
+91 6002993949
submission@iarconsortium.org
Open Access
ISSN (Print) : 2709-3301
ISSN (Online) : 2709-331X
Introduction: Premedication involves administering medication to a patient before a surgical or invasive medical procedure. Managing postoperative pain and postoperative nausea and vomiting (PONV) remains a significant challenge in postoperative care, but is crucial for the early recovery and overall well-being of the patient after surgery. Methods: This study was conducted at the Department of Anesthesiology, Indira Gandhi Medical College and Hospital in Shimla, Himachal Pradesh, from April 2015 to November 2016.The patients were randomly assigned into three groups. Group I received placebo in the form of B-complex tablets. Group II received Cap Gabatin 300mg, and Group III received Tab Clonidine 0.2mg. Results: Mean age (in years) in Group I was 38.1±10.4, in Group II was 40.2±12. 2 and Group III was 39.1±12.5. Group-II patients were more sedated at time of induction than Group-I and Group-III. The level of sedation was significantly higher in Group-II at 0 and 6 hours post operatively p (0.0001). Variation in HR was found to be significant at 5 minutes post induction with less variation in HR in Group-III. In post operative analgesia the VAS score was significantly lower in Group-III. Conclusion: No adverse effect was noticed in above mentioned doses of gabapentin and clonidine. Thus, they can be used safely as premedicants.
Premedication involves administering medication to a patient before a surgical or invasive medical procedure [1]. Managing postoperative pain and postoperative nausea and vomiting (PONV) remains a significant challenge in postoperative care, but is crucial for the early recovery and overall well-being of the patient after surgery. The primary goal of premedication is to reduce patient anxiety and fear, which can lead to various physiological and psychological complications during and after the procedure [2]. In addition to reducing anxiety, premedication also helps in pain management, reduces postoperative nausea and vomiting (PONV), and facilitates the early mobilization and recovery of the surgical patient. Additionally, premedication also plays an essential role in pain management [3].
Gabapentin is an anticonvulsant that possesses anti-nociceptive and anti-hyperalgesic properties, making it effective in treating chronic neuropathic pain. Although traditionally thought to be unsuitable for acute perioperative conditions, recent studies have shown that its perioperative administration can effectively provide postoperative analgesia, preoperative anxiolysis, and prevent chronic post-surgical pain, postoperative nausea and vomiting, and delirium [4]. Clonidine (Catapresan) has been widely used as premedication for general anaesthesia, with significant experience in this area. This alpha 2-adrenoceptor agonist has central sympatholytic effects that can blunt the stress response to surgical stimuli, allowing for a reduction in narcotic and anaesthetic dosage. Additionally, preoperative application of clonidine can prevent perioperative myocardial ischemic events [5,6]. When administered orally at a dose of 1.5-2 µgm/kg body weight, clonidine can provide anxiolysis, sedation, and analgesia with stable hemodynamics and respiration, without the morphine-related side effects of nausea and vomiting. The etiology of postoperative nausea and vomiting (PONV) is multifaceted and depends on a variety of factors. Research indicates that approximately 53-72% of patients require antiemetic therapy after laparoscopic cholecystectomy. Given these factors, it is crucial to address the high level of anxiety experienced by many patients prior to this procedure through formal premedication. Therefore, the current study aims to compare and evaluate the effects of oral gabapentin and oral clonidine as premedication on the haemodynamic response, modulation of post-operative pain, and prevention of PONV in patients undergoing laparoscopic cholecystectomy.
Objectives
To compare the effects of oral gabapentin and oral clonidine as premedication on haemodynamic response, modulation of post-operative pain, prevention of postoperative nausea and vomiting (PONV), and patient satisfaction in patients undergoing laparoscopic cholecystectomy
To evaluate the impact of premedication or preoperative psychological care on the prevention and treatment of postoperative pain and PONV, as well as the promotion of early mobilization and well-being of the surgical patient
To assess the safety profile of oral gabapentin and oral clonidine as premedication in patients undergoing laparoscopic cholecystectomy
Study Area
This study was conducted at the Department of Anesthesiology, Indira Gandhi Medical College and Hospital in Shimla, Himachal Pradesh, from April 2015 to November 2016.
Study Design
The patients were randomly assigned into three groups using random allocation software, and the co-guide delivered drugs to the patients while maintaining a record in the computer. The investigators were blinded to the drugs used, and the drugs given to the patients were disclosed at the end of the study. The study included 75 patients of ASA 1 classification, aged 20-60 years of both genders, who were undergoing Laproscopic Cholecystectomy in the Operation theatres of I.G.M.C. & Hospital, Shimla, H.P. The patients were divided into three equal groups of 25 each.
Group I received placebo in the form of B-complex tablets (Cobadex Forte by GlaxoSmithKline Pharmaceuticals Ltd.).
Group II received Cap Gabatin 300mg (Gabatin 300 by Neon Laboratories Ltd.), and
Group III received Tab Clonidine 0.2mg (Aristo Pharmaceuticals Pvt. Ltd.)
Prior to the surgery, all patients underwent a general physical examination and routine investigations were conducted after being visited by medical personnel one day prior to the procedure. Consent for participation in the study was obtained from all patients. Random allocation software was used to assign the patients to one of the study groups. The patients were informed about the use of Visual Analog Scale (VAS) scoring during preoperative counseling. Premedication was administered to all patients in the three study groups, including 0.5mg Tab. Alprazolam (Tab. Alprex by Neon Laboratories Limited) at bedtime on the night before the surgery. Two hours before the surgery, premedication was given and baseline vitals were recorded, while patients were evaluated.
Statistical Analysis
The was entered and cleaned in MS excel spreadsheet. The data was analysed using SPSS v22. The quantitative data was expressed as mean and standard deviation, whereas the qualitative data was expressed in frequencies and proportions. Analysis of data among the groups was performed using one way analysis of variance test (ANOVA test). A p-value of less than 0.05 was considered to be statistically significant.
Observations And Results
Demographic Data: Mean age (in years) in Group I was 38.1±10.4, in Group II was 40.2±12. 2 and Group III was 39.1±12.5. Incidentally majority of patients in our study group were females. The ratio of female versus male in Group I was 19:6, in Group II was 16:9 and in Group III was 15:10. Mean weight (in Kilograms) in Group I was 52.9±7.7, in Group II was 57.4±11.7 and in Group III was 57.3±7.9. The demographic profile of patients in terms of age, body weight, male: female ratio was comparable in all the three study groups. There was no significant difference among the three groups (p>0.05) at the baseline.
Haemodynamic Variables
In the pre-anaesthetic unit patient’s baseline vitals (HR, SBP, DBP, MAP, SpO2) along with sedation score were recorded and premedication was given two hours before the surgery. Same parameters were again recorded before induction and post induction at 0-minute, 1 minute, 3 min, 5 min, 10 min and 30 min. As most of our surgeries lasted between 30 min to 40 min., so time period beyond 30 min was not taken into statistical analysis. Among the haemodynamic variables the variation in HR was found to be significant at 5 min post induction and SBP, DBP and MAP were found to be significant at 1 min, 3 min, and 5 min post induction intraoperatively. (p value <0.05). (Table 1).
In Gp-I the baseline HR at premedication was 76.8±11.4 and two hrs after premedication was 77.1±11.6. HR at 3 min and 5 min post induction in Gp-I was 87.6 ±16.3, 87.1±12.5 respectively (Range-77.1±11.4 to 87.1±12.5). In Gp-II The baseline HR at premedication was 77.6±10.1 and two hrs after premedication was 77.8±10.0. And 3 min and 5 min. post induction was 85.7±16.3, 85.1±14.9 respectively (range 77.6±10.1 to 85.1±14.9). In Gp-III the baseline HR at premedication was 78.3±11.4 and two after premedication is 79.1±11.4.
HR 3 min and 5 min post induction was 77.2±11.1, 78.0±12.3 respectively (range 78.3±11.4 to 78.0±12.3). In the inter group comparison of HR a significant difference was found in variation of HR at 3 min and 5 min post induction between Gp-I and GP-III with p value of 0.01 at both time intervals. Between GP-II and GP-III a significant difference was found at 3 min post induction with p value of 0.03 Between GP-I and GP-II no significant difference was found at any time interval. Thus, variation in HR from baseline is minimum in GP-III. Thus, no intubation response in terms of HR was observed in GP-III.
In GP-I the baseline SBP at premedication was 120.9±16.1 and two hrs after premedication was 120.1±16.7. SBP 1, 3, 5 Min post induction was 126.8±20.0, 131.1±22.3, 132.1±19.1 (range 120.9±16.1 to 132.1±19.1). In GP-II—The baseline SBP at premedication is120.8±17.3 and two hrs after premedication was 118.4±15.7, SBP AT 1, 3, 5 Min post induction is 131.1±18.1, 132.1±20.4, 129.9±22.6. 9. (range 120.8±17.3 to 129.9±22.6). In GP-III the baseline SBP at premedication was 120.5±18.6 and two after premedication was 118.3±14.4.SBP 1, 3, 5 min post induction was 118.0±14.4, 118.0±13.3, 116.4±12.3 respectively. (range 120.5±18.6 to 116.4±12.3).
Between group I and II the variation in SBP was not found to be significant at any time interval with p > 0.05. And between Gp I and III the variation in SBP was found to be significant at 3 min and 5 min post induction with p value of 0.01 and 0.001 respectively. Between GPII and GPIII the variation in SBP was found to be significant at 0min, 1min, 3 min,5 min post induction with p value of 0.04, 0.008, 0.005 and 0.01 respectively. Thus, change in SBP from baseline was minimum in GP-III. Hence no intubation response in terms of SBP was observed in GP-III. (p<0.01).
In GP-I the baseline DBP at premedication was 76.1±10.8 and two hrs after premedication was 77.2±10.5. DBP at 0 min, 1 min, 3 min and 5 min post induction were 78.3±9.5, 81.5±13.3, 81.4±11.7, and 83.2±12.2 (range-76.1±10.8 to 83.2±12.2). In GP-II DBP at premedication was 75.7±11.2 and two hrs after premedication was 76.5±10.4, DBP 0 min, 1 min, 3 min, 5 min post induction was 81.7±10.6, 82.4±10.2, 83.4±11.5, 80.7±13.9 respectively. (Range 75.7±11.2 to 80.7±13.9). In GP –III—DBP at premedication was 77.2±9.8 and two hrs after premedication was 76.5±9.6. DBP at 0min, 1min,3min and 5 min post induction was 78.3±9.4, 76.0±8.9, 77.7±8.8, 77.1±10.1 respectively, (range-77.2±9.8—77.1±10.1). Variation in DBP between Gp-I and Gp II was not found to be significant at any time interval with p value > 0.05. Between Gp I and Gp III DBP was found to be significant at 0 min post induction with p value of 0.0001. Between Gp II and Gp III, it was found to be significant at 1 min post induction with p value of 0.02. Thus, change in DBP from baseline was minimum in GP-III.
In GP-I baseline MAP at premedication was 91.0±11.7 and two hrs after premedication was 91.5±12.0. MAP at 0 min, 1 min, 3 min, 5 min post induction was 93.5±11.4, 96.6±15.0, 97.9±14.6, 99.5±13.9 respectively (range 91.0±11.7 to 99.5±13.9). In GP-II baseline MAP at premedication was 90.7±12.6 and two hrs after premedication was 90.4±11.1. MAP at 0 min, 1 min, 3 min, 5 min post induction was 91.3±12.5, 98.6±12.4, 95.3±21.6, 97.1±16.2 respectively (range 90.7±12.6 to 97.1±16.2). In GP-III baseline MAP at premedication is 91.6±11.8 and two hrs after premedication was 90.4±10.8. MAP at 0 min, 1 min, 3 min, 5 min post induction was 92.0±10.5, 89.9±10.2, 91.1±9.8, 90.1±10.2 respectively (range 91.6±11.8 to 90.1±10.2). Variation in MAP in GP-I and GP-II was not found to be significant at any time intervals. and in between GP-I and GP-III variation in MAP was found to be significant at 5 min post induction with p value of 0.009 between GP-II and GP-III MAP found to be significant at 1 min post induction with p value of 0.009.
The baseline hemodynamic variables (SBP, DBP, MAP and HR) were similar in all the three groups (p > 0.05). MAP had minimum variation in GP-III after laryngoscopy and tracheal intubation as compared to GP-I and GP-II. Minimum variation in MAP was seen at 1, 3 and 5 minutes after intubation in GP-III compared to GP-I and II. Hemodynamic variables were similar in GP-I and GP-II (p > 0.05).
No significant difference in spo2 was observed at any time interval between the three study groups (p value 0.91).
Table 1: Hemodynamic Variables of the Patients at Different Time Intervals
Variables | Group 1 (n = 25) | Group 2 (n = 25) | Group 3 (n = 25) | p value |
Heart Rate | 76.8±11.4 | 77.6±10.1 | 78.3±11.4 | 0.90 |
Before Induction | 77.1±11.6 | 77.8±10.0 | 79.1±11.4 | 0.81 |
Post Induction 30 minutes | 80.7±8.6 | 78.7±12.9 | 78.2±11.8 | 0.72 |
Systolic BP | 120.9±16.1 | 120.8±17.3 | 120.5±18.6 | 0.99 |
Before Induction | 120.1±16.7 | 118.4±15.7 | 118.3±14.4 | 0.89 |
Post Induction 30 minutes | 122.1±19.0 | 119.9±18.9 | 119.9±18.9 | 0.20 |
Diastolic BP | 76.1±10.8 | 75.7±11.2 | 77.2±9.8 | 0.87 |
Before Induction | 77.2±10.5 | 76.5±10.4 | 76.5±9.6 | 0.95 |
Post Induction 30 minutes | 91.7±14.9 | 90.3±13.9 | 91.3±10.7 | 0.92 |
Mean Arterial Pressure | 91.0±11.7 | 90.7±12.6 | 91.6±11.8 | 0.96 |
Before Induction | 91.5±12.0 | 90.4±11.1 | 90.4±10.8 | 0.92 |
Post Induction 30 minutes | 91.7±14.9 | 90.3±13.9 | 91.3±10.7 | 0.92 |
SPO2 | 93.2±2.3 | 93.1±1.4 | 99.6±0.6 | 0.88 |
Before Induction | 92.6±1.9 | 93.4±1.8 | 99.6±0.5 | 0.89 |
Post Induction 30 minutes | 93.8±1.7 | 93.8±1.5 | 99.4±0.7 | 0.91 |
Variation In Sedation Score Pre and Postoperatively
The level of sedation was measured using Sedation Score (0 = Alert, conversant, 1 = Awake but drowsy, 2 = Asleep but arousable, 3 = Asleep and not arousable.). And sedation score was taken before premedication and then two hrs after premedication at the time of induction and then 0 hrs, 6 hrs and 24 hrs postoperatively according to score given by American Society of Anaesthesia The baseline sedation score before premedication was comparable in all three groups (p>0.05).At time of induction in GP-I 12 patients (48%) had sedation score of 0 and 13 patients (52%) had sedation score of 1.In GP-II 9 patients (36%) had sedation score of 0 and 16 patients(64%) had sedation score of 1 at time of induction. In GP-III 13 patients (52%) had 0 sedation score and 12 patients (48%) had 1 sedation score at time of induction. The Sedation score was recorded post-operatively in the three groups when the patients were extubated and shifted to the recovery room. In GP-I 11 patients (44%) had sedation score of 1, 10 patients (40%) of 2 and 4 patients (16%) had 3 at 0 postoperative hours. In Gp-II sedation score of 0 and 1 was not present in any patient, sedation score of 2 in 11 patients (44%) and 3 in 14 patients (56%) 0 postoperative hours. In GP-III sedation score of 0 in 3 patients (12%), 1 in 18 patients (72%), 2 in 4 patients (16%) and sedation score of 3 was not present in any patient (0%) at 0 postoperative hours. Thus, the patients in GP-II were more sedated than GP-I and GP-III with p (<0.0002) at 0 postoperative hrs. Whereas sedation score at 6 hrs postoperatively in GP-I All 25 patients (100%) had sedation score 0, In GP-II- 24 patients (96%) had sedation score of 2 and 1 patient (4%) had sedation score of 1 at 6 hrs postoperatively. In GP-III 24 (96%) patients had sedation score of 0 and 1 (4%) patient had sedation score of 1 at 6 hrs postoperatively. Thus, in GP-II level of sedation was significant (p<0.001) as 96% (24 patients had sedation score of 2, and sedation score 24 hrs postoperatively in GP-I 25 (100%) patients had sedation score of 0, In GP-II 17 (68%) patients had sedation score of 0, and 8 (32%) patients had sedation score of 1 at 24 hrs postoperatively. In GP-III all 25 (100%) patients had sedation score of 0 at 24 hrs postoperatively. (p = 0.0001) There was a significant difference (p-value < 0.05) in sedation score in GP-I and GP-II at 0, 6, and 24 hrs postoperatively. Between GP-I and GP-III significant difference was observed only at one time interval that is 0 hrs postoperatively with p value of 0.01. Whereas in GP-II and GP-III a statistically significant difference was observed at 0, 6 and 24 hrs postoperatively with p value of <0.05. Thus, results showed that GP-II had maximum sedation among three study groups and GP-III had mild sedation and no sedation with Gp-I. Thus, in Gp-II patients were having high sedation score at induction and 0, 6 and 24 hrs postoperatively (Table 2).
Variation In Vas Score in Three Groups
Postoperative analgesia assessed in terms of intensity of pain, which was measured on basis of VAS score. Rescue analgesic given when patient had VAS score of 4 and more than 4. VAS score was measured at 0, 2, 3, 6, 12 and 24 hrs postoperatively. A highly significant difference was observed in VAS score in Gp-I and Gp-II at all the time intervals that was at 0, 2, 3, 6, 12 and 24 hrs post operatively with p value (< 0.05). A highly significant difference in VAS score was observed in Gp-I and Gp-III at 0, 2, 3, 12 and 24 hrs postoperatively with p value (<0.05). A highly statistically significant difference was observed in VAS score between Gp-II and Gp-III at all time intervals postoperatively with p value (< 0.05). It was observed that in GP-III more patients had VAS score <4 thus the quality of analgesia requiring rescue analgesic was better in GP-III. Whereas in GP-II the analgesic requirement was less than GP-I but higher than GP-III. The patients in GP-II were more sedated, hence this can explain lower VAS score obtained in first 24 hrs. Thus Gp-III had best post op analgesia among three study groups. Thus, patients in Gp-I had statistically more pain than Gp-II that is gabapentin group and GP-III that is clonidine group. And among Gp-II and Gp-III, Gp-III had better pain relief with less requirement of rescue analgesic. (p = 0.001) (Table 3).
Time Required for First Rescue Analgesic
Time required for rescue analgesic postoperatively was also observed. In GP-I, 10 patients required rescue analgesic at 2hr postoperatively (40%), 7 patients at 4hrs (28%), 5 patients at 3hrs (20%), 2 patients at6hrs (8%) and 1 patient at 5hrs (4%) postoperatively (Figure 1).
In GP-II, 9 patients (36%) did not require any rescue analgesic at all and 4 patients (16%) at 3hrs 7 patients at 6hrs (28%) and 5 patients at 12hrs (20%) postoperatively required rescue analgesic. In Gp-III 18 patients (72%) did not require any analgesic and 5 patients (20%) at 12hrs and 2 patients (8%) at 6hrs postoperatively required rescue analgesic. A statistically significant difference for the first rescue analgesic requirement occurred between three groups with p value of 0.001. Between GP-I and GP-II A statistically significant difference was found in first rescue analgesic requirement with p value of 0. 001.
Results were found significant between GP-I and GP-III with p value of 0.001. Between GP-II and GP-III results were found significant with p value of 0.01. Thus, the results showed that group 2 and 3 had good post op analgesia than group 1, And in between group 2 and 3, group 3 had good postoperative analgesia. (p = 0.01). In terms of average time required for first rescue analgesic in GP-I was 3.2 hrs and in GP-II was 7.8 hrs and in GP-III was 10.3 hrs. So, prolongation of first rescue analgesic requirement occurred in both GP-II and GP-III with maximum prolongation in GP-III.
Table 2: Variation of Sedation Score with Time in the Control and Case Group.
| Groups | Sedation Score 0 | Sedation Score 1 | Sedation Score 2 | Sedation Score 3 | p Value Inter-Group | p value |
| Sedation Score at Pre 1 | ||||||
Vit. B-complex (GP-I) | 20 | 5 | 0 | 0 | GP-I Vs GP-II = 0.14 GP-I Vs GP-III = 0.14 GP-II Vs GP-III = 0.15 | 0.78 |
GABA (GP-II) | 22 | 3 | 0 | 0 | ||
Clonidine (GP-III) | 22 | 3 | 0 | 0 | ||
| Sedation Score at Pre 2(Before induction) | ||||||
Vit. B-complex (GP-I) | 12 | 13 | 0 | 0 | GP-I Vs GP-II = 0.25 GP-I Vs GP-III = 0.77 GP-II VsGP-III = 0.39 | 0.49 |
GABA (GP-II) | 9 | 16 | 0 | 0 | ||
Clonidine (GP-III) | 13 | 12 | 0 | 0 | ||
2Vit. B-complex (GP-I) | 0 | 11 | 10 | 4 | GP-I Vs GP-II = 0.0002 GP-I Vs GP-III = 0.01 GP-II Vs GP-III = 0.0001 | 0.0001 |
GABA (GP-II) | 0 | 0 | 11 | 14 | ||
Clonidine (GP-III) | 3 | 18 | 4 | 0 | ||
ss | Sedation Score at 6 hrs (post op) | |||||
Vit. B-complex (GP-I) | 25 | 0 | 0 | 0 | GP-I Vs GP-II = 0.001 GP-I Vs GP-III = 0.31 GP-II Vs GP-III = 0.0001 | 0.0001 |
GABA (GP-II) | 0 | 1 | 24 | 0 | ||
Clonidine (GP-III) | 24 | 1 | 0 | 0 | ||
| Sedation Score at 24 hrs (post op) | ||||||
Vit. B-complex (GP-I) | 25 | 0 | 0 | 0 | GP-I Vs GP-II = 0.002 GP-I Vs GP-III = 1 GP-II Vs GP-III = 0.002 | 0.0001 |
GABA (GP-II) | 17 | 8 | 0 | 0 | ||
Clonidine (GP-III) | 25 | 0 | 0 | 0 | ||
Table 3: Variation of VAS Score with Time in Control and Case Group
Group | VAS 0 | VAS 1 | VAS 2 | VAS 3 | VAS 4 | VAS 5 | VAS 6 | VAS 7 | P Value Inter-Group | p value |
VAS 0 hr(postop) | ||||||||||
Vit. B-comp. (GP-I) | 4 | 5 | 10 | 3 | 2 | 1 | 0 | 0 | GP-I Vs GP-II = 0.0002 GP-I Vs GP-III = 0.007 GP-II Vs GP-III = 0.0001 | 0.001 |
GABA (GP-II) | 15 | 10 | 0 | 0 | 0 | 0 | 0 | 0 | ||
Clonidine (GP-III) | 0 | 5 | 11 | 9 | 0 | 0 | 0 | 0 | ||
VAS 2 hr(postop) | ||||||||||
Vit. B-comp. (GP-I) | 0 | 3 | 4 | 8 | 6 | 0 | 3 | 1 | GP-I Vs GP-II = 0.0003 GP-I Vs GP-III = 0.001 GP-II Vs GP-III = 0.004 | 0.001 |
GABA (GP-II) | 9 | 0 | 8 | 8 | 0 | 0 | 0 | 0 | ||
Clonidine (GP-III) | 0 | 2 | 15 | 8 | 0 | 0 | 0 | 0 | ||
VAS 3 hrs(postop) | ||||||||||
Vit. B-comp. (GP-I) | 0 | 2 | 9 | 9 | 0 | 4 | 0 | 1 | GP-I Vs GP-II = 0.0008 GP-I Vs GP-III = 0.0003 GP-II Vs GP-III = 0.002 | 0.001 |
GABA (GP-II) | 4 | 1 | 4 | 12 | 4 | 0 | 0 | 0 | ||
Clonidine (GP-III) | 0 | 6 | 8 | 11 | 0 | 0 | 0 | 0 | ||
VAS 6 hrs(postop) | ||||||||||
Vit. B-comp. (GP-I) | 0 | 6 | 11 | 6 | 2 | 0 | 0 | 0 | GP-I Vs GP-II = 0.0037 GP-I Vs GP-III = 0.15 GP-II Vs GP-III = 0.003 | 0.001 |
GABA (GP-II) | 7 | 1 | 4 | 6 | 5 | 2 | 0 | 0 | ||
Clonidine (GP-III) | 0 | 3 | 11 | 9 | 2 | 0 | 0 | 0 | ||
V AS12 hrs(postop) | ||||||||||
Vit. B-comp. (GP-I) | 1 | 3 | 10 | 11 | 0 | 0 | 0 | 0 | GP-I Vs GP-II = 0.03 GP-I Vs GP-III = 0.009 GP-II Vs GP-III = 0.004 | 0.001 |
GABA (GP-II) | 8 | 4 | 4 | 4 | 3 | 2 | 0 | 0 | ||
Clonidine (GP-III) | 0 | 11 | 8 | 1 | 5 | 0 | 0 | 0 | ||
VAS 24 hr (postop) | ||||||||||
Vit. B-comp. (GP-I) | 0 | 4 | 14 | 3 | 4 | 0 | 0 | 0 | GP-I Vs GP-II = 0.0002 GP-I Vs GP-III = 0.0004 GP-II Vs GP-III = 0.0001 | 0.001 |
GABA (GP-II) | 14 | 4 | 3 | 1 | 3 | 0 | 0 | 0 | ||
Clonidine (GP-III) | 0 | 18 | 7 | 0 | 0 | 0 | 0 | 0 | ||
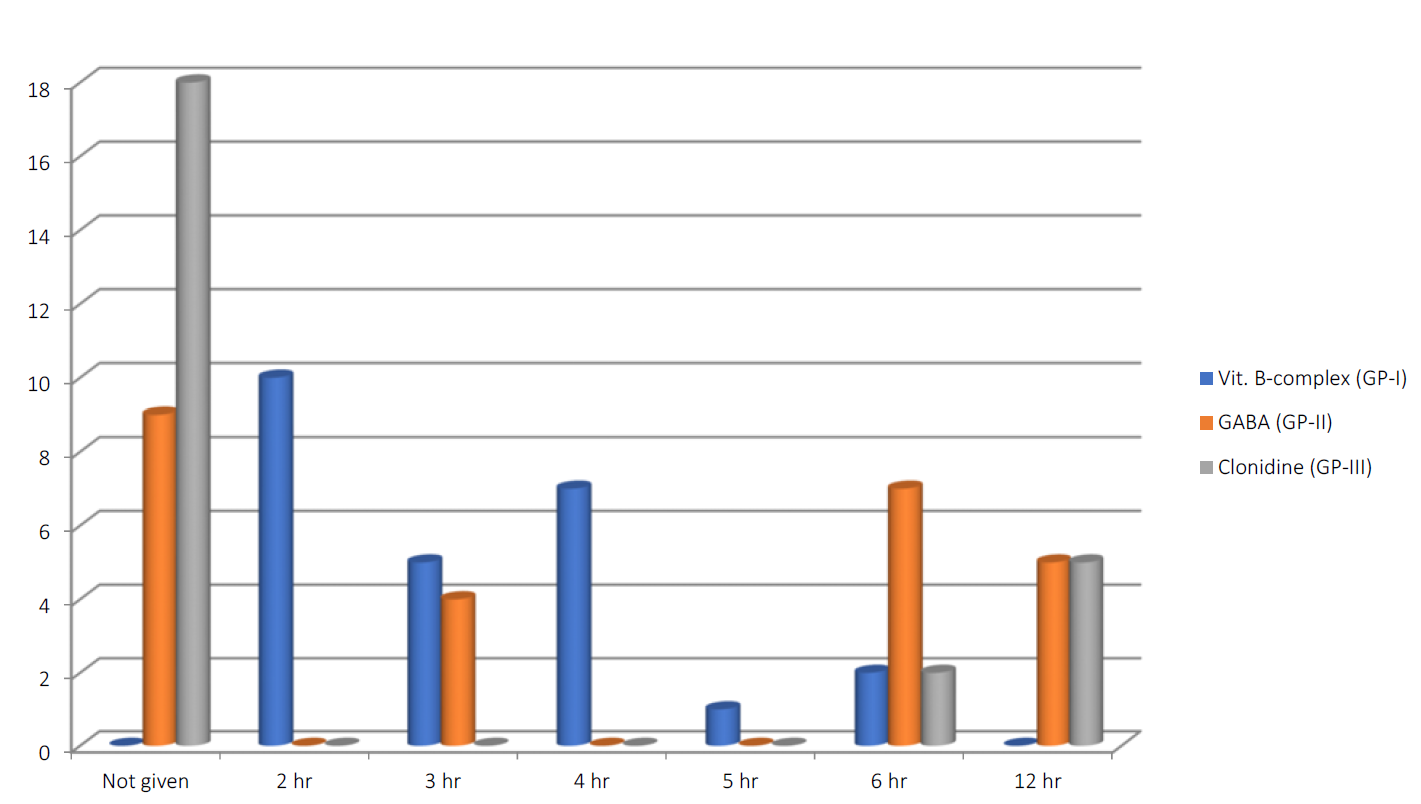
Figure 1: Time Required for Rescue Analgesia
(X-AXIS showing time in hrs at which first rescue analgesic was given and Y-AXIS showing no. of patients, Nil showing to which no rescue analgesic given at all.)
Total Analgesic Requirement
There was significant reduction in requirement of total analgesic dose (Inj. Diclofenac Sodium) occurred within 24 hours in both the Gp-II and Gp-III. (p=0.001) In GP-I, 10 patients (40%) required 3 doses, 6 patients (24%) required 4 doses and 4 patients (16%) required 5 and 2 doses respectively and 1 patient (4%) required 6 doses in first 24 hrs. In GP-II, 9 patients required no analgesia (36%), 10 patients required only 1 dose of analgesic (40%), 2 doses of analgesic required in 4 patients (16%) and 3 doses of analgesic required in 2 patients (8%). In GP-III, 18 patients (72%) required no analgesia and 7 patients (28%) required only single dose of analgesic in 24 hrs. A significant difference occurred in total analgesic requirement in 3 groups both between group 1 and II with p value of 0.0001, group 1 and III with p value of 0.0001 and a significant difference occur between group II and III with p value of 0.02 (<0.05). Total analgesic requirement is lowest in group III as compare to group 1 and II. In between group 1 and, group II had less analgesic requirement.
Variation Of Ponv with Time
PONV was assessed on basis of PONV score with score 0-no nausea, score 1-nausea, score 2-retching, score 3-vomiting. Variation in PONV score was assessed at 0, 6, 12 and 24 hrs postoperatively. A significant difference in PONV score was observed at 0 hrs in Gp-I and Gp- II with p value of 0.01 Between Gp-I and Gp-III at 0 and 6 hrs postoperatively with p value of 0.002 and 0.004. Between Gp-II and Gp-III a significant difference in variation in PONV score was found 6 hrs postoperative with p value of 0.01 (<0.05) and p = 0.004 between GPI and GPIII. Thus, results showed that Gp-II and Gp-III had a role in preventing PONV. No significant difference in variation in PONV was seen between three study groups at 12 and 24 hrs postoperatively with p value > 0.05.
Quality of PONV in three study groups in 24 hrs
Among three study groups in GP-I 68% of patients had retching and vomiting in 24 hrs. Whereas quality of PONV in GP-II and GP-III is comparable as 20% patients in GP-II and 16% of patients in GP-III had retching in 24 hrs and none of patients had vomiting in 24 hrs.
Preoperative anxiety and stress are common among patients awaiting surgical procedures and may lead to increased requirements of anesthetic induction agents and postoperative analgesic drugs. Anxiety causes various signs of sympathetic stimulation and stress, such as tachycardia, elevated systolic blood pressure, pale and sweaty skin, constricted veins, and ventricular ectopic beats or even ventricular fibrillation [7,8]. Such anxiety is also associated with a slower and more complicated postoperative recovery. Therefore, oral premedication using a combination of gabapentin and clonidine, which provides sedation, analgesia, and anxiolysis in a single dose, may offer a viable option to reduce preoperative anxiety and improve the overall outcome of anesthesia and surgery.
Effect of Oral Premedication with Gabapentin and Clonidine on Sedation
In our study we premedicated Gp-I patients with B-complex tab, and Gp-II patients with 300mg of gabapentin tab. and Gp-III patients with 0.2mg clonidine tab two hrs before operation. The level of sedation between three groups were measured using Sedation Score. In our study, in Gp-II that is gabapentin group patients were more sedated postoperatively with sedation score of 2 and 3 postoperative as compared to clonidine with mild arousable sedation with sedation score of 0 and 1 postoperatively.
Trevor Sequeira [9] and Upadya Madhusudan et al. [10] in their study compared oral midazolam (0.5 mg/kg) 30 minute before induction versus oral clonidine (4 μg /kg) 90 minute before induction as a premedication in pediatric patients aged between 2-12 years with regard to sedation and anxiolysis.
In our study the most of the patient were in sedation score 0, 1 and 2 as compared to their study in which the sedation score was 3 and 4.The higher sedation score in their study may be due to age group as all the patients were children less than 12 years as compared to our study in which all the patients were adult and also dose of clonidine used is different than that we used in our study.
Our study is also in concordance with the study of Syal K et al. [11] which is a comparative study of Acetaminophen, gabapentin and combination of acetaminophen and gabapentin on postoperative analgesia in patients undergoing open cholecystectomy under GA.
In their study sedation was discovered to be major drawback due to consumption of gabapentin. A significantly high number of patients (100%) in Gp-III and Gp-IV who consumed gabapentin had sedation of level of 4, 5 in comparison to 65.52% patients in Gp-I and 73.33% patients in Gp-II, who did not consume gabapentin, as in our study 96% of patients in Gp-II had higher sedation score postoperatively at 6 hrs. Same results obtained may be due to similar type of surgery and similar age group of patients.
Haemodynamic Variables
In our study in all the three groups baseline haemodynamic variables at premedication were comparable. And haemodynamic variables like (HR, SBP, DBP and MAP) again observed at induction and at 0,1,3,5,10,30 min post induction [12].
In our study GP-III i.e. clonidine had minimum variation in HR, SBP, DBP and MAP from baseline as compared to Gp-I and Gp-II concluding that clonidine obtunds haemodynamic changes during intubation in laparoscopic cholecystectomy. Our study was in concordance with study of Minroy Das et al. [13], in which they studied the effect of clonidine premedication on haemodynamic changes during laparoscopic cholecystectomy. They divided 60 ASA-1 and ASA-II patients into two groups, 30 patients received tab clonidine 150 mcg and other 30 patients received tab ranitidine 150 mg 90 min before induction. Significant increase in HR, SBP, DBP, MAP had been observed in ranitidine group from baseline as compared to clonidine group. Thus, clonidine obtunds intubation response and causes minimum variation in hemodynamic parameters in laparoscopic cholecystectomy.
Postoperative Analgesia
Our study was in accordance with the study by Singh Shivinder and Arora Kapil [14] who studied effect of oral clonidine premedication on perioperative haemodynamic response and post op analgesia requirement for patients undergoing laproscopic cholecystectomy. In their study 50 patients were divided into two groups, group I received oral clonidine 150mcg and group II received placebo 90 min. prior to induction. Pain intensity was assessed on VAS score. In their study total analgesic requirement was significantly reduced in clonidine group as compared to placebo [15]. Our study was also in accordance with the study by Baghel Hansraj et al. [16] which was comparative study of single dose pre-emptive gabapentin vs clonidine for postoperative pain relief in lower limb surgeries under spinal anesthesia. In their study total analgesic requirement was less in GP-C, which is again similar to our study in which Total analgesic requirement is again less in GP-III that is clonidine group.
Variation in PONV
Our study was in accordance with study by Ajori et al. [17] and Pandey et al. [18]. Ajori et al in their study had 64% of patients had PONV score 0 in first 6 hrs while in our study 60% of patients had 0 PONV score in Gabapentin group in first 6 hrs. None of patients had nausea and vomiting at 12 hrs in gabapentin group in both the studies. Pandey et al. [19] reported gabapentin 600mg to be more effective in controlling PONV but had not mentioned the exact PONV score. In most of studies the exact PONV score had not been mentioned they had given combined scores and nature of surgery was also different. Hence our study was not in accordance with the studies done by Shreeraghu et al, Mohammadi S.S. et al. [20]and Morashi S.M. et al. [21] Shreeraghu et al. [22] had reported 3.3% incidence of PONV in clonidine group as compared to 20% in control group in postoperative period but they had not mentioned the exact time of nausea and vomiting in their study.
Our study was not in accordance with the study of Mohammadi S.S. et al. [23] They observed lesser incidence of PONV in recovery room in first 6 hrs. Although no statistically significant difference was observed. None of their patients in clonidine group had PONV. The difference could be because they had not mentioned the PONV score in their study and type of surgery was also different as it was any elective abdominal surgery.
Group-II patients were more sedated at time of induction than Group-I and Group-III. The level of sedation was significantly higher in Group-II at 0 and 6 hours post operatively p (0.0001). Variation in HR was found to be significant at 5 minutes post induction with less variation in HR in Group-III as compared to Group-I and Group-II. Variation in SBP, DBP and MAP were found to be significant at 1-, 3- and 5-minutes post induction intraoperatively with less variation in Group-III than Group-I and Group-II thus Group-III had a role in attenuation of hemodynamic response to laryngoscopy whereas Group-I and Group-II did not cause any attenuation of hemodynamic response to intubation. In post operative analgesia the VAS score was significantly lower in Group-III and both Group-II and Group-III had better post operative analgesia than Group-I. The time of 1st rescue analgesic was prolonged in both Group-II and Group-III but was more prolonged in Group-III. Total analgesic requirement within 24 hours was less in Group-II and Group-III but Group-III had fewer requirements as compared to Group-II. Thus Group-III i.e. clonidine group was proved to be the best for post operative analgesia among three groups. Group-I had no role in post operative analgesia. PONV was assessed on the basis of PONV score 0, 6, 12 and 24 hours post operatively. The results showed that Group-II and Group-III had role in preventing PONV. Between GP-II and GPIII in preventing PONV results were comparable with no statistically significant difference with p value 0.39 at 0 hrs postoperatively. But at 6 hrs postoperatively a statistically significant difference was observed between GP-II and GP-III in preventing PONV with p value of 0.01. Thus Group-I had no role in prevention of PONV. In GP-II and GP-III results were comparable in prevention of PONV and No significant difference in variation in PONV was seen between three study groups at 12 and 24 hours post operatively. No adverse effect was noticed in above mentioned doses of gabapentin and clonidine. Thus, they can be used safely as Premedicants.
Mitchell, M. “Patient anxiety and modern elective surgery: A literature review.” Journal of Clinical Nursing, vol. 12, no. 6, October 2003, pp. 806–815.
Maranets, I. and Z.N. Kain. “Preoperative anxiety and intraoperative anesthetic requirements.” Anesthesia & Analgesia, vol. 89, no. 6, December 1999, pp. 1346–1351.
Mohammadi, S.S. and M. Seyedi. “Comparing oral gabapentin versus clonidine as premedication on early postoperative pain, nausea and vomiting after general Anesthesia.” International Journal of Pharmacology, vol. 4, 2008, pp. 153–156.
Mohammadi, S.S. and M. Seyedi. “Comparing oral gabapentin versus clonidine as premedication on early postoperative pain, nausea and vomiting following general Anesthesia.” Saudi Journal of Anaesthesia, vol. 3, no. 1, July 2009, pp. 25–28.
Studer, F.R. et al. “Comparison of clonidine and midazolam as anxiolytic premedication before wisdom tooth surgery: A randomized, double-blind, crossover pilot study.” Oral and Maxillofacial Surgery, vol. 16, 2012, pp. 341–347.
Lee, S.Y. et al. “hemodynamic effects of topical lidocaine on the laryngoscope blade and trachea during endotracheal intubation: A prospective, double-blind, randomized study.” Journal of Anesthesia, vol. 28, 2014, pp. 668–675.
Trevor, S. et al. “A comparison of midazolam and clonidine as an oral premedication in pediatric patients.” Saudi Journal of Anaesthesia, vol. 6, 2012, pp. 8–11.
Mohamed Ali, H.S. et al. “A comparative study of clonidine and magnesium sulfate premedication on perioperative hormonal stress responses, hemodynamic stability and postoperative analgesia in patients with gallbladder diseases undergoing laparoscopic cholecystectomy.” Egyptian Journal of Anaesthesia, vol. 38, 2022, pp. 108–115.
Syal, K. et al. “‘Protective premedication’: A comparative study of acetaminophen, gabapentin and combination of acetaminophen with gabapentin for postoperative analgesia.” Journal of Anaesthesiology Clinical Pharmacology, vol. 26, no. 4, October 2010, pp. 531–536.
Weissman, C. “The metabolic response to stress: An overview and update.” Anesthesiology, vol. 73, no. 2, August 1990, pp. 308–327.
Gold, M.S. et al. “The effect of lumbar epidural and general anesthesia on plasma catecholamines and hemodynamics during abdominal aortic aneurysm repair.” Anesthesia & Analgesia, vol. 78, 1994, pp. 225–230.
Barber, N. and M.C. Blunt. “Principles of anaesthesia: premedication.” Surgery (Oxford), vol. 20, 2002, pp. 58–60.
Belhoula, M. et al. “Clonidine premedication improves metabolic control in type 2 diabetic patients during ophthalmic surgery.” British Journal of Anaesthesia, vol. 90, 2003, pp. 434–439.
Bafna, U. et al. “A comparison of different doses of gabapentin to attenuate the haemodynamic response to laryngoscopy and tracheal intubation in normotensive patients.” Journal of Anaesthesiology Clinical Pharmacology, vol. 27, no. 1, January–March 2011, pp. 43–46.
Richens, A. “Clinical pharmacokinetics of gabapentin.” New Trends in Epilepsy Management: The Role of Gabapentin, edited by D. Chadwick, Royal Society of Medicine, 1993, pp. 41–46.
Rose, M.A. and P.C.A. Kam. “Gabapentin: Pharmacology and its use in pain management.” Anaesthesia, vol. 57, 2002, pp. 451–462.
Pandey, C.K. et al. “Prophylactic gabapentin for prevention of postoperative nausea and vomiting in patients undergoing laparoscopic cholecystectomy: A randomized double-blinded placebo-controlled study.” Journal of Postgraduate Medicine, vol. 52, no. 2, 2006, pp. 97–101.
Kulkarni, P. et al. “Pre-operative sedation using oral clonidine and oral gabapentin: A comparative study.” Journal of Evidence Based Medicine and Healthcare, vol. 1, no. 13, December 2014, pp. 2349–2569.
Gupta, K. et al. “Premedication with clonidine versus fentanyl for intraoperative hemodynamic stability and recovery outcome during laparoscopic cholecystectomy under general anesthesia.” Anesthesia Essays and Researches, vol. 7, 2013, p. 29.
Patil, R. et al. “Effect of preemptive clonidine on intraoperative isoflurane requirement, hemodynamic stability and postoperative analgesia in patients undergoing laparoscopic cholecystectomy.” Journal of Evidence Based Medicine and Healthcare, vol. 1, no. 15, December 2014, pp. 1866–1873.
Taheri, A. et al. “The effect of oral clonidine premedication on nausea and vomiting after ear surgery.” Middle East Journal of Anesthesiology, vol. 20, 2010, pp. 691–694.
Mark, M. “Patient anxiety and modern elective surgery: A literature review.” Journal of Clinical Nursing, vol. 12, no. 6, October 2003, pp. 806–815.
Mohammadi, S.S. and M. Seyedi. “Comparing oral gabapentin versus clonidine as premedication on early postoperative pain, nausea and vomiting after general anesthesia.” International Journal of Pharmacology, vol. 4, 2008, pp. 153–156.
