
+91 6002993949
submission@iarconsortium.org
Open Access
ISSN (Print) : 2709-1872
ISSN (Online) : 2709-1880
The overall incidence of the Sinus of Valsalva aneurysm (SOVA) is 0.09% in the general population and comprise 0.1% to 3.5% of all congenital cardiac defects. It is associated with only 2% of Tetralogy of Fallot (TOF) patients, thus making this combination of unruptured SOVA with TOF unique. We present the case of a 4½- year-old West African boy who developed exertional dyspnea and frequent squatting episodes since the age of ten months. He was not having any other major medical/ genetic history or phenotypically syndromic features. Preoperative diagnosis was confirmed with Trans Esophageal Echocardiography (TEE) features of TOF with SOVA arising from right coronary cusp (RCC) bulging but not distorting Right Ventricular Outflow Tract (RVOT). The narrowest portion of the aneurysm being 0.65 cm. Postoperative Adequacy of TOF repair was demonstrated by ruling out residual Ventricular Septal Defect (VSD), morphological distortion as stenosis/ regurgitation across both Left Ventricular Outflow Tract (LVOT) and RVOT. The measurements of RVOT and LVOT at different levels were compared with the Z- scores provided by the Detroit data. TEE was useful not only in pointing out the adequacy of repair but also predicted not requiring additional intervention especially to aortic valve in the near future.
Sinus of Valsalva aneurysm is not only a rare anomaly but also not commonly associated with TOF patients. The overall incidence of the sinus of Valsalva aneurysm is 0.09% in the general population. It comprises 0.1% to 3.5% of all congenital heart defects. Only seen in 2% of TOF patients [1 -2], thus making this combination of unruptured SOVA with TOF unique .
Unruptured SOVA can silently present with a myriad of sequelae, from asymptomatic expansion to the most dreaded, ruptured SOVA, whose peri - operative mortality rate is 3.9% [3]. We are reporting a case of unruptured SOVA with TOF who was posted for definitive correction electively. Intraoperative Trans Esophageal Echocardiography provided its detailed information, ruled put possible complications, and guided in deciding appropriate interventions [4].
Case Report
We obtained informed consent from the guardian for anaesthesia, surgery, publishing clinical profile, and maintaining data confidentiality. 4 ½year-old West African boy developed exertional dyspnea and frequent squatting episodes since the age of 10 months. No other major medical/ genetic history or phenotypically syndromic features were noted. Preoperative TTE displayed features of TOF, viz., Right Ventricular Hypertrophy (RVH), Non- restrictive membranous Ventricular Septal Defect with outlet extension, Severe Right Ventricular Outflow Tract obstruction, and Aortic override. Besides, SOVA was detected arising from the right coronary cusp.
Preoperative TEE findings (Figure 1-2)
Mid-Esophageal Aortic Valve Long Axis view (ME AV LAX)
confirmed our preoperative findings. SOVA was at the level of RCC bulging but not distorting RVOT. The diameter of the narrowest part is 0.65 cm. It also did not affect aortic valve function. Leaflet coaptation was adequate without subluminal distortion nor stenosis/ regurgitation of the aortic valve. The aneurysmal sac originated from sinus extra murally without affecting Inter- Ventricular Septum.
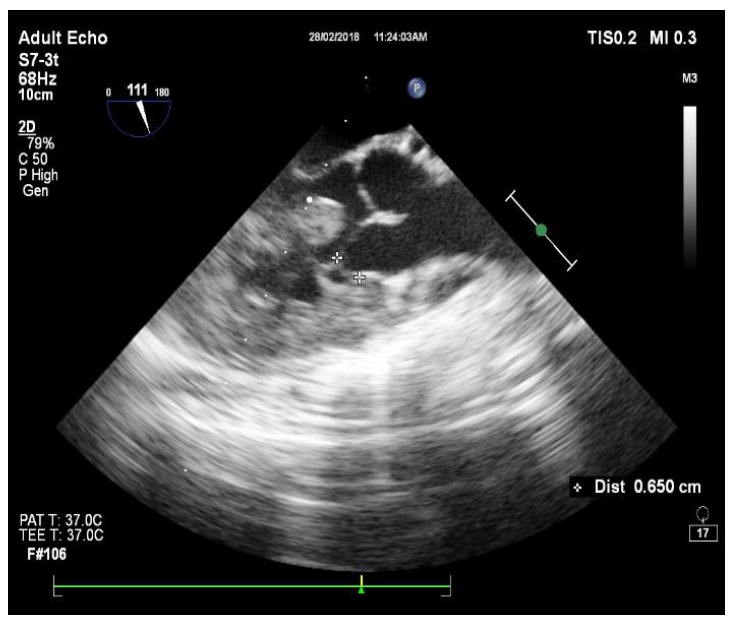
Figures 1: Preoperative Mid-Esophageal Aortic Valve
Long Axis View (ME AV LAX) in 2-D
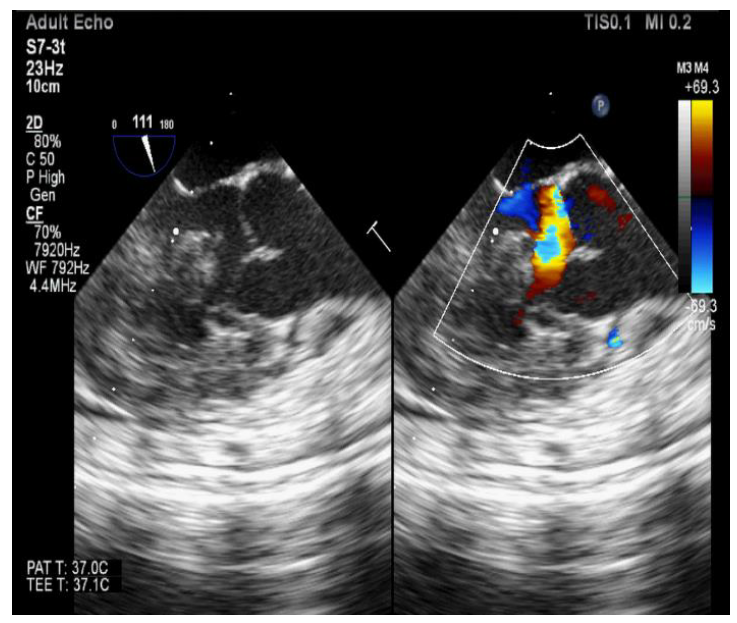
Figures 2: Preoperative Mid-Esophageal Aortic Valve
Long Axis (ME AV LAX) View in 2-D and Colour Doppler
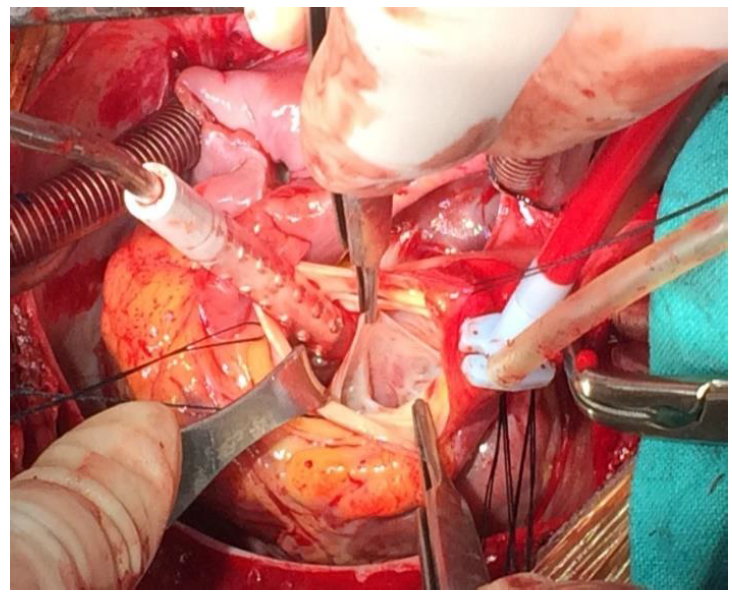
Figures 3: Surgical view (Photographed from Headend. The Suction Cannula and Retractor are Isolating SOVA. The Forceps to the Right of the Cannula are Retracting RCC)
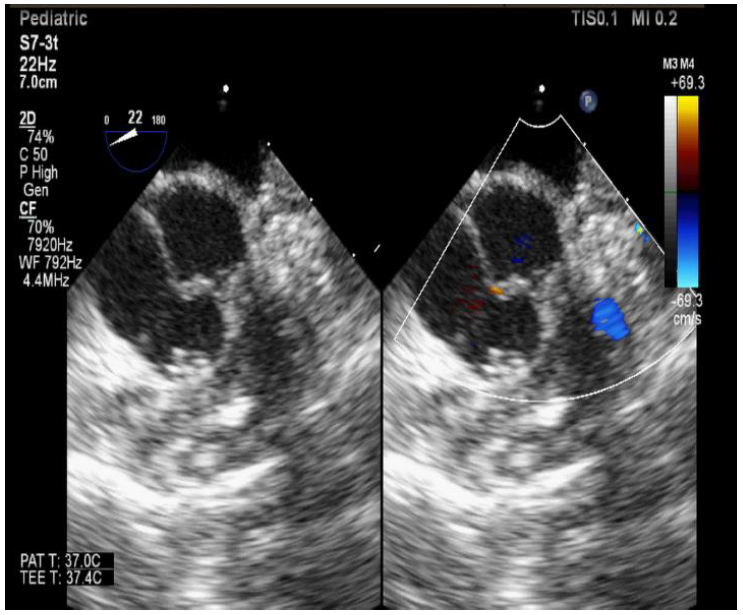
Figure 4: Postoperative Mid-Esophageal Aortic Valve Short Axis (ME AV SAX) view 2D and Colour. No Residual VSD or Aortic Regurgitation
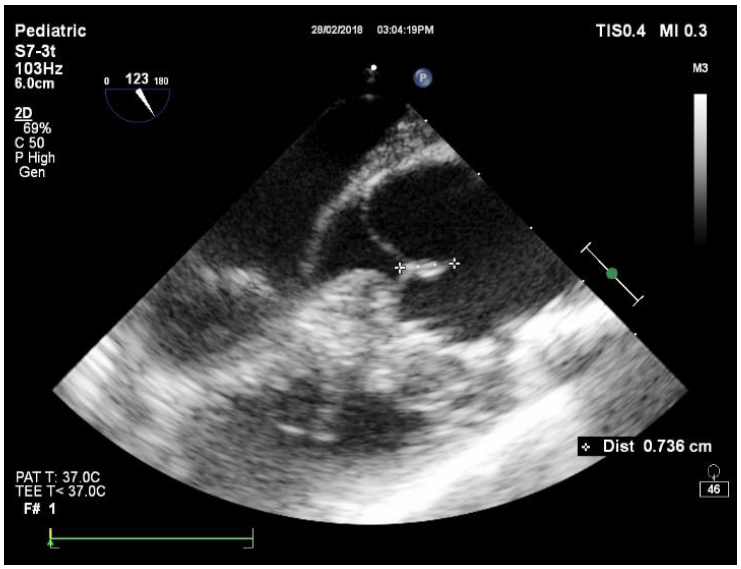
Figure 5: Postoperative Mid-Esophageal Aortic Valve Long Axis (ME AV LAX). Leaflet Coaptation Distance = 0.736 cm (Adequate)
Table 1: The Pre and Postoperative Measurements of Dimensions and Z- Scores
Site | Size [cm] | Z- score | ||||
Pre- Op | Post- Op | Pre- Op | Post- Op | |||
LVOT | 1.07 | 1.28 | - | - | ||
Aortic Valve annulus | 2.33 | 1.89 | +8.28 | +4.64 | ||
Sinus | - | 2.63 | - | +4.83 | ||
Sino- tubular Junction | - | 2..44 | - | +3.77 | ||
Proximal Ascending Aorta | - | 2.42 | - | - | ||
Aortic Valve area (cm2) | 2.73 | 2.53 | +4.87 | +4.33 | ||
Pulmonary Valve annulus | 1.56 | - | -0.17 | - | ||
Proximal MPA | 1.54 | - | -0.44 | - | ||
LPA | 0.87 | - | -0.22 | - | ||
RPA | 1.02 | - | -0.12 | - | ||
Neck of Aneurysmal sac | 0.65 | - | Absent | - | ||
The occurrence of the overall incidence of the Sinus of Valsalva aneurysm (SOVA) is 0.09% in the general population. It comprises 0.1% to 3.5% of all congenital heart defects and is associated with only 2% of Tetralogy of Fallot patients, thus making this combination of un- ruptured SOVA with TOF unique [1-2]. Besides, the fact that this child belonged to an African ethnic group unlike the high prevalence in Asians makes this clinical profile even rarer and distinct [1]. Clinical examination ruled out the possibility of connective tissue disorders like Marfan’s syndrome, etc. Intraoperative TEE corroborated with the clinical examination by demonstrating the LVOT dimensions within the acceptable range [5]. Most of the patients, including ruptured SOVA, are diagnosed incidentally [1]. Lilllehei et al. in the late 50s not only reported ruptured SOVA but also emphasised the importance of surgical intervention [6]. Vural et al. in their review of SOVA patients also mentioned about their association with TOF, although it was not clear whether the SOVA was ruptured or not [2]. Presences of symptoms are often associated with rupture. Aneurysmal IVS can be misdiagnosed as SOVA. Hence, detailed evaluation, which can alter surgical treatment, is necessary [7-8]. RCC is commonly involved and incidence of rupture in adulthood is high, hence the need for early intervention [1]. Grellner et al reported mortality associated with ruptured SOVA in a young patient [9]. Feldman et al. have also mentioned complications like arrhythmias, ischemia, and thromboembolic events [10-11].
Preoperative TEE demonstrated accurate diagnosis, location of the aneurysm and also helped differentiate it from IVS involvement and rupture. Although transthoracic echocardiography is an initial investigation of choice, TEE is the most sensitive, accurate, and recommended subsequent investigation [10]. The narrowest portion of the aneurysm being 0.65 cm, made it easier to plicate extramurally. The measurements of RVOT and LVOT at different levels were compared with the Z- scores provided by the Detroit data [5]. Takach et al. used pericardial patch repair technique and in some patients, replaced aortic valve [3, 12]. However, it was apprehended that the aortic valve is vulnerable to distortion due to the anatomical proximity of the aneurysm repair site [3]. Colour and Spectral Doppler assessments ruled out the possibility of aortic stenosis, regurgitation, and morphological distortion. Hall et al noted that when the length of the coaptation of aortic leaflets is more than 4 mm in ME AV LAX view, the recurrence of aortic regurgitation in the future is significantly low [4]. Waroux et al. also expressed a similar conclusion in their study on postoperative patients who underwent aortic valve repair [13]. Their study also concluded the major predictors of failure of repair surgeries, viz. coaptation length <4 mm, the tip of the coaptation below the annulus, presence of residual postoperative aortic insufficiency and dilated aortic annulus. We noticed that both the pre and postoperative dimensions of the aortic annulus was>+3 as per Detroit data [4]. However, there was a decrease in calibre after the repair, and the presence of other strong predictors mentioned by Waroux et al. made us infer not to intervene in the LVOT further [13]. These findings were the predominant deciding factors to intervene, approach, and treat surgically, given the various choices of interventions available for SOVA [2].
This was a rare and unique case of unruptured SOVA incidentally found associated with TOF in child of African ethnicity. Intraoperative TEE findings provided a volume of information. It helped to rule out ruptured SOVA, aneurysmal IVS, regurgitation/ stenosis of the aortic valve, and also localize it accurately. These factors helped in deciding appropriate surgical intervention, both for TOF and SOVA. Postoperatively, TEE was useful not only in pointing out the adequacy of repair but also predicted not requiring additional intervention especially to aortic valve in the near future.
Weinrich M. et al. “Sinus of valsalva aneurysms: review of the literature and an update on management.” Clinical Cardiology, vol. 38, no. 3, 2015, pp. 185–189.
[2] Vural K.M. et al. “Approach to sinus of valsalva aneurysms: a review of 53 cases.” European Journal of Cardiothoracic Surgery, vol. 20, 2001, pp. 71–76.
[3] Takach T.J. et al. “Sinus of valsalva aneurysm or fistula: management and outcome.” Annals of Thoracic Surgery, vol. 68, 1999, pp. 1573–1577.
[4] Hall T. et al. “The role of transesophageal echocardiography in aortic valve preserving procedures.” Indian Heart Journal, vol. 66, 2014, pp. 327–333.
[5] Petterson M.D. et al. “Regression equations for calculation of Z scores of cardiac structures in a large cohort of healthy infants, children, and adolescents: an echocardiographic study.” Journal of the American Society of Echocardiography, vol. 21, no. 8, 2008, pp. 922–934.
[6] Lillehei C.W. et al. “Surgical treatment of ruptured aneurysms of the sinus of valsalva.” Annals of Surgery, vol. 146, no. 3,1957, pp. 459–472.
[7] Singh S. et al. “A rare case of transposition of great arteries with an intact septum and aorto pulmonary window.” Journal of Surgery, vol. 2, no. 2, 2014, pp. 24–26.
[8] Raut M.S. et al. “Aneurysm: sinus of valsalva or ventricular septal?” Annals of Cardiac Anaesthesia, vol. 18, no. 3, 2015, pp. 427–429.
[9] Grellner W. et al. “Fatal outcome of a congenital aneurysm of the right sinus valsalvae ruptured into the right atrium.” Zeitschrift für Kardiologie, vol. 84, no. 7, 1995, pp. 553–559.
[10] Feldman D.M. and Roman M.J. “Aneurysms of the sinuses of valsalva.” Cardiology, vol. 106, 2006, pp. 73–81.
[11] Ali N.P. et al. “Dexmedetomedine-ketamine versus propofol- ketamine as anaesthetic agents in paediatric cardiac catheterization.” Journal of Armed Forces Medical College, Bangladesh, vol. 10, 2014, pp. 19–24.
[12] Singh S. and Singh A. “Current status of nanomedicine and nanosurgery.” Anesthesia: Essays and Researches, vol. 7, no. 2, 2013, pp. 237–242.
[13] Le Polain De Waroux J.B. et al. “Mechanisms of recurrent aortic regurgitation after aortic valve repair: predictive value of intraoperative transeophageal echocardiography.” JACC Cardiovascular Imaging, vol. 2, 2009, pp. 931–939.
