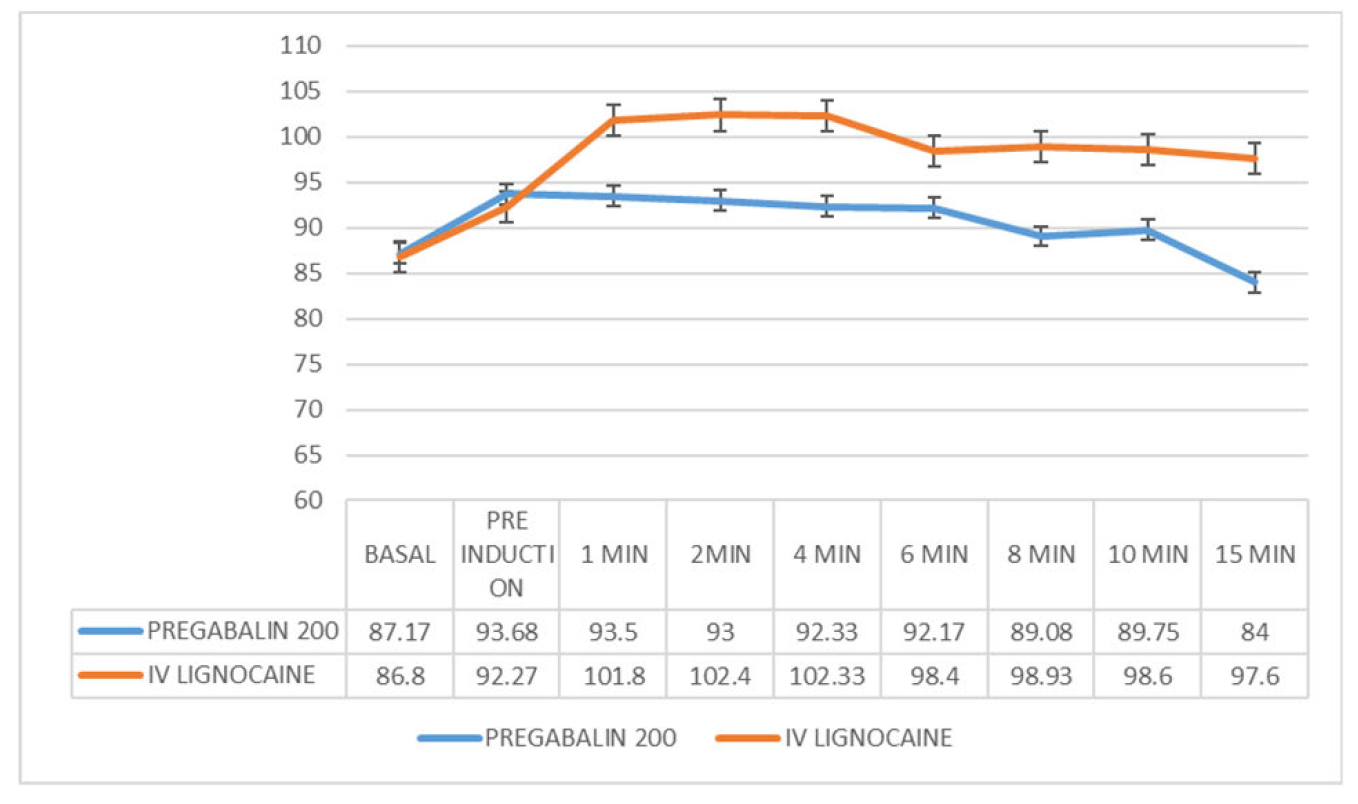
Figure 2: Heart Rate (Per min)- Comparison Between Two Study Groups
There was a statistically significant rise (p-value <0.01) in systolic blood pressure in both the groups at 1- and 2-mins following laryngoscopy and intubation which was greater in the lignocaine group.
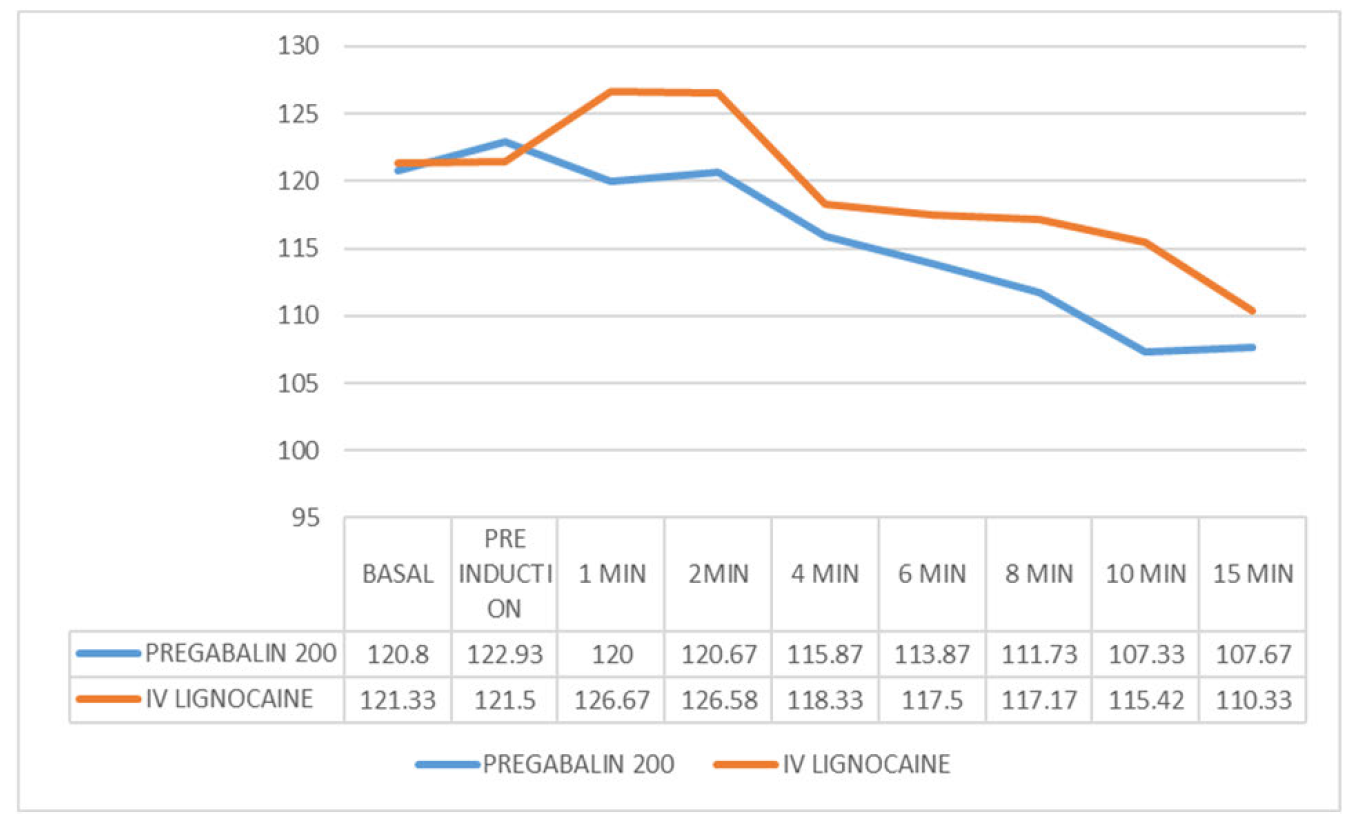
Figure 3: Systolic Blood Pressure (mmHg)- Comparison Between Two Study Groups
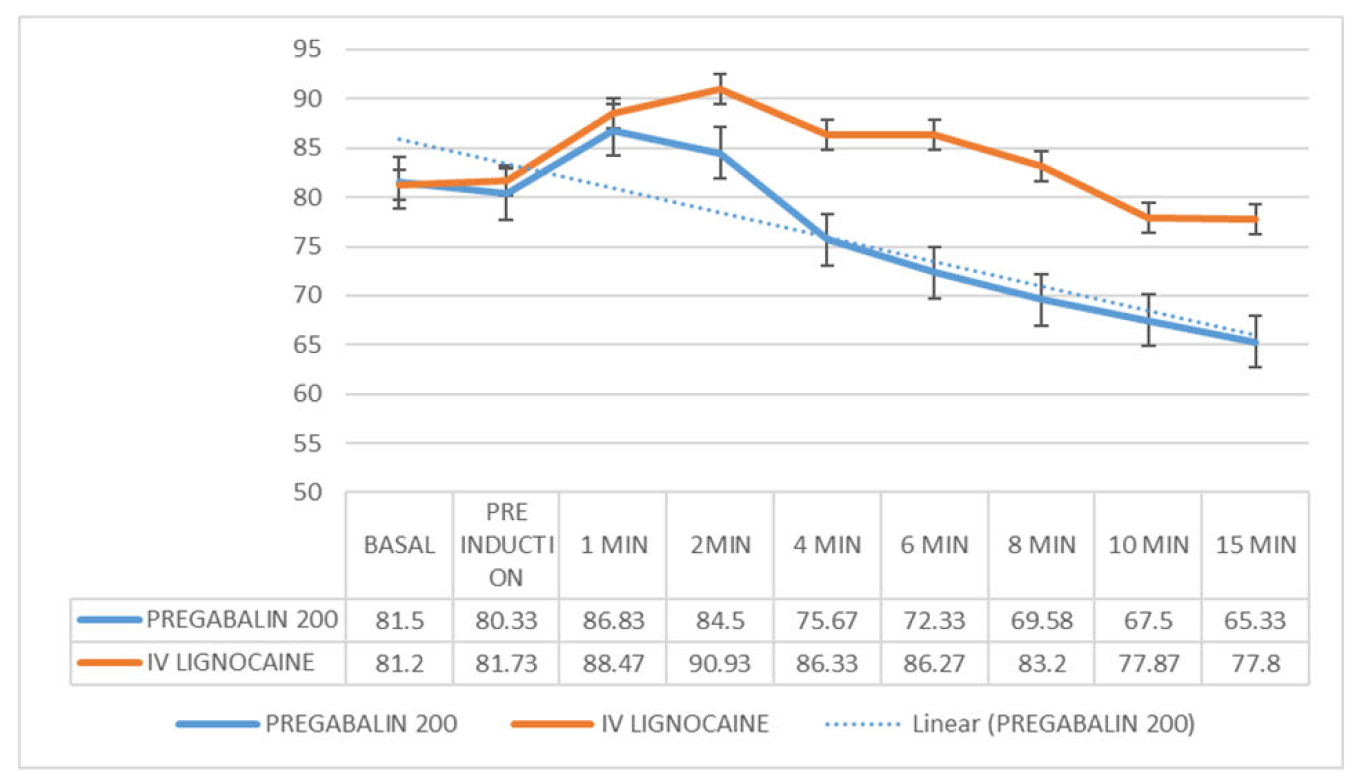
Figure 4: Diastolic Blood Pressure (mmHg)- Comparison Between Two Study Groups
The magnitude of rise in systolic blood pressure was lower and found to be falling to less than the basal value by 4 minutes in the pregabalin group. However, the rise in systolic blood pressure in the lignocaine group was more sustained reached the basal value by 6 minutes following laryngoscopy and intubation.
The mean diastolic blood pressure after 1 min was lower and statistically significant (p-value <0.01) in the pregabalin group compared to the lignocaine group.
The mean diastolic blood pressure is lower and the trend is lesser in the pregabalin group than lignocaine group.
The mean arterial pressure at basal and preinduction are comparable in both groups (p-value >0.05)
The mean arterial pressure at all times following laryngoscopy and intubation is lower and statistically highly significant in pregabalin group (p-value <0.01).
The trend in mean arterial pressure is better in the pregabalin group.
Laryngoscopy and endotracheal intubation are considered as the most critical events during general anaesthesia as they provoke transient but marked sympathoadrenal response manifesting as hypertension and tachycardia.
These responses are usually transient and inconsequential in normal individuals.
Patients with cardiovascular diseases like hypertension, ischemic heart disease, cerebrovascular disease, intracranial aneurysms, the changes in hemodynamic variables can result in harmful effects like left ventricular failure, pulmonary edema, myocardial ischemia, and cerebral haemorrhage. Therefore, it is essential to attenuate this response to laryngoscopy and endotracheal intubation. The newer methods include the use gabapentin and pregabalin given pre-emptively.
The present study was undertaken to compare the clinical efficiency in attenuation of hemodynamic response provided by tablet pregabalin 200mg given pre-emptively with that of IV lignocaine given prior to intubation.
Several studies have been done comparing different doses of tablet pregabalin given pre-emptively to attenuate hemodynamic response to laryngoscopy and endotracheal intubation, however no study was done comparing the efficacy of pregabalin with that of IV lignocaine.
Anudeep Saxena et al. [10], in their study titled “Effect of Pregabalin Premedication on the Laryngoscopic Response and Intra-operative Hemodynamic Variables in Laparoscopic Cholecystectomy: A Randomized Comparison of Two Doses” done on 90 patients (30 patients each in placebo, group 2 receiving pregabalin 75mg HS and 150mg 1 hr prior to surgery, group 3 receiving pregabalin 75mg HS and 300mg 1hr prior to surgery concluded that oral pregabalin is more effective compared to diazepam and both 150mg and 300mg were equally effective in diminishing the cardiovascular response [10].
Ritwik Chakraborty et al. [11], in their study titled ‘Evaluation of the efficacy of pre-operative oral pregabalin in attenuating haemodynamic response to laryngoscopy and intubation and on post-operative pain in patients undergoing elective surgery under general anaesthesia’ done on 50 patients of group pregabalin 150mg given 1hr prior to surgery and group C (receiving placebo) concluded that pregabalin 150mg premedication safely attenuates haemodynamic responses to laryngoscopy and intubation and decreases post-operative pain with acceptable levels of sedation [11].
Dheer Singh et al. [12], in their study titled ‘Oral Pregabalin as Premedication on Anxiolysis and Stress Response to Laryngoscopy and Endotracheal Intubation in Patients Undergoing Laparoscopic Cholecystectomy: A Randomized Double‑Blind Study’ done on 60 patients (Group 1 receiving placebo and group 2 receiving pregabalin 150mg) concluded that pregabalin 150 mg is an effective and safe drug for anxiolysis, analgesia, and hemodynamic stability during laryngoscopy and intubation and can be useful for patients with comorbid conditions preoperatively [12].
Limitations
We did not measure the stress mediators such as plasma catecholamines or cortisone. The dose response effect of pregabalin was not done.
Pregabalin 200mg as premedication is more effective in attenuating hemodynamic response to laryngoscopy compared to IV lignocaine.
The present study did not show any serious side effects with a single oral dose of pregabalin 200mg.
E. Lowenstein. "Perianesthetic ischemic episodes cause myocardial infarction in humans – A hypothesis confirmed." Anesthesiology, vol. 62, no. 2, 1985, pp. 103–106. https://doi.org/10.1097/00000542-198502000-00001.
R.F. Bedford and W.K.Marshall. "Cardiovascular response to endotracheal intubation during four anesthetic techniques." Acta Anaesthesiologica Scandinavica, vol. 28, no. 5, October 1984, pp. 563–566. https://doi.org/10.1111/j.1399-6576.1984.tb02120.x.
J.M. Low et al. "Studies of anaesthesia in relation to hypotension VII." British Journal of Anaesthesia, vol. 58, no. 5, 1986, pp. 471–477. https://doi.org/10.1093/bja/58.5.471.
M. Vucevic et al. "Esmolol hydrochloride for management of cardiovascular stress responses to laryngoscopy and tracheal intubation." British Journal of Anaesthesia, vol. 68, no. 5, 1992, pp. 529–530. https://doi.org/10.1093/bja/68.5.529.
K.Mikawa et al. "The effect of diltiazem on cardiovascular."
D.R.Miller et al. "Effects of alfentanil on hemodynamic and catecholamine response to tracheal intubation." Anesthesia and Analgesia, vol. 76, 1993, pp. 1040–1046.
A. Fassoulaki and P. Kaniaris. "Intranasal administration of nitroglycerin attenuates the pressor response to laryngoscopy and intubation of trachea." British Journal of Anaesthesia, vol. 55, no. 1, 1983, pp. 49–52. https://doi.org/10.1093/bja/55.1.49.
B. Rastogi et al. "Oral pregabalin premedication for attenuation of haemodynamic pressor response of airway instrumentation during general anaesthesia: a dose response study." Indian Journal of Anaesthesia, vol. 56, no. 1, January–February 2012, pp. 49–54. https://doi.org/10.4103/0019-5049.93344.
G. Eren et al. "Pregabalin blunts cardiovascular responses to laryngoscopy and tracheal intubation." Journal of Anesthesiology and Reanimation, vol. 7, 2009, pp. 82–87.
A. Saxena et al. "Effect of pregabalin premedication on the laryngoscopic response and intra-operative hemodynamic variables in laparoscopic cholecystectomy: A randomized comparison of two doses." International Journal of Scientific Study, vol. 4, no. 5, 2016, pp. 75–80.
R. Chakraborty et al. "Evaluation of the efficacy of preoperative oral pregabalin in attenuating haemodynamic response to laryngoscopy and intubation and on post-operative pain in patients undergoing elective surgery." Indian Journal of Clinical Anaesthesia, vol. 3, no. 3, 2016, pp. 423–430. https://doi.org/10.5958/2394-4994.2016.00071.8.
