
+91 6002993949
submission@iarconsortium.org
Open Access
ISSN (Print) : 2709-3301
ISSN (Online) : 2709-331X
Introduction: Streptococcus pyogenes is one of the common causes of pharyngo-tonsillar infections of childhood. The infection does not limit to pharyngeal infections only, rather affects vital organs to develop different conditions like acute glomerulonephritis, Rheumatic Heart Disease (RHD), toxic shock syndrome, generalized sepsis, necrotizing fasciitis etc. Its ever increasing virulence due to frequent mutations makes it a prime cause of infant mortality throughout the globe. Gradual emergence of antibiotic resistance has become a new contributing factor to increased burden of streptococcal diseases. Methods: In this experiment some commonly prescribed homeopathic medicines were studied to find out their efficacy against S. pyogenes. In this experiment, the Growth Inhibition Zones (GIZ) of different homeopathic medicines in three different potencies were measured against S. pyogenes. Results: The results of the experiment revealed that the medicines are significantly effective against the bacterial strain and 30CH potency of Belladonna, Mercurius, Solublis, Ferrum Phosphoricum, Lycopodium Clavatum, Lachesis (arranged in decreasing order of GIZ) can inhibit growth of S pyogenes. Conclusion: This experiment clearly showed that homoeopathic medicines have antibacterial property against S. pyogenes and this important finding may be utilized in direct or supplementary treatment of S. pyogenes infection in future.
S. pyogenes, a beta haemolytic streptococcus, is also known as Group A Streptococcus (GAS). It is an important human pathogen known for centuries and can cause a diverse spectrum of diseases [1]. Wide variety of streptococcal infections evident in humans are ranging from mild skin and upper respiratory tract infections to severe life-threatening conditions such as septicaemia, pneumonia and streptococcal toxic shock syndrome. Around 15-30% cases of GAS pharyngitis has associated with peoples of low socioeconomic group and poverty [1-3]. In a small minority of patients (0.3–3%), untreated GAS pharyngitis may trigger autoimmune diseases, including acute poststreptococcal glomerulonephritis, acute rheumatic fever and rheumatic heart diseases, that still remains one of the most important public health problems in low- and middle-income countries [4]. Streptococcal sore throat occurs through respiratory droplets, as indirect or direct contact and the incubation period is one to three days. The commonest presentations are in the form of redness, soreness and oedematous condition of throat, accompanied by submandibular and submental lymphadenitis [5,6]. A broad-spectrum review on the GAS diseases was published in 2011, showing 18.1 million people were suffering from it during that time, with an additional 1.78 million incident cases occurring each year. The exact cases of S. pyogenes sore throat are much greater than the other serious GAS diseases and about 616 million each year. In India, GAS sore throat is prevalent in 4.2% to 13.7% of the children population; however, asymptomatic carriage of GAS is about 11.2%-34% in different parts of India [7-10]. In conventional medicine, the treatment guidelines for GAS sore throat are conflicting and it differs from one country to other. Most of the guidelines recommend the administration of antibiotics in GAS culture positive sore throat cases, on the other hand many high-income countries, like United Kingdom, Belgium and the Netherlands discourages the extensive use of antibiotics in such cases. But it is a common medical practice to administer antibiotics chiefly to reduce the symptoms and disease duration, irrespective of the patient’s other complications [11-14]. This common attitude of prescribing antibiotics has led us today to the present era of antibiotic resistance. Emergence and dissemination of resistant microbes has increased mortality, prolonged hospital days and exceeded medical cost. Nearly 700,000 people die from antimicrobial resistance per year and according to a study another 10 million people projected to die from it by 2050. In this scenario, the homoeopathic system of medicine can be the effective solution and it can help to reduce the use of antibiotics [15-19]. A review article, published in 2018 on homoeopathic prospects on Upper Respiratory Tract Infection (URTI) showed definite therapeutic opportunities of homoeopathic medicine in antimicrobial resistant URTI, but there were fewer studies on pharyngitis or sore throat in particular and the studies lacked in replicability and reproducibility [20].
Different species of Streptococcus which have been invented so far, possess a common affinity towards warm blooded mammals. Though GAS is an external pathogen causing infections in the human body, but recent studies have shown both in vivo and in vitro evidence of the bacterium. Bacterial pathogen usually has various strategies for binding with their target (extra cellular matrix mainly). In case of streptococcal infection adherence and internalization of the bacteria plays key role behind virulence and pathogenicity. Fibronectin binding proteins F1 and F2 helps the organism to attach with the epithelial cells and are the most important factors associated with the virulence. Following adhesion, internalization depends on reaction between S. pyogenes fibronectin binding protein (SfbI = F1) with fibronectin present over epithelial cell surface [21]. Blocking binding of SfbI domain can reduce adherence and internalization of the organism. Along with that M protein which is chiefly present in GAS plays vital role to escape the host immune response. Till date more than 150 different types of M proteins and other proteins with much structural similarity with this protein have been recognized [22]. Several studies have shown different nature of interaction of M protein with different human plasminogen, immunoglobulin [23-27] protein has been recognized. This protein shares epitopes with few host proteins like cardiac and skeletal tropomyosin, laminin, keratin etc. The hypervariability of M protein helps it to bind with C4bp and escapes phagocytosis by causing alteration of the classical complement pathway [28,29]. M protein also causes resistance to phagocytosis by binding to fibronectin via B repeat region [30]. The hypervariability is also responsible for antibiotic resistance in GAS diseases. In children (53%) and asymptomatic carriers (80%) presence of pfbp I gene has been demonstrated and their association with macrolide resistance was observed as well [31]. Drug resistance and everchanging variability of the bacteria and its promiscuous reactive nature creates a mystery and make it difficult to control. Along with that asymptomatic carriers are present in a large group of reservoirs make eradication impossible. Therefore, in this in vitro study our main aim was to see whether homeopathic medicines may have anti-bacterial activity on S. pyogenes.
Materials
Selection of Bacteria: International strain of Group A Streptococcus pyogenes (ATCC 12384) was taken which was highly susceptible to antibiotics when tested by sensitivity tests. A pure culture of the bacteria on blood agar plate was used.
Culture Medium
Mueller Hinton Agar (MHA) was prepared in Petri dishes. For study with medicines MHA plates were used because blood present in blood agar plate can alter the efficacy of the medicines. Moreover, S. pyogenes grows well on MHA.
Sensitivity Disc
Discs of 6mm diameter of Whatman filter paper no.41 of round shapes were cut and sterilized in autoclave at 1210C, 0.02 ml of medicine was used per disc. Similarly 0.02 ml of ethanol was used as control as the drugs contained ethanol as vehicle.
Measuring Scale
Sensitivity measuring scale (Hi Media) with millimetre marking was used to measure Growth Inhibition Zone (GIZ).
Table 1: Showing Selected Homeopathic Medicines and Their Respective Potencies
| HOMOEOPATHIC MEDICINES | POTENCY | ||
| Belladonna | 6CH | 30CH | 200CH |
| Mercurius solubilis | 6CH | 30CH | 200CH |
| Lachesis | 6CH | 30CH | 200CH |
| Ferrum phosphoricum | 6CH | 30CH | 200CH |
| Lycopodium clavatum | 6CH | 30CH | 200CH |
Selection Homoeopathic Medicines
The medicines selected are mentioned in different repertories under section of inflammation and these medicines are most commonly used by clinicians for ages for inflammatory diseases with considerable efficacy (Table 1). Medicines were procured from Willmar Schwabe India Pvt. Ltd, a GMP certified company, all the medicines are included in HPI (Homoeopathic Pharmacopoeia of India). Three most commonly used potencies i.e. 6th, 30th and 200th potency of centesimal scale were used in this experiment.
Methods
Seven MHA plates were taken in each lot, out of which 6 were radially divided into 5 sectors, one for each medicine; and the 7th plate served as control. Then MHA plates were inoculated with the bacteria as lawn culture and were kept at room temperature for 5 to 10 minutes to dry the medium. Then homoeopathic drug sensitivity discs were taken with the help of sterile forceps and carefully placed on the surface of medium so that complete contact was made. Plates were placed in the incubator at 350 –370C and left undisturbed for 24 hours. After 24 hours, diameter of the Growth Inhibition Zone (GIZ) was measured with the help of GIZ measuring scale. We repeated the experiment for three consecutive times to minimize the error.
Statistical Methods
Three-way ANOVA and paired t test were done to detect significance of statistical differences between the potencies in formation of GIZ.
Zone of sensitivity was observed in all the plates. The results were however different with different medicines and their respective potencies as given in Table 2. Present study showed maximum growth inhibition zone of 13mm with the 30th potency of Belladonna.
Moreover, all the medicines except Lachesis showed highest GIZ in its 30th potency among the three potencies that had been selected for the study. Ethanol showed a constant GIZ of 7mm in all the three tests (Table 2, Figure 1).
Table 2: Showing Growth Inhibitory Zones (GIZ) of Different Medicines and the Control p-value of the Differences between Control Value and the Test Value Shows Significant Differences (**<0.01 level, * <0.05 level)
| Medicines/Control | 6 CH Mean±S.D (mm) | 30 CH Mean±S.D (mm) | 200 CH Mean±S.D (mm) |
| Belladonna | 9±1.4 | 13±0.0** | 7±1.0 |
| Mercurius solubilis | 6±0.0 | 11.5±0.5** | 8 ±2.0 |
| Lachesis | 7.5±0.5 | 6.5±0.5 | 7.5±1.5 |
| Ferrum phosphoricum | 10.5±0.7* | 11±1.0* | 11±1* |
| Lycopodium clavatum | 6±0 | 10±2.0 | 9±3.0 |
| Ethanol (Control) | 7±0.0 | 7±0.0 | 7±0.0 |
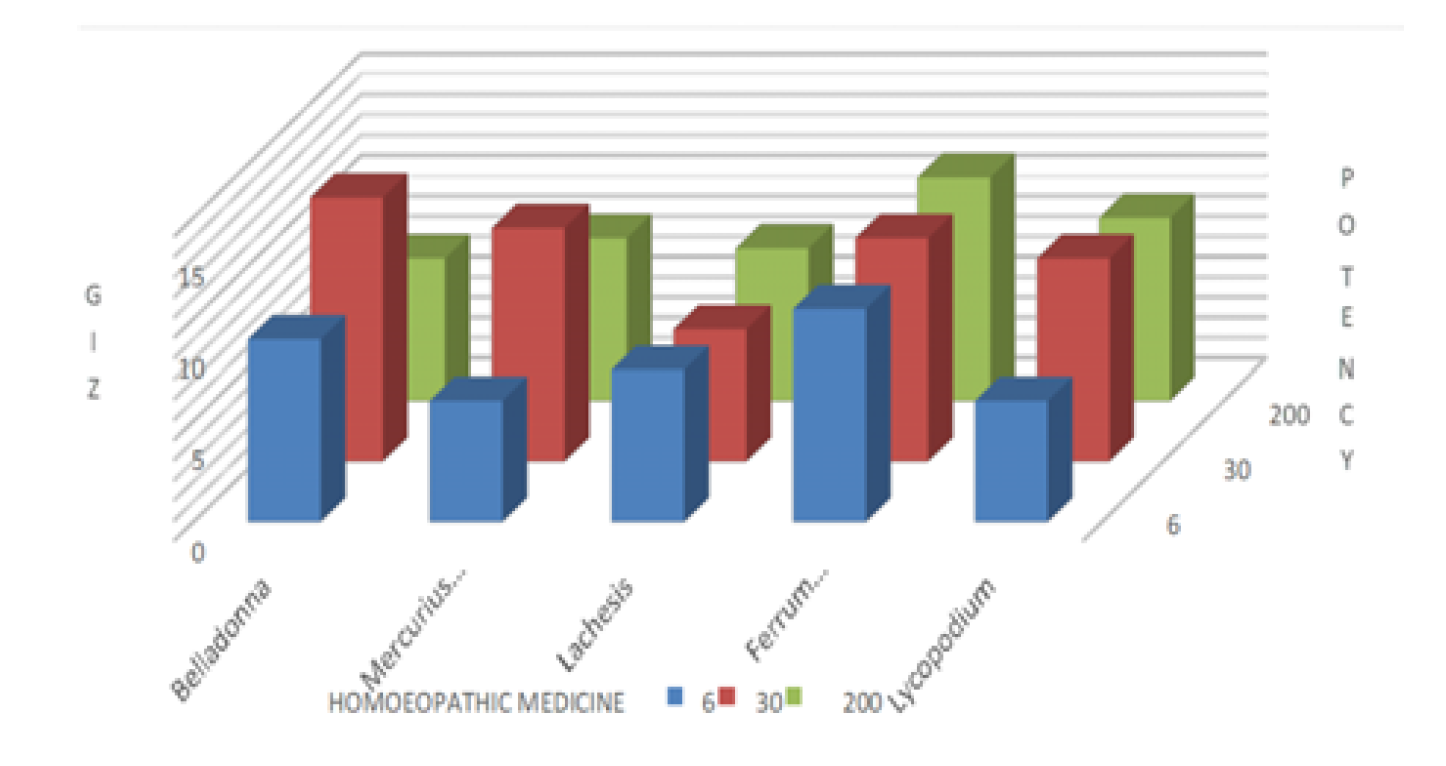
Figure 1: GIZ of Different Medicines at Different Dilution
Homoeopathic drugs have been extensively used since its inception in curing various cases of pathogenic manifestations. Be it the first use of the Cinchona bark in treating malaria or the prophylactic use of Belladonna in scarlet fever of Sydenham or the countless other uses over the century, homoeopathic drugs have proved their efficacy over and over again. Nowadays antimicrobial resistance has made the situation worse as microbes are changing their pattern through frequent mutations [32, 33]. This current crisis is a real eye opener and opening path for the homoeopathic researchers to work on alternative agents against microbes. Passeti et al. [34], in their study showed that homoeopathic medicine Belladonna 30CH and a Nosode (6CH and 30CH) prepared from Methicillin-Resistant Staphylococcus Aureus (MRSA), on the same bacterium significantly decreased bacterial DNase production and reduced red blood cell lysis [34]. Zaman et al., proved that mother tinctures of Rhus glabra and Thuja occidentalis have higher antibiotic property than povidone iodine [35]. Nambison et al., has on the other hand proved the antibiotic effect of potentised drugs on bacterial strains [36]. In this study we observed that homoeopathic medicines Belladonna, Mercurius solublis, Ferrum phosphoricum, Lycopodium clavatum (arranged in decreasing order of GIZ) at 30th potency can inhibit the growth of S. pyogenes in vitro and they possess antibacterial property which cannot be solely attributed to the dispensing medium i.e. ethanol (91.2 % v/v). After going through Cochrane, HomBRex (Homoeopathy Basic Research Experiments), Medline, PubMed databases, some previous in vitro studies with different organisms were found showing positive result, unfortunately no such study assessing the anti-bacterial activity of homoeopathic medicine on S. Pyogenes in laboratory settings was found unlike our experiment [37-50]. Major question arises despite of its commendable success in the clinical practice and laboratory-based evidences are unknown mechanism of actions of post-Avogadro dilutions of homeopathic preparations. Though some recent studies showed that homoeopathic medicines contain measurable source nanoparticles, that act on living body by complex physiological phenomena like hormesis, allostatic stress response, cross adaptation, time dependent sensitization [51-53]. Chatterjee et al., suggested that there are three hypothetical mechanisms by which the metallic nanoparticles can act on the bacteria, that is by:
Accumulation of nanoparticles in the membrane of bacteria, changes its permeability, consequently, intracellular contents are released
Generation of reactive oxygen species with oxidative deterioration to cell content
Uptake of ions derived from metallic nanoparticles, ATP production and inhibition of DNA replication
Similar mechanisms can be hypothesized in this study where nanoparticles of Belladonna and other medicines might stop the DNA replication and binary fission, ultimately inhibiting the bacterial growth or by free radical mediated pore formation in the bacterial cell wall leading to cell death [32,33]. It is not unknown that Homoeopathy is one of the most popular system of medicine in developing and many developed countries in spite of many criticisms. Practically, in clinical settings homoeopathic physicians has been treating many acute cases regularly since ages and cases of GAS diseases (Sore throat, RTI, Suppurative lesions) are one of them but paucity of basic research, evidence-based case reports and case series or clinical trials regarding are major lag in the literature.
As because it is a completely new finding and it has limitations so in future further level of experiments studying changes at the level of inflammatory cytokines should be performed to see the efficacy of these medicines.
This study clearly shows that efficacy of homoeopathic medicines particularly Belladonna, Mercurius solublis, Ferrum phosphoricum, Lycopodium clavatum at 30th potency can restrict growth of S. pyogenes. Right from the time of birth human body shows high affinity towards streptococcal infections, if we can restrict the bacterial infections through homeopathic medicines it can be useful to control childhood infections and can also be used to reduce the use of antibiotics and its complications. It can also be used in the form of add on therapy to minimize the risk of developing antibiotic resistance. As it is a completely new finding further studies should be done on this line for the benefit of the mankind.
Author Contributions
Antara Majumder: Conceptualization, Visualization Kumar Gaurav: Investigation Sayak Ghosh: Resources, Investigation Joydeep Khanra: Data Curation. Pritam Goswami: Writing-Original Draft, Visualization, Investigation Satadal Das: Conceptualization, Writing-Review and Editing, Supervision,
Acknowledgement
We would like to acknowledge institutional heads of all the participating institutions for their support.
Willey, J. et al. Prescott’s Microbiology. 7th ed., McGraw-Hill Education, 2011.
Kayser, F. et al. Medical Microbiology. Georg Thieme Verlag, 2005.
Oliver, J. et al. “Group a streptococcus pharyngitis and pharyngeal carriage: A meta-analysis.” PLOS Neglected Tropical Diseases, vol. 12, 2018, pp. 1–5, https://doi.org/10.1371/journal.pntd.0006335.
Barnett, T.C. et al. “The fall and rise of group a streptococcus disease.” Epidemiology and Infection, vol. 147, 2018, pp. 1–6, https://doi.org/10.1017/S0950268818002285.
Dougherty, S. et al. “Rheumatic heart disease screening: current concepts and challenges.” Annals of Pediatric Cardiology, vol. 10, 2017, pp. 39–49, https://doi.org/10.4103/0974-2069.197051.
Schroeder, B.M. “Diagnosis and management of group A streptococcal pharyngitis.” American Family Physician, vol. 67, 2003, pp. 880–884.
Carapetis, J. et al. “The global burden of group A streptococcal disease.” The Lancet Infectious Diseases, vol. 5, 2005, pp. 685–694, https://doi.org/10.1016/S1473-3099(05)70267-X.
Danchin, M.H. et al. “Burden of acute sore throat and group A streptococcal pharyngitis in school-aged children and their families in Australia.” Pediatrics, vol. 120, no. 5, 2007, pp. 950–957, https://doi.org/10.1542/peds.2006-3368.
Efstratiou, A. and T. Lamagni. “Epidemiology of Streptococcus pyogenes.” Streptococcus pyogenes: Basic Biology to Clinical Manifestations, edited by J.J. Ferretti et al., University of Oklahoma Health Sciences Center, 2016.
Nandi, S. et al. “Group A streptococcal sore throat in a periurban population of northern India: A one-year prospective study.” Bulletin of the World Health Organization, vol. 79, 2001, pp. 528–533.
Matthys, J. et al. “Differences among international pharyngitis guidelines: not just academic.” The Annals of Family Medicine, vol. 5, 2007, pp. 436–443, https://doi.org/10.1370/afm.741.
Moro, M.L. et al. “Why do pediatricians prescribe antibiotics? results of an italian regional project.” BMC Pediatrics, vol. 9, 2009, p. 69, https://doi.org/10.1186/1471-2431-9-69.
Chiappini, E. et al. “Analysis of different recommendations from international guidelines for the management of acute pharyngitis in adults and children.” Clinical Therapeutics, vol. 33, no. 1, 2011, pp. 48–58, https://doi.org/10.1016/j.clinthera.2011.02.001.
Danchin, M.H. et al. “Treatment of sore throat in light of the cochrane verdict: is the jury still out?” Medical Journal of Australia, vol. 177, no. 9, 2002, pp. 512–515, https://doi.org/10.5694/j.1326-5377.2002.tb04925.x.
Ventola, C.L. “The Antibiotic resistance crisis: Part 1: causes and threats.” P&T, vol. 40, 2015, pp. 277–283.
Taneja, N. and M. Sharma. “Antimicrobial resistance in the environment: The Indian scenario.” Indian Journal of Medical Research, vol. 149, 2019, pp. 119–128, https://doi.org/10.4103/ijmr.IJMR_331_18.
Gottlieb, T. and G.R. Nimmo. “Antibiotic resistance is an emerging threat to public health.” Medical Journal of Australia, vol. 194, 2011, pp. 281–283, https://doi.org/10.5694/j.1326-5377.2011.tb02973.x.
Zaman, S.B. et al. “A review on antibiotic resistance: alarm bells are ringing.” Cureus, vol. 9, 2017, e1403.
Abraham, T. and S. Sistla. “Trends in antimicrobial resistance patterns of group A streptococcus.” Indian Journal of Medical Microbiology, vol. 36, 2018, pp. 186–191, https://doi.org/10.4103/ijmm.IJMM_18_107.
Fixsen, A. “Homeopathy in the age of antimicrobial resistance.” Homeopathy, vol. 107, 2018, pp. 99–114, https://doi.org/10.1055/s-0037-1621745.
Molinari, G. et al. “The fibronectin-binding protein of Streptococcus pyogenes, SfbI, is involved in the internalization of group A streptococci by epithelial cells.” Infection and Immunity, vol. 65, 1997, pp. 1357–1363.
Fischetti, V.A. “Surface proteins on gram-positive bacteria.” Gram-Positive Pathogens, edited by V.A. Fischetti et al., American Society for Microbiology Press, 2000, pp. 11–24, https://doi.org/10.1128/IAI.00717-07.
Berge, A. and U. Sjobring. “PAM, a novel plasminogen-binding protein from Streptococcus pyogenes.” Journal of Biological Chemistry, vol. 268, 1993, pp. 25417–25424.
Frithz, E. et al. “Extensive sequence homology between iga receptor and M proteins in Streptococcus pyogenes.” Molecular Microbiology, vol. 3, 1989, pp. 1111–1119, https://doi.org/10.1111/j.1365-2958.1989.tb00261.x.
Gomi, H. et al. “The gene sequence and some properties of protein H: A novel igg-binding protein.” Journal of Immunology, vol. 144, 1990, pp. 4046–4052.
Stenberg, L. et al. “Many group A streptococcal strains express two different immunoglobulin-binding proteins.” Molecular Microbiology, vol. 6, 1992, pp. 1185–1194.
Stenberg, L. et al. “Molecular characterization of protein sir, a streptococcal cell surface protein that binds both immunoglobulin A and immunoglobulin G.” Journal of Biological Chemistry, vol. 269, 1994, pp. 13458–13464.
Berggard, K. et al. “Binding of human C4BP to the hypervariable region of M protein.” Molecular Microbiology, vol. 42, 2001, pp. 539–551.
Johnsson, E. et al. “A highly variable region in members of the streptococcal M protein family binds the human complement regulator C4BP.” Journal of Immunology, vol. 157, 1996, pp. 3021–3029.
Ringdahl, U. et al. “A role for the fibrinogen-binding regions of streptococcal M proteins in phagocytosis resistance.” Molecular Microbiology, vol. 37, 2000, pp. 1318–1326, https://doi.org/10.1086/596656.
Musumeci, R. et al. “Internalization-associated proteins among Streptococcus pyogenes.” Clinical Infectious Diseases, vol. 37, no. 2, 2003, pp. 173–179, https://doi.org/10.1086/375589.
Gupta, M. et al. “Effective antimicrobial activity of green ZnO nanoparticles of Catharanthus roseus.” Frontiers in Microbiology, vol. 9, 2018, pp. 2030, https://doi.org/10.3389/fmicb.2018.02030.
Kon, K. and M. Rai. Antibiotic Resistance. Elsevier, 2016, pp. 121–126, 135–136.
Passeti, T. et al. “Action of antibiotic oxacillin on In vitro growth of MRSA.” Homeopathy, vol. 106, 2017, pp. 27–31, https://doi.org/10.1016/j.homp.2016.10.002.
Zaman, M.M. et al. “Comparative analysis of antibacterial activity of povidone iodine and homoeopathic mother tinctures.” Indian Journal of Research in Homoeopathy, vol. 10, 2016, pp. 36–41.
Nambison, N. et al. “Antibacterial activity of homeopathic drugs in vitro.” International Journal of Homoeopathic Sciences, vol. 1, no. 1, 2017, pp. 26–29, https://doi.org/10.1055/s-0038-1637729.
Clausen, J. et al. “Infection models in basic research on homeopathy.” Homeopathy, vol. 99, no. 4, 2010, pp. 263–270, https://doi.org/10.1016/j.homp.2010.08.001.
Almaguer, A. and P. Gonzalez. “Antibacterial activity of homoeopathic medications.” ODOVTOS–International Journal of Dental Sciences, vol. 20, 2018, pp. 71–79.
Rehman, A. et al. “Comparative analysis of antibacterial activity of ciprofloxacin and homeopathic mother tincture.” RADS Journal of Pharmacy and Pharmaceutical Sciences, vol. 6, no. 2, 2018, pp. 113–118.
Sandoval, C.H. et al. “Preliminary research for testing baptisia tinctoria 30c effectiveness against salmonellosis.” British Homoeopathic Journal, vol. 87, no. 3, 1998, pp. 131–134.
Oberbaum, M. et al. “Treatment of experimentally-induced aids in mice by very high dilutions of virus: A Preliminary study.” Signals and Images, 1989, pp. 127–129.
[42] Rabe, A. et al. “Effectiveness and tolerability of a homoeopathic remedy compared with conventional therapy for mild viral infections.” International Journal of Clinical Practice, vol. 58, no. 9, 2004, pp. 827–832, https://doi.org/10.1093/ecam/nel045.
Velkers, F.C. et al. “Isopathic and pluralist homeopathic treatment of commercial broilers with experimentally induced colibacillosis.” Research in Veterinary Science, vol. 78, no. 1, 2005, pp. 77–83.
[44] Gupta, G. and L.M. Singh. “Virus chemotherapy through homeopathic drugs: A new approach.” British Homeopathic Research Group Communications, vol. 14, 1985, pp. 30–35.
Singh, L.M. and G. Gupta. “Antiviral efficacy of homeopathic drugs against animal viruses.” British Homeopathic Journal, vol. 74, 1985, pp. 168–174.
Sukul, N.C. et al. “Antifilarial effect of artemisia nilagirica extract and its ultra-high dilutions against canine dirofilariasis.” Japanese Journal of Tropical Medicine and Hygiene, vol. 27, no. 4, 1999, pp. 477–481.
Oberbaum, M. et al. “Antiviral activity of engystol®: An in vitro analysis.” Journal of Alternative and Complementary Medicine, vol. 11, no. 5, 2005, pp. 855–862, https://doi.org/10.1089/acm.2005.11.855.
Glatthaar-Saalmüller, B. “In vitro evaluation of the antiviral effects of the homeopathic preparation gripp-heel on selected respiratory viruses.” Canadian Journal of Physiology and Pharmacology, vol. 85, no. 11, 2007, pp. 1084–1090.
Lira-Salazar, G. et al. “Effects of homeopathic medications eupatorium perfoliatum and arsenicum album on parasitemia of plasmodium berghei-infected mice.” Homeopathy, vol. 95, no. 4, 2006, pp. 223–228, https://doi.org/10.1016/j.homp.2006.06.003.
Sukul, N.C. et al. “Reduction in the number of infective trichinella spiralis larvae in mice by use of homeopathic drugs.” Complementary Medicine Research, vol. 12, no. 4, 2005, pp. 202–205.
Bell, I.R. and M. Koithan. “A model for homeopathic remedy effects: Low-dose nanoparticles, allostatic cross-adaptation and time-dependent sensitization in a complex adaptive system.” BMC Complementary and Alternative Medicine, vol. 12, no. 1, 2012, pp. 1–21.
Upadhyay, R.P. and C. Nayak. “Homeopathy emerging as nanomedicine.” International Journal of High Dilution Research, vol. 10, no. 37, 2011, pp. 299–310.
Bellavite, P. et al. “Immunology and homeopathy. V: The rationale of the ‘simile.’” Evidence-Based Complementary and Alternative Medicine, vol. 4, 2007, pp. 149–163, https://doi.org/10.1093/ecam/nel117
