
+91 6002993949
submission@iarconsortium.org
Open Access
ISSN (Print) : 2788-9475
ISSN (Online) : 2788-9483
Despite the availability of a preventative vaccination for hepatitis B virus (HBV) for more than 20 years, HBV infection continues to be a major worldwide health burden 50 years after the virus was first discovered. Cirrhosis, hepatic decompensation and hepatocellular cancer (HCC) are all possible outcomes of the chronic HBV infection that affects more than 240 million individuals worldwide. Clinical consequences are more prevalent in older males with hepatitis B e antigen (HBeAg)-positive illness, high-grade liver necroinflammation and progressing fibrosis.Recent improvements in our knowledge of the natural history of chronic HBV infection have displayed that plasma HBV DNA levels play an essential role as a risk predictor for clinical outcomes. In adults, a higher risk of developing cirrhosis and HCC is shown when high-level HBV replication is allowed to exist for an extended period of time. Accordingly, the goal of treatment has shifted to one of long-term suppression of the virus. Hepatitis B surface antigen levels, also called HBsAg, are becoming an increasingly important sign of natural history. Low levels of HBsAg have been linked to better control of the immune system, HBsAg seroclearance and a lower risk of getting HCC.This research examines the natural course of HBV infection, focusing on clinical outcome factors in CHB patients.
Hepatitis B virus (HBV) infects over 2 billion individuals worldwide and more than 240 million chronic carriers are at risk of developing liver cirrhosis or hepatocellular carcinoma in the future [1].
According to the prevalence of HBV infection, the globe is classified into three endemic zones. The high prevalence (8%–15%), moderate prevalence (2%–7%) and low prevalence (2%) areas [2]. Iraq is classified as an intermediate HBV endemic country since the population's HBV infection rate ranges between (3%-4.5%) and (2%-3%) among seemingly healthy blood donors [3].
HBV is a DNA virus that belongs to the Hepadnaviridae family. The HBV -DNA genome is circular and partially double stranded. The minus DNA strand contains all of the coding information, which is structured into five open reading frames [4]
As first-line therapies for CHB, international guidelines recommend two types of drugs: peginterferon (Peg IFN), which boosts the immune system's response to HBV and nucleotide analogues (NAs), which stop viral replication directly. At the current time, treatment with antiviral medication for CHB may dramatically decrease the course of HBV infection [5].
The present research seeks to evaluate the prevalence of hepatitis B virus in terms of age, gender and location, as well as to investigate the clinical kinds of this virus.
Hepatitis
Hepatitis is a systemic illness that mostly affects the liver, which is the main place where the virus replicates. Symptoms of hepatitis include fever, jaundice and stomach problems. Aside from viruses, bacteria, parasites, fungi and chemicals like drugs, toxins and alcohol can also cause liver inflammation, which is called hepatitis [6].
Viral Hepatitis
Viral hepatitis is the most common cause of liver disease around the world. It is caused by one of five hepatitis viruses: Hepatitis A virus (HAV), Hepatitis B virus (HBV), Hepatitis C virus (HCV), Hepatitis D virus (HDV) and Hepatitis E virus (HEV) ( HEV ). hepatitis F virus (HFV), hepatitis G virus (HGV), TT virus and SEN-virus. Other viruses, such as cytomegalovirus (CMV), Epstein-Barr virus (EBV), yellow fever and Herpes Simplex virus, which only makes up about 1-2% of cases [7].
Hepatitis B virus ( HBV ) History and Classification
MacCallum published the first report regarding Hepatitis B virus (HBV) in 1947. Nevertheless, the virus was not identified until 1965. 1970 saw the discovery of the viral particle using electron microscopy by Dane DS and others. By the early 1980s, the virus's genome had been sequenced and the first vaccinations were being tried. HBV is the smallest DNA virus that can infect humans. Its genome is between 3.1 and 3.2 kb and it is the first member of the family Hepadnaviridae. This family is split into two genera: Orthrohepadnaviridae (infects mammals) and Avihepadnaviridae (infects birds) [7].
HBV Virion Structure
The viral "DNA and DNA polymerase are kept in the icosahedral nucelocapsid", which is made up of core protein (HBcAg) and is surrounded by an outer lipid membrane (envelope) that contains large (LHBs), medium (MHBs) and small (SHBs) surface proteins [8]. This entire infectious virus is referred to as the Dane particle [9]. Additionally, the serum may include filamentous and spherical particles with a diameter of 22 nm that lack the viral core protein and viral nucleic acid [10]. For them, there is no interior structure beyond the lipid membrane that surrounds the surface proteins [9]. The structure of the HBV virion is seen in Figure 1.
HBV Replication
Replication of HBV begins with the binding of the infectious virion to a preS1 receptor found only on hepatocytes, as shown in Figure 1 [11] A recent study shows that the part of pre-S1 that binds to receptors interacts in a very specific way with sodium taurocholate cotransporting polypeptide (NTCP).The liver is the primary organ responsible for producing the multiple transmembrane transporter known as NTCP [12] Viruses can infiltrate cells either by fusing to the plasma membrane or endocytosing the nuclocapsid and then fusing to the cell [13] Following virus entry, the viral nucleocapsid is released into the cytoplasm [12] The C-terminus of HBcAg in the protein coat serves as a nuclear localization signal that directs transport of the nucleocapsid to the nucleus [13]. This carries the virus to the nuclear membrane, where it releases relaxed circular DNA (rcDNA) into the nucleoplasm [14]. At this point, the viral polymerase finishes making the positive strand by fixing the rcDNA [15] When two positive and negative DNA strands are joined together, a mini-chromosome called covalently closed circular DNA (cccDNA) is constructed [13]. This serves as a transcriptional template for RNA polymerase II, producing six genomic and subgenomic RNAs:
The translation of "pregenomic RNA" (pgRNA) into "HBcAg and polymerase"
The translation of "preC/C mRNA" into "HbeAg"
The translation of "preS2 mRNA" into "MHBs" (preS2/S)
The translation of "S mRNA" into the "SHBs" (S)
The translation of "X mRNA" into the "X protein" [15].This transcription is controlled by viral and host factors, including viral proteins (core, the regulatory X protein) and CCAAT/enhancer-binding protein (C/EBP)/hepatocyte nuclear factors (HNF), correspondingly [16]
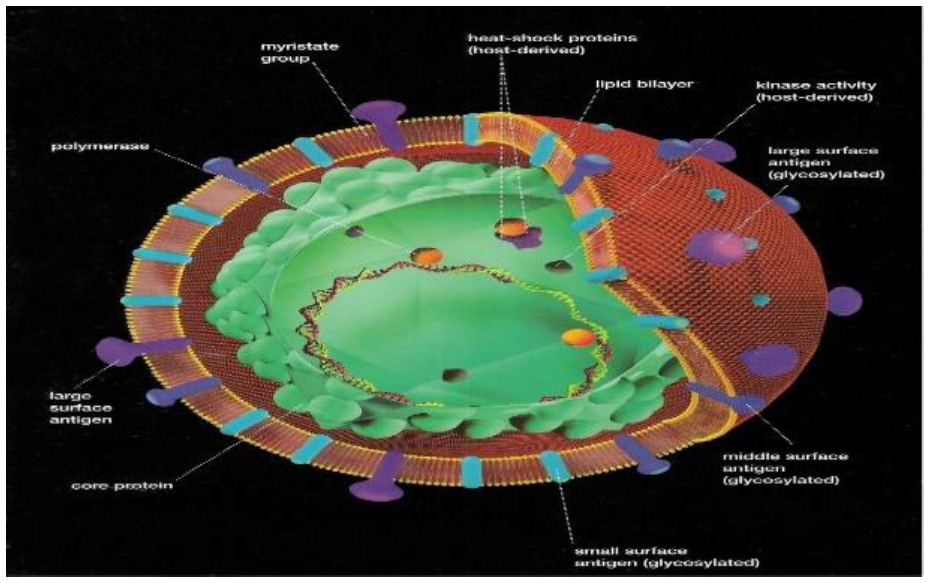
Figure 1: Hepatitis B Virion Structure [10]
Clinical Types of HBV Infection
Silent Primary Infection: HBV infections often have asymptomatic courses and result in immunity in people with good immune systems [16]. Diagnosis of asymptomatic persons is possible by detecting biochemical or viral-specific serologic abnormalities in their blood. They are at risk of becoming asymptomatic carriers of the virus, which would contribute to its spread to other people [17].
Acute HBV Infection
As the ampunt of HBV-infected hepatocytes is still minimal at the time when an efficient immune response is established, the infection is usually self-limiting and symptomless during the incubation phase of acute hepatitis B (AHB) infection in around 90% of cases [18]. The vast majority of patients recover without serious repercussions and without recurrence after 4 to 8 weeks of sickness [19] When a patient has a clinical sickness, the symptoms often appear gradually and include fatigue, anorexia, unexplained stomach pain, nausea and vomiting. Sometimes, arthralgias, rash, w`hich often progresses to jaundice and either a lack of or a slight fever [18].
Chronic HBV Infection
Chronic B hepatitis infection CHB is an infection that lasts longer than six months. Although the majority of AHB-infected adult patients recover completely, the virus remains in the bodies of 5-10% of them. This proportion is significantly higher in children, with 70-90% of infants infected within their first few years becoming chronic HBV carriers [19]. CHB infection occurs in 40-70% of HBV infections under the age of three years [18]. The severity of the accompanying inflammatory liver disease varies. Despite being far less severe than in AHB, it can last for decades, lead to cirrhosis and raise the risk of developing HCC by a factor of 100 [19]. During the course of a CHB infection, there are three stages of viral replication: high, low and non-replicative. 15–25% of people with cirrhosis and HCC will die [20].CHB infection is considered to be prevalent in Iraq and many other developing nations [21].
Fulminant HBV Infection
Fulminant hepatitis B (FHB) is an uncommon illness that occurs in around 1% of cases; it is often deadly and is characterised by severe necrosis of liver tissue [19]. FHB may be caused by HBV genetic heterogeneity, co-infection or superinfection with other viral hepatitis agents, or host immunological variables [20]. When infected hepatocytes are destroyed and the consequence is deadly, a fast drop in Alanine transferase (ALT) and aspartate transferase (AST) in individuals with fulminant hepatic failure may be misinterpreted as resolving hepatic infection. FHB survivors are seldom chronically infected and HBsAg carriers almost always have no history of acute hepatitis.
Occult Hepatitis B
It is possible to diagnose occult (hidden) hepatitis B even in the absence of HBsAg by testing for the presence of HBV-DNA in the serum or liver [22]. Typically, the serum HBV-DNA level is less than 104 copies/ml. Patients with HCC, those with a history of HBV infection or chronic HCV, as well as those without serological signs, have all been reported to have occult HB [20]. The incidence of diagnosis relies on the relative sensitivity of HBV-DNA testing and the population prevalence of HBV infection. Overall, 5–55% of HBsAg-negative people with CHB infection and either HCC or HBV infection had positive serum HBV-DNA levels [13] In communities with substantial HBV exposure, patients with anti-HBc positivity but anti-HBs negativity have a prevalence of HBV-DNA that ranges from 7% to 60%[18]. The clinical relevance of latent HBV infection is unknown. Furthermore, a relationship has been shown between occult HBV infection and cryptogenic CH and HCC.
Transmission
HBV is mostly transmitted by percutaneous or mucosal contact with contaminated blood and bodily fluids such as saliva, menstrual, vaginal and seminal fluids, all of which have been identified as vehicles of human transmission. Sexual transmission of hepatitis B is possible, especially among unvaccinated males who engage in sex with other men and heterosexuals with several sexual partners or contact with sex workers. Less than 5% of instances of adult infection result in chronic hepatitis. Inadequately sterilised syringes and needles, intravenous and percutaneous drug abuse, tattooing, body piercing and acupuncture can all contribute to the spread of the virus. Accidental inoculation of minute quantities of blood or fluid during medical, surgical and dental procedures, as well as razors and other similar instruments contaminated with infectious blood, can all result in infection.
In many areas of the globe, notably in China and South East Asia, perinatal transmission is the primary route of HBV transmission and a significant element in sustaining the reservoir of the virus. A high percentage of viraemic women, particularly those who are seropositive for HBeAg, will infect their newborns during or soon after delivery if they are not given prophylaxis [23]. If the mother has acute hepatitis B during the second or third trimester of pregnancy or within two months after giving birth, the risk of infection for the infant rises. Even though HBV can infect the foetus while it is still in the womb, it doesn't seem to happen very often and is usually linked to antepartum haemorrhage and placental tears.Following prenatal infection (up to 6 months of age), the probability of chronic infection is 90%, although it falls to 20–60% between 6 months and 5 years of age [24].
Horizontal transmission, including "household, intrafamilial and particularly child-to-child transfer", is also crucial. In many endemic countries, at least fifty percent of childhood illnesses cannot be explained by mother-to-infant transmission.This was especially true before the introduction of neonatal immunizations, when the disease was most common in children between the ages of 7 and 14 [24].
Epidemiology of HBV Infection
HBV infection is a well-known and critical health issue that causes considerable morbidity and death globally, particularly in poorer nations [25]. WHO says that 2 billion people around the world have HBV infection and 450 million people are chronically infected. People who are chronically infected with HBV are more likely to get HDV infection [26]. Each year, more than one million individuals worldwide die owing to the complications of HBV infection. This issue is especially significant in Asia, Africa and the West Pacific, where HBV infection affects anywhere from 5% to 80% of the world's afflicted population [25]. High, moderate and low endemicity of hepatitis B virus infection may be distinguished over the globe [26].
High Endemicity
In regions where at least 8% of the population is CHB carrier, such as South East Asia, China, Sub-Saharan Africa and the Amazon Basin, hepatitis B is a widespread problem. In these regions, between 70 and 95% of the population has serological evidence of having HBV infection [27].
Most infections occur during infancy or childhood [25], because the predominate mode of transmission is prenatal [28]. Some of these countries change this situation very fast, such as China and Taiwan by using an effective immunization program, whereas in India, because of the absence of national immunization program it will become the largest HBV infection pool in the world [29].
Intermediate Endemicity
In the Middle East, Japan, South America, Eastern and Southern Europe and the Middle East, HBV is relatively endemic. Infection evidence is present in 10- 60% of the population and 2-7% of people are chronic carriers. AHB infection is frequent in these locations since different infections happen in teenagers and adults; nevertheless, infections in newborns and children sustain the high rates of chronic infection [27]. There are several transmission patterns, including transmission in infancy, early childhood and adults.
Low Endemicity
Most developed regions, including North America, Northern and Western Europe and Australia, have low HBV prevalence rates. Most HBV infections occur in high-risk teenagers and young adults, such as injectable drug users, healthcare workers and hemodialysis patients. In these places, 5-7% of the population has HBV and 0.5-2% are chronic carriers.
Prevalence of HBV Infection in Iraq
In the past, Iraq is considered as one of the intermediate endemic countries and many studies have been conducted since 1973; the results of these studies shows the prevalence of HBsAg in Al-Rusafa sector of Baghdad according to Iraqi CDC (Center for Disease Control and Prevention) from 2002 to 2008. Of the countries with which Iraq has frontiers, Turkey, KSA and UAE have an intermediate endemicity, while Iran, Kuwait and Bahrain are areas of a low endemicity [28]. In Iraq, between 3 and 4.5% of the general population and 2 to 2% of healthy blood donors are HBV carriers. HBsAg seroprevalence was found to be 1.6% in the general population and 1%-2% among Iraqi blood donors [30].
Age Distribution of HBV Infection
An important determinant of epidemiology of HBV is the age of acquisition of the virus. In areas with high endemicity, most infections occurs in children (4-8 years) and in area with intermediate endemicity the infection occur in adolescents and adults, while in areas with low endemicity, most infections occur in adolescents and young adults (15-29 years) [28]. In India, the number of people with HBsAg was detected to be highest after the age of 20 [29]. In Pakistan, the peak of HBsAg is seen in people aged 21 to 40 (high prevalence) [31].
Sex Distribution of HBV Infection
An epidemiological study done by Kramvis et al. showed a relatively higher prevalence of HBsAg among males than females in most countries. Once infected with HBV, males have a greater chance of maintaining a permanent infection compared to females, who are more likely to be infected momentarily and to generate anti-HBs antibodies. Additionally, males have a greater risk of becoming infected with HBV in the first place [27].These variations are most likely owing to a faster fall in HBsAg titer in females, resulting in a shorter carrier state duration [32]. Recently, most studies agreement with “Sobeslavsky” results with some exception, as that found in Dominican Republic, significantly higher in females [27] In Iraq, the normal population prevalence of HBsAg was found to be higher in males than females according to many studies [27].
Hepatitis B Indicators and their Relevance to Diagnostic Criteria
Serological testing is used to identify HBV infection by measuring a range of HBV-specific antigens and antibodies produced by the host in response to early HBV infection [33].
Hepatitis B Surface Antigen (HBs Ag)
Before symptoms occur, HBsAg is the first viral antigen found in the plasma of individuals with acute HBV infection [33]. The incubation period of the Hepatitis B Virus (Hepatitis B) is normally between 8 and 12 weeks (from HBV acquisition to the beginning of clinical symptoms) [34]
Hepatitis B surface antigen (HBsAg) is the first serologic marker to show and it may be identified in serum anywhere from 1 week to 12 weeks (on average, 30-60 days) after infection [35]. When symptoms first develop, the HBsAg rises and then it falls after about two to three months [34]. The apearence of HBV DNA virus in hepatocytes is shown by the detection of HBsAg in plasma. HBsAg testing is a sign of HBV infection. In general, having HBsAg for longer than six months indicates chronic HBV infection [36].Patients whose HBV infection has been cleared up do not have detectable levels of HBsAg [37].
One possible explanation for a negative HBsAg test in people with acute HBV infection is that the present assay cannot found very low levels of HBsAg or that HBsAg is neutralised by anti-HBs antibodies [35].
Hepatitis B e Antigen (HBe Ag)
HBeAg occurs one week after HBsAg is detected and it typically vanishes three weeks before HBsAg [33]. Patients who have HBeAg in their serum have a long-term HBV infection [34]. In general, the presence of HBeAg corresponds with a greater degree of infectiousness [33] Since the presence of HBeAg indicates that HBV is actively replicating, HBeAg-positive individuals pose a risk of transmitting the illness to others [36] If the mother is both HBsAg-positive and HBeAg-positive, the likelihood of perinatal HBV transmission is around 85-90% [37].
Hepatitis B Core Antigen (HBc Ag)
Infected hepatocytes are the only source of the intracellular antigen known as HBcAg. Plasma does not contain any detectable levels of HBcAg.Anti-HBc antibodies may be identified in hepatocyte samples collected after a liver biopsy owing to vaccination at the time of collection [34].
Total Hepatitis B Core Antibody (Total Anti-HBc)
The first antibodies are classed as IgM and IgG and they typically develop following the appearance of HBsAg [38]. About 8 weeks after HBV infection, antibodies to HBV core protein are the first ones that can be seen [37]. Anti-HBc IgM is identified early in the disease, indicating an active HBV infection, although Anti-HBc IgG emerges later and lasts longer [37]. In the convalescent phase after acute HBV infections, anti-HBc may continue for months to years, but in chronic HBV infections, it may persist for much longer [36]. Antibodies to HBcAg don't stop the virus from spreading and anti-HBc doesn't protect against getting HBV again [36].
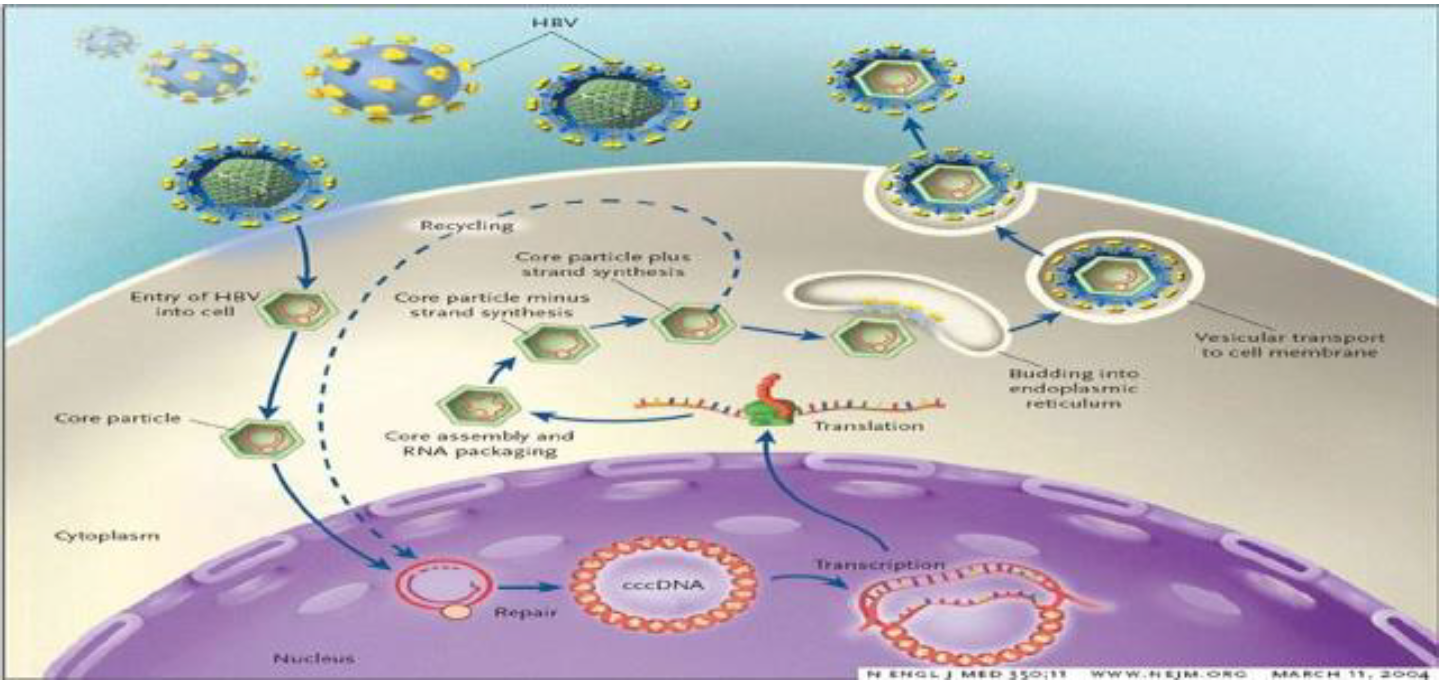
Figure 2: Hepatitis B Virus Cycle of Replication
Hepatitis B e Antibody (Anti -HBe)
In most cases, anti-HBe may be detected between 12 and 16 weeks, after HBeAg has stopped being produced [38] Anti-HBe cannot be detected until the majority of HBe antigens have been eliminated from the blood by the immune system. Generally, the existence of anti-HBe suggests a healthy immunological response to HBV infection [34].
Anti-HBs Ag
In most cases, HBsAg will be gone after three months of HBV infection, when anti-HBs antibodies have developed [36] After an infection with HBV has lasted for three months, anti-HBs antibodies will generally begin to emerge and at that point, HBsAg will no longer be present [37].The detection of anti-HBs may serve as an indication of successful treatment. Anti-HBs have a vital function in preventing HBV re-infection in patients; as a result, they are a necessary component in the production of HBV hyper-immune plasma [38]. When a person gets vaccinated against HBV, the only antibody that is present in their bloodstream is anti-HBs [34].
Hepatitis B DNA (HBV DNA)
HBV DNA is detectable relatively early after HBV infection (Figure 2) and typically implies viral replication [38]. The presence of HBV DNA in the bloodstream is clear proof of HBV infection. A quantitative HBV DNA test may be used as a measure of disease progression [36].
Prevention
Using safe blood supplies, modifying behaviour to reduce disease transmission, passive immune-prophylaxis for those who have been exposed to HBV and active immunisation are all methods that may be used to prevent HBV infection [39].
The decrease of HBV infection caused by blood transfusions has been attributed to the refusal of blood donors with risky behaviours and enhanced screening [40].Commonly, condom use during sexual activity is advised not just for HIV protection but also for HBV prevention. In addition to health education for the general public and a focus on high-risk populations, behaviour modification also include initiatives such as targeting high-risk groups. For persons who have been potentially exposed to Hepatitis B virus (HBV), Hepatitis B Immune Globulin (HBIG) administration is a passive immune-prophylaxis that may prevent infection [40]. Human plasma collected from donors with a history of high levels of antibodies to HBV is used to create HBIG.HBIG is indicated in four circumstances: newborns of HBV-infected mothers, following exposure to a contaminated needle, after sexual exposure and after liver transplantation [39]. For all newborns delivered to HBsAg-positive mothers, HBIG is advised as soon as possible after delivery or within 12 hours of birth, along with the recombinant HBV vaccination. It has been shown that up to 90% of pregnant women have protective levels of antibodies against perinatal HBV infection [40]. High-dose HBIG monotherapy may prevent HBV recurrence in 60% to 80% of individuals who have had a liver transplant [39].
HBV Therapy
Several factors must be considered while deciding how to treat HBV infection.
Status of HBV markers (HBsAg, HBeAg, anti-HBc, anti-HBc-IgM)
The quantity of HBV virus
Enzymes involved in hepatic function (alanine transaminase, or ALT and aspartate transaminase, or AST).Immune status of the infected patient
Cirrhosis of the liver is present
Because 90-95% of acute HBV infections in adults recover and gain immunity, acute hepatitis B infection may not always require therapy [41]. Children are far more susceptible to persistent infections. Up to 90% of young infants infected with the virus will be unable to eliminate it and will develop chronic illness. In the event that the acute infection is particularly severe, fulminant hepatitis will occur [42]. Currently, the U.S. Food and Drug Administration has licenced six antiviral medicines for chronic HBV therapy, including IFN-α, pegylated IFN-α, lamivudine, adefovir, dipivoxil, entecavir and telbivudine. IFN-α(and pegylated forms) is the only medicine capable of removing covalently closed circular DNA (cccDNA) from hepatocytes and is hence potentially therapeutic [41].
Dusheiko, G. et al. “Chronic Hepatitis B.” 2017.
Bogler, Y. et al. “Epidemiology and Natural History of Chronic Hepatitis B Virus Infection.” Hepatitis B Virus and Liver Disease, Springer, 2018, pp. 63–89.
Al-Hamdani, A.H. et al. “Retrospective Seroprevalence Study of Hepatitis B and C in Iraqi Population at Baghdad: A Hospital-Based Study.” Iraqi Journal of Community Medicine, vol. 3, 2012, pp. 186–190.
Hansi, N. et al. “Chronic Hepatitis B.” Liver Disease in Clinical Practice, Springer International Publishing, 2017, pp. 163–182.
Hemming, A.W. et al. “Hepatitis B and Hepatocellular Carcinoma.” Clinics in Liver Disease, vol. 20, no. 4, 2016, pp. 703–720.
Hui, C.K. and G.K. Lau. “Immune System and Hepatitis B Virus Infection.” Journal of Clinical Virology, vol. 34, 2005, pp. S44–S48.
Ott, J.J. et al. “Global Epidemiology of Hepatitis B Virus Infection: New Estimates of Age-Specific HBsAg Seroprevalence and Endemicity.” Vaccine, vol. 30, no. 12, 2012, pp. 2212–2219.
Zhang, X. et al. “Modulation of Hepatitis B Virus Replication and Hepatocyte Differentiation by MicroRNA-1.” Hepatology, vol. 53, no. 5, 2011, pp. 1476–1485.
Zoulim, F. and S. Locarnini. “Management of Treatment Failure in Chronic Hepatitis B.” Journal of Hepatology, vol. 56, 2012, pp. S112–S122.
Lai, C.L. and S. Locarnini. Human Virus Guides: Hepatitis B Virus. Vol. 1, International Medical Press, 2002.
Khaderi, S.A. and F.B. Hollinger. “Is the Risk of Death Enhanced in Immunosuppressed Hepatitis B Virus–Infected Patients Who Develop Acute Liver Failure?” Clinical Gastroenterology and Hepatology, vol. 15, no. 1, 2017, pp. 123–126.
Kumar, R. et al. “Development of Hepatocellular Carcinoma in Chronic Hepatitis B Patients with Advanced Fibrosis Is Independent of Viral Genotype.” Journal of Medical Virology, vol. 89, no. 5, 2017, pp. 845–848.
Cai, C.W. et al. “Hepatitis B Virus Replication Is Blocked by a 2-Hydroxyisoquinoline-1,3-Dione Inhibitor of Viral Ribonuclease H Activity.” Antiviral Research, vol. 108, 2014, pp. 48–55.
Kang, Y.B.A. et al. “Human Liver Sinusoid on a Chip for Hepatitis B Virus Replication Study.” Micromachines, vol. 8, no. 1, 2017, p. 27.
Nassal, M. “Hepatitis B Viruses: Reverse Transcription a Different Way.” Virus Research, vol. 134, no. 1, 2008, pp. 235–249.
Levrero, M. et al. “Control of cccDNA Function in Hepatitis B Virus Infection.” Journal of Hepatology, vol. 51, no. 3, 2009, pp. 581–592.
Nagpal, B. et al. “Seroprevalence of Hepatitis B Antigenemia among Dental Students in a Private South Indian Dental Institution.” International Journal of Research in Medical Sciences, vol. 3, no. 12, 2017, pp. 3543–3547.
Brousseau, N. et al. “Acute Hepatitis B Virus Infection with Delayed Appearance of Hepatitis B Core Antibody in an Immunocompromised Patient: A Case Report.” Journal of Medical Case Reports, vol. 11, no. 1, 2017, p. 111.
Hollinger, F.B. and T.J. Liang. “Hepatitis B Virus.” Fields Virology, vol. 4, 2001, pp. 2971–3036.
Gunardi, H. et al. “Hepatitis B Virus Infection in Children of HBV-Related Chronic Liver Disease Patients.” Hepatology International, vol. 11, no. 1, 2017, pp. 96–104.
Khalil, A.S. et al. “The Effectiveness of Post-Exposure Prophylaxis in Infants Born to Hepatitis B Virus Positive Mothers in the Kurdistan Region, Iraq.” International Journal of Infection, 2016.
Suspène, R. et al. “PCR-Mediated Recombination Impacts the Analysis of Hepatitis B Virus Covalently Closed Circular DNA.” Retrovirology, vol. 13, no. 1, 2016, p. 84.
MacLachlan, J.H. and B.C. Cowie. “Hepatitis B Virus Epidemiology.” Cold Spring Harbor Perspectives in Medicine, vol. 5, no. 5, 2015, article a021410.
McMahon, B.J. “Chronic Hepatitis B Virus Infection.” Medical Clinics of North America, vol. 98, no. 1, 2014, pp. 39–54.
Abdullah, R.A. et al. “Hepatitis B Knowledge among Healthy Volunteers in Duhok City, Kurdistan Region, Iraq.” International Journal of Infection, vol. 4, no. 4, 2017.
Abass, Y.A. et al. “Epidemiology of Hepatitis B and C at Thi-Qar Province, Iraq.” Al-Qadisiyah Medical Journal, vol. 4, no. 5, 2017, pp. 154–165.
Hussein, N.R. and S. Daniel. “A Study of Hepatitis B Virus–Associated Risk Factors in Patients Attending Hepatitis Unit in Duhok City, Iraq.” Archives of Clinical Infectious Diseases, 2017.
Al-Thwani, A.N. et al. “Evaluation of Hepatitis B Virus Vaccination among Children in Al-Diawynia City.” Al-Qadisiyah Medical Journal, vol. 4, no. 6, 2017, pp. 116–125.
Al-Saffar, O.B. and A.H. Ad’hiah. “Interferon Gamma: Gene Polymorphism and Serum Level in HBV and HCV Iraqi Patients.” Current Research in Microbiology and Biotechnology, vol. 6, no. 1, 2018, pp. 1400–1404.
Omer, A.R. et al. “Hepatitis B Virus.” Viral Hepatitis, edited by A.R. Omer and A. Al-Salmani, 1st ed., Iraqi Ministry of Health and WHO, 2005, pp. 11–15.
Alam, M.M. et al. “Serology-Based Disease Status of Pakistani Population Infected with Hepatitis B Virus.” BMC Infectious Diseases, vol. 7, no. 1, 2007, p. 64.
Hussein, N.R. et al. “Prevalence of Hepatitis B and C Viruses among Blood Donors Attending Blood Bank in Duhok, Kurdistan Region, Iraq.” International Journal of Infection, vol. 4, no. 1, 2017.
Price, H. et al. “Hepatitis B Serological Markers and Plasma DNA Concentrations.” AIDS, vol. 31, no. 8, 2017, p. 1109.
Towell, V. and B. Cowie. “Hepatitis B Serology.” Australian Family Physician, vol. 41, no. 4, 2012, p. 212.
Di Bisceglie, A.M. et al. “Determination of Hepatitis B Phenotype Using Biochemical and Serological Markers.” Journal of Viral Hepatitis, vol. 24, no. 4, 2017, pp. 320–329.
Maini, M.K. and A. Bertoletti. “HBV in 2016: Global and Immunotherapeutic Insights into Hepatitis B.” Nature Reviews Gastroenterology & Hepatology, 2017.
Bertoletti, A. and C. Ferrari. “Adaptive Immunity in HBV Infection.” Journal of Hepatology, vol. 64, no. 1, 2016, pp. S71–S83.
Giersch, K. et al. “Serum HBV pgRNA as a Clinical Marker for cccDNA Activity.” Journal of Hepatology, vol. 66, no. 2, 2017, pp. 460–462.
Kojuri, S.A. et al. “Detection of HBV Virus Nucleic Acid by Serological Methods.” IIOAB Journal, vol. 7, no. 8, 2016, pp. 36–41.
Colvin, H.M. and A.E. Mitchell. Hepatitis and Liver Cancer: A National Strategy for Prevention and Control of Hepatitis B and C. Institute of Medicine, 2010.
Triolo, M. et al. “Impact of HBV Therapy on the Incidence of Hepatocellular Carcinoma.” Liver International, vol. 34, suppl. 1, 2014, pp. 139–145.
Zoulim, F. et al. “Entecavir plus Tenofovir Combination Therapy for Chronic Hepatitis B in Patients with Previous Nucleos (t) ide Treatment Failure.” Hepatology International, vol. 10, no. 5, 2016, pp. 779–788.
