
+91 6002993949
submission@iarconsortium.org
Open Access
ISSN (Print) : 2709-3301
ISSN (Online) : 2709-331X
Background: Chronic Obstructive Pulmonary Disease (COPD) is a severe lung disease and a major cause of mortality and morbidity worldwide. Because COPD is associated with systemic inflammation, which initiates or aggravates comorbid diseases, cardiovascular disease and arrhythmia risks have been reported to be associated with COPD. In previous studies, supraventricular arrhythmia, particularly atrial fibrillation, was the most common cardiac arrhythmia in patients with COPD. However, in patients with acute COPD exacerbation, the most common arrhythmia was reported to be ventricular premature beats. Aim: The aim of this study is to determine the risk and prevalence of arrhythmia among COPD patient. Methods and Materials: This prospective cross sectional study carried out in the Azadi Teaching Hospital/Kirkuk general hospital in Kirkuk between November 2021 to March 2022. Patients who had been diagnosed with COPD depending on clinical features and admitted to hospital for exacerbation of COPD. Each patient has ECG on admission and 24-48 hours Holter monitoring. Results: There were 82 patients with acute exacerbation of COPD have been included in this study. The mean age of patients was 65.8±7.9 years (range 55-90 years). Majority of patients (80.5%) were males. Regarding medical history for HTN, DM and IHD, there were 47 (57.3%), 43 (52.4%) and 28 (34.1%) patients had HTN, DM and IHD respectively. For smoking, all patients were a smoker with mean pack per year was 36.8±8.5 pack-years. The ECG finding at the time of COPD exacerbation showed that, 40 (48.7%) patients had abnormal ECG finding and 42 (51.2%) patients had normal ECG finding. The most common abnormal ECG finding was Ectopic beats that presented in 10 (12.2%) of patients, followed by AF which was presented in 8 (9.8%) patients. The Holter finding showed that, 47 (57.3%) patients had abnormal Holter finding and 35 (42.6%) patients had normal Holter finding. The most common abnormal Holter finding was Ectopic beats that presented in 29 (35.4%) of patients, followed by AF in 8 (9.8%) patients, RBBB was presented in 5 (6.1%) patients. No significant associations have been found with abnormal ECG or Holter finding for demographic characteristics. Spo2 and PR showed significant association with abnormal ECG or Holter finding. Conclusion: The prevalence of arrhythmia in patients with exacerbation of COPD was 48.7% by ECG and increased to 57.3% with 24-48 hours Holter monitoring. Only Spo2 and PR showed significant association with abnormal ECG or Holter finding.
Chronic Obstructive Pulmonary Disease (COPD) is a progressive, heterogeneous respiratory disorder characterized by persistent airflow limitation and chronic inflammatory response of the airways and lung parenchyma to noxious particles and gases [1]. It represents one of the leading causes of morbidity and mortality worldwide and is currently ranked among the top three causes of death globally [2]. The Global Initiative for Chronic Obstructive Lung Disease (GOLD) defines COPD by a post-bronchodilator FEV₁/FVC ratio <0.70, reflecting incompletely reversible airflow obstruction [1]. In 2019, COPD was estimated to affect approximately 12% of the global population, corresponding to nearly 390–400 million individuals [3]. Although COPD is primarily a pulmonary disease, it is now recognized as a systemic disorder with multiple extrapulmonary manifestations and comorbidities [4]. Among these, Cardiovascular Disease (CVD) is the most frequent and clinically significant comorbidity [5]. Patients with COPD are at increased risk of Coronary Artery Disease (CAD), Heart Failure (HF), Acute Myocardial Infarction (AMI) and cardiac arrhythmias [6]. Cardiovascular complications account for a substantial proportion of deaths in COPD patients, particularly during acute exacerbations [7]. Systemic inflammation plays a central role in linking COPD with cardiovascular morbidity [8]. Elevated circulating inflammatory mediators, oxidative stress, endothelial dysfunction and autonomic imbalance contribute to myocardial injury and electrical instability [9]. Hypoxemia, hypercapnia and acid–base disturbances further aggravate myocardial irritability and predispose to arrhythmogenesis [10]. Additionally, structural cardiac changes such as right ventricular hypertrophy, pulmonary hypertension and left ventricular diastolic dysfunction are common in advanced COPD and may increase arrhythmic risk [11]. Acute Exacerbations of COPD (AECOPD), defined as worsening of respiratory symptoms requiring additional therapy, represent critical events associated with increased hospitalization and mortality [12]. During AECOPD, arrhythmias are frequently observed and may complicate the clinical course [13]. Studies have reported that supraventricular arrhythmias, particularly Atrial Fibrillation (AF), are common in stable COPD, while ventricular premature beats and ventricular tachycardia are more frequently documented during acute exacerbations [14]. The prevalence of AF in COPD ranges from 4.7-15%, increasing up to 30% in severe disease [15]. Multifocal Atrial Tachycardia (MAT), a distinctive arrhythmia often associated with severe pulmonary disease, is particularly characteristic of COPD [16]. MAT is typically observed in elderly patients with respiratory failure and is associated with significant in-hospital mortality [17]. Furthermore, COPD severity has been identified as an independent predictor of ventricular arrhythmias and sudden cardiac death [18]. Pharmacologic therapy may also influence arrhythmia risk. Beta-adrenergic agonists and theophylline can enhance atrial automaticity and reduce refractory periods, potentially exerting pro-arrhythmic effects [19]. However, large clinical trials suggest that long-acting beta-agonists do not significantly increase serious arrhythmic events in most patients [20]. Electrolyte imbalances, particularly hypokalemia and hypomagnesemia, commonly encountered during exacerbations, further contribute to electrical instability [21]. Electrocardiographic abnormalities are common in COPD patients, especially during exacerbations [22]. Prolonged P-wave dispersion, QT interval abnormalities and reduced heart rate variability reflect autonomic dysfunction and are associated with adverse outcomes [23]. Ambulatory Holter monitoring improves detection of transient or asymptomatic arrhythmias, with a diagnostic yield of 15–39% in symptomatic individuals [24]. Despite growing evidence of the COPD–arrhythmia association, the relationship remains complex due to overlapping comorbidities, medication effects and asthma–COPD overlap syndrome [25]. Understanding the prevalence, risk factors and clinical implications of arrhythmias in COPD is therefore essential for improving patient outcomes. The aim of this study is to determine the prevalence and risk of cardiac arrhythmias among patients with COPD and to evaluate their clinical significance. The aim of this study is to determine the risk and prevalence of arrhythmia among COPD patients.
Patients and Methods
This prospective cross-sectional study was conducted to evaluate the prevalence and pattern of cardiac arrhythmias among patients admitted with Acute Exacerbation of Chronic Obstructive Pulmonary Disease (AECOPD). The study was carried out at Azadi Teaching Hospital and Kirkuk General Hospital, Iraq, over a five-month period from November 2021 to March 2022. The study population consisted of adult patients diagnosed with COPD who were admitted to the hospital due to acute exacerbation during the study period. Diagnosis of COPD was established based on clinical assessment and history consistent with chronic airflow limitation.
Inclusion Criteria
Patients were eligible for inclusion if they met the following criteria:
Age ≥18 years
Clinical diagnosis of COPD based on:
History of cigarette smoking of more than 20 pack-years
Chronic productive cough for at least 3 months per year for two consecutive years
Dyspnea on exertion
Use of accessory respiratory muscles
Presence of expiratory wheezes and prolonged expiratory phase on chest examination
Admission to hospital with acute exacerbation of COPD
Exclusion Criteria
Patients were excluded if they had:
Pre-existing congenital heart disease, documented coronary artery disease, valvular heart disease, uncontrolled hypertension, or unstable angina
Physical disabilities that interfered with clinical assessment or patients in a comatose state
Refusal to provide informed consent for participation in the study
Data Collection
Data were collected through direct patient interviews and clinical examination using a structured questionnaire specifically designed for the study. The questionnaire consisted of two main parts.
Part One: Demographic and Clinical Data
This section included:
Age and gender
Smoking status and duration (pack-years)
Assessment of comorbidities including hypertension, diabetes mellitus and ischemic heart disease
Clinical history of cough, sputum color, dyspnea (on exertion or at rest) and fever
General respiratory examination including central cyanosis, use of accessory muscles, tremor and clubbing
Vital signs: Pulse Rate (PR), Blood Pressure (BP), Respiratory Rate (RR) and Oxygen Saturation (SpO₂)
Detailed chest examination assessing vesicular breath sounds, bronchial breathing, prolonged expiration, wheezes and crepitations
Laboratory and imaging investigations including White Blood Cell Count (WBC), chest X-ray, Electrocardiography (ECG), Echocardiography (ECHO) and 24-hour Holter monitoring
Part Two: Electrocardiographic Assessment
A baseline 12-lead Electrocardiogram (ECG) was performed for each patient upon admission. ECG recordings were analyzed for the presence of arrhythmias as follows:
Atrial Ectopic Beats
Identified by premature P waves with altered morphology compared to sinus P waves. The PR interval could be shorter or longer than preceding complexes. In some cases, the P wave was superimposed on the preceding T wave. Blocked atrial ectopics were defined as premature P waves not followed by a QRS complex.
Atrial Fibrillation (AF)
Diagnosed by absence of distinct P waves, presence of fibrillatory waves and a grossly irregular ventricular rhythm.
Ventricular Ectopic Beats
Defined as premature wide QRS complexes (≥0.12 seconds) occurring before the expected sinus beat, usually with discordant T waves. Three or more consecutive ventricular ectopic beats were classified as ventricular tachycardia.
Holter Monitoring
All enrolled patients underwent ambulatory electrocardiographic monitoring using a Holter device for 24–48 hours. This allowed detection of transient, intermittent, or asymptomatic arrhythmias not captured on baseline ECG.
Statistical Analysis
Data were entered and analyzed using the Statistical Package for Social Sciences (SPSS) version 23. Continuous variables were expressed as mean ± Standard Deviation (SD), along with minimum and maximum values. Categorical variables were presented as frequencies and percentages. Comparisons between groups were performed using the independent samples t-test for continuous variables and the chi-square test for categorical variables. A p-value of less than 0.05 was considered statistically significant.
There were 82 patients with acute exacerbation of COPD have been included in this study. The mean age of patients was 65.8±7.9 years (range 55-90 years). Majority of patients (80.5%) were males. Regarding medical history for HTN, DM and IHD, there were 47 (57.3%), 43 (52.4%) and 28 (34.1%) patients had HTN, DM and IHD respectively (Table 1 and Figure 1).
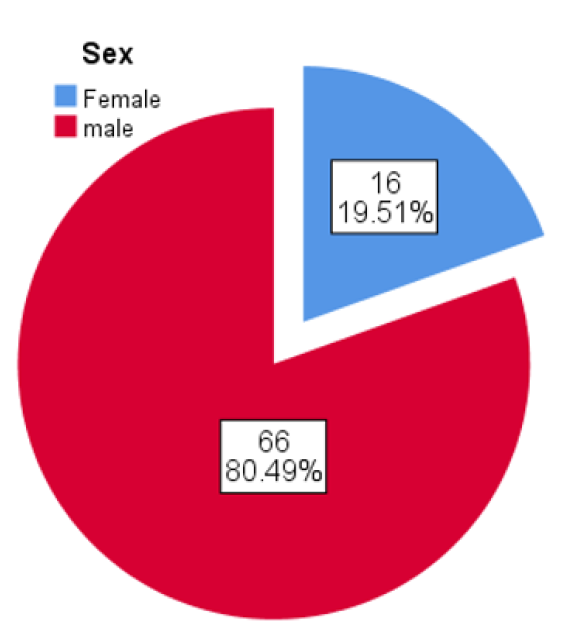
Figure 1: Gender Distribution across Patients
Table 1: Demographic Characteristics of Patients
Age |
|
Mean±SD | 65.8±7.9 years |
Range | 55-90 years |
Gender, N (%) | |
Male | 66 (80.5%) |
Female | 16 (19.5%) |
Hypertension, N (%) | |
Yes | 47 (57.3%) |
No | 35 (42.7%) |
DM, N (%) | |
Yes | 43 (52.4%) |
No | 39 (47.6%) |
IHD, N (%) | |
Yes | 28 (34.1%) |
No | 54 (65.9%) |
Past Medical History, N (%) | |
No | 18 (22%) |
One and more | 64 (78%) |
WBC | |
Mean ± SD | 10731.71±2748.95 |
Range | 7000 -22000 |
For smoking, all patients were a smoker with mean pack per year was 36.8±8.5 pack-years. For the vital signs, the descriptive statistics for vital signs are given in Table 2.
Table 2: Descriptive Statistics of Vital Signs
SBP | N | Minimum | Maximum | Mean | SD |
82 | 90 | 180 | 144.33 | 15.88 | |
DBP | 82 | 60 | 110 | 87.93 | 8.01 |
RR | 82 | 16 | 28 | 21.07 | 2.69 |
PR | 82 | 85 | 190 | 110.37 | 22.93 |
SPO2 | 82 | 80 | 94 | 89.93 | 2.27 |
ECHO finding, the ECHO finding showed that 41 (50%) patients had abnormal ECHO finding and another half of patients had normal ECHO finding. The abnormal ECHO findings are given in Table 3.
Table 3: Abnormal ECHO Finding
| Frequency | Percent |
Diastolic dysfunction | 1 | 1.2 |
LVD | 8 | 9.8 |
mild LVH | 13 | 15.9 |
mild RVH | 2 | 2.4 |
moderate LVH | 7 | 8.5 |
PH | 1 | 1.2 |
RVD | 2 | 2.4 |
RVD+ PH | 1 | 1.2 |
RVH | 4 | 4.9 |
RVH+ PH | 1 | 1.2 |
Severe LVH | 1 | 1.2 |
The ECG finding at the time of COPD exacerbation showed that, 40 (48.7%) patients had abnormal ECG finding and 42 (51.2%) patients had normal ECG finding (Figure 2).
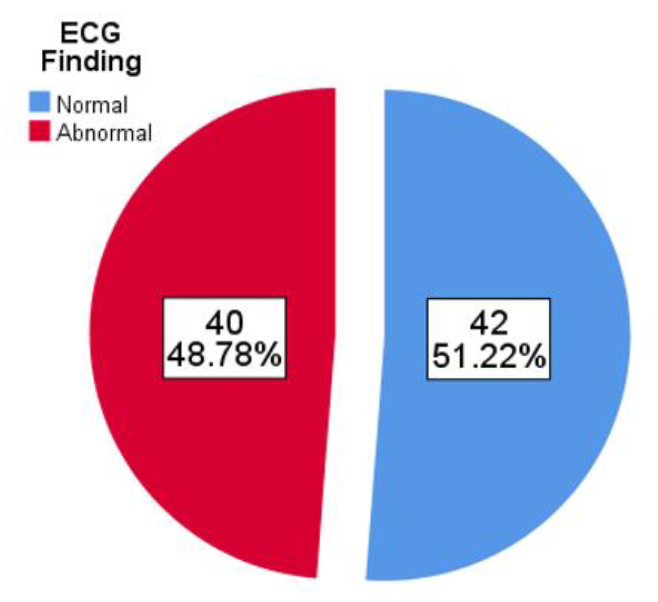
Figure 2: ECG Finding at the Time of COPD Exacerbation
The most common abnormal ECG finding was Ectopic beats that presented in 10 (12.2%) of patients, followed by AF which was presented in 8 (9.8%) patients. The descriptions of abnormal ECG findings are given in below Table 4.
Table 4: Abnormal ECG Findings
| AF | Frequency | Percent |
| 8 | 9.8 | |
| Ectopic Beats | 10 | 12.2 |
| MAT | 2 | 2.4 |
| RBBB | 5 | 6.1 |
| S arrhythmia | 7 | 8.5 |
| S Tachycardia | 6 | 7.3 |
| SVT | 1 | 1.2 |
| VT | 1 | 1.2 |
The Holter finding showed that, 47 (57.3%) patients had abnormal Holter finding and 35 (42.6%) patients had normal Holter finding (Figure 3).
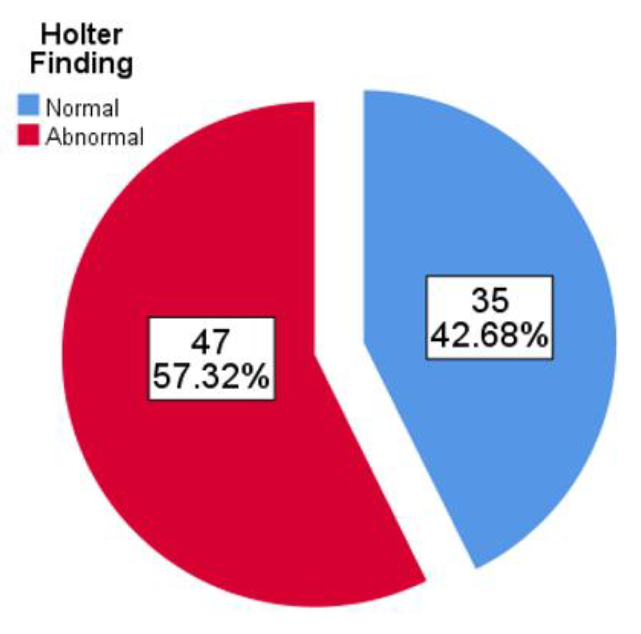
Figure 3: Holter Finding
The most common abnormal Holter finding was Ectopic beats that presented in 29 (35.4%) of patients, followed by AF in 8 (9.8%) patients, RBBB was presented in 5 (6.1%) patients. The descriptions of abnormal Holter findings are given Table 5.
Table 5: Abnormal Holter Findings
| AF | Frequency | Percent |
| 8 | 9.8 | |
| Ectopic beats | 29 | 35.4 |
| M. ectopic | 1 | 1.2 |
| MAT | 2 | 2.4 |
| RBBB | 5 | 6.1 |
| Sinus arrhythmia | 2 | 2.4 |
The association between abnormal ECG and demographic characteristics did not demonstrated a significant difference between abnormal and normal ECG finding (p>0.05) (Table 6).
Table 6: Factors Associated with Abnormal ECG
| Age | Normal | Abnormal |
| |||
Count | N % | Count | % | p value | ||
Sex | Female | 5 | 11.9 | 11 | 27.5% | 0.075 |
male | 37 | 88.1 | 29 | 72.5% | ||
HTN | No | 19 | 45.2 | 16 | 19 | 0.63 |
Yes | 23 | 54.8 | 24 | 23 | ||
DM | No | 16 | 38.1 | 23 | 16 | 0.079 |
Yes | 26 | 61.9 | 17 | 26 | ||
IHD | No | 25 | 59.5 | 29 | 25 | 0.21 |
Yes | 17 | 40.5 | 11 | 17 | ||
PMH | 0 | 6 | 14.3 | 12 | 6 | 0.38 |
1 | 14 | 33. | 11 | 14 | ||
2 | 14 | 33.3 | 10 | 14 | ||
3 | 8 | 19.0 | 7 | 8 | ||
Regarding vital signs and its association with ECG finding, the RR and PR showed significant higher mean across patients with abnormal ECG finding, while SPo2 showed significant lower mean among patients with abnormal ECG finding in comparison to normal ones (p<0.05). Other factors did not showed significant association (p>0.05) (Table 7).
Table 7: Association between Age, Vital Signs with ECG Finding
| Age | Normal | Abnormal |
| ||
Mean | SD | Mean | SD | P value | |
67 | 9 | 64 | 7 | 0.097 | |
Smoking | 36 | 7 | 38 | 10 | 0.41 |
SBP | 145 | 15 | 143 | 17 | 0.64 |
DBP | 89 | 8 | 87 | 8 | 0.13 |
RR | 20 | 2 | 22 | 3 | 0.002 |
PR | 95 | 7 | 127 | 23 | 0.0001 |
SPO2 | 91 | 2 | 89 | 3 | 0.001 |
WBC | 10233 | 2869 | 11282 | 2533 | 0.084 |
The association between abnormal Holter and demographic characteristics did not demonstrated a significant difference between abnormal and normal Holter finding (p>0.05) (Table 8).
Table 8: Factors Associated with Abnormal Holter
| Age | Normal | Abnormal |
| |||
Count | N % | Count | % | p value | ||
Sex | Female | 6 | 17.1 | 10 | 21.3 | 0.64 |
male | 29 | 82.9 | 37 | 78.7 | ||
HTN | No | 16 | 45.7 | 19 | 40.4 | 0.63 |
Yes | 19 | 54.3 | 28 | 59.6 | ||
DM | No | 17 | 48.6 | 22 | 46.8 | 0.87 |
Yes | 18 | 51.4 | 25 | 53.2 | ||
IHD | No | 24 | 68.6 | 30 | 63.8 | 0.65 |
Yes | 11 | 31.4 | 17 | 36.2 | ||
PMH | 0 | 8 | 22.9 | 10 | 21.3 | 0.89 |
1 | 12 | 34.3 | 13 | 27.7 | ||
2 | 9 | 25.7 | 15 | 31.9 | ||
3 | 6 | 17.1 | 9 | 19.1 | ||
Regarding vital signs and its association with Holter finding, the smoking (pack-years) and PR showed significant higher mean across patients with abnormal Holter finding, while SPO2 showed significant lower mean among patients with abnormal Holter finding in comparison to normal ones (p<0.05). Other factors did not showed significant association (p>0.05) (Table 9).
Table 9: Association between Age, Vital Signs with Holter Finding
Age | Normal | Abnormal |
| ||
Mean | SD | Mean | SD | p value | |
66 | 8 | 65 | 7 | 0.34 | |
Smoking | 35 | 8 | 40 | 9 | 0.04 |
SBP | 145 | 15 | 144 | 18 | 0.87 |
DBP | 89 | 7 | 87 | 9 | 0.35 |
RR | 21 | 3 | 22 | 3 | 0.057 |
PR | 103 | 19 | 125 | 23 | 0.0001 |
SPO2 | 91 | 1 | 89 | 3 | 0.001 |
WBC | 10315 | 2494 | 11536 | 3073 | 0.074 |
There was no significant association between the comorbidities and CT nor O2 saturation (p>0.05) (Table 10).
Table 10: Group Statistics Comparison of BMI with CT and O2 Saturation
C.T scan | Variable | N | Mean | SD | p value |
Hypertension | 36 | 67.78 | 15.741 | 0.76 | |
No | 64 | 66.80 | 15.207 | ||
O2 sat. | Hypertension | 36 | 83.92 | 5.674 | 0.71 |
No | 64 | 83.44 | 7.536 | ||
C.T scan | DM | 27 | 70.37 | 14.539 | 0.2 |
No DM | 73 | 65.96 | 15.538 | ||
O2 sat. | DM | 27 | 82.44 | 5.235 | 0.3 |
No DM | 73 | 84.04 | 7.404 | ||
C.T scan | Others | 10 | 63.00 | 18.439 | 0.36 |
No comorbidities | 90 | 67.61 | 14.995 | ||
O2 sat. | Others | 10 | 85.10 | 6.903 | 0.47 |
No comorbidities | 90 | 83.44 | 6.915 |
Chronic Obstructive Pulmonary Disease (COPD) is a leading cause of global morbidity and mortality and remains one of the top contributors to chronic disease burden worldwide [1–3]. Although COPD has traditionally been regarded as a pulmonary disorder, it is now widely recognized as a systemic inflammatory condition with important cardiovascular consequences [4,5]. Cardiovascular Disease (CVD), including ischemic heart disease, heart failure and cardiac arrhythmias, represents one of the most frequent and clinically significant comorbidities in COPD patients [5,6]. The present study aimed to determine the prevalence and pattern of arrhythmias among patients hospitalized with acute exacerbation of COPD (AECOPD). The mean age of patients in this study was 65.8±7.9 years, which is consistent with the epidemiological profile of hospitalized COPD populations reported globally [3,7]. Increasing age is strongly associated with disease severity, comorbidity burden and mortality in COPD [1,2]. Advanced age also independently increases the risk of Atrial Fibrillation (AF) and other arrhythmias, thereby compounding cardiovascular risk in COPD patients [6]. Male predominance (80.5%) in our cohort aligns with regional data demonstrating higher COPD prevalence among men, largely attributable to greater smoking exposure [3,8]. Smoking is a well-established risk factor for both COPD and cardiovascular disease, promoting endothelial dysfunction, oxidative stress and myocardial irritability [5]. Prolonged smoking duration in our study was associated with abnormal Holter findings, reinforcing the cumulative cardiovascular impact of tobacco exposure. Comorbidities such as hypertension and diabetes mellitus were common in our patients. This is consistent with previous reports indicating that more than half of COPD patients have at least one major comorbidity [5,9]. The coexistence of metabolic and cardiovascular disorders enhances systemic inflammation and autonomic imbalance, which are central mechanisms in arrhythmogenesis [4,10]. Leukocytosis observed during exacerbation (WBC range 7000–22000 cells/mL) reflects heightened inflammatory activity. Exacerbations are characterized by acute inflammatory surges that amplify oxidative stress and cytokine release [10,11]. These inflammatory mediators may directly affect myocardial electrophysiology and promote atrial and ventricular ectopy [12]. Elevated vital signs-including tachycardia and increased respiratory rate-also reflect sympathetic activation and hypoxemic stress, both of which are known arrhythmogenic triggers [13]. In this study, 48.7% of patients had abnormal ECG findings during AECOPD. This proportion appears higher than that reported in some administrative datasets but comparable to focused clinical studies [14,15]. Variability between studies may reflect differences in patient severity, timing of ECG acquisition and arrhythmia definitions. Ectopic beats were the most common abnormality, followed by AF. Similar findings have been reported, where ventricular premature beats and AF were predominant arrhythmias in COPD populations [6,16]. AF prevalence in COPD ranges between 4.7 and 15%, increasing significantly in severe disease [17]. Holter monitoring revealed an even higher prevalence of arrhythmias (57.3%), underscoring the limitation of single-time ECG recordings. Ambulatory monitoring improves detection of transient arrhythmias that may be clinically silent [18]. Previous Holter-based studies have reported very high arrhythmia prevalence during exacerbations, particularly ventricular premature beats and supraventricular tachyarrhythmias [19]. Einvik et al. [20] demonstrated that premature ventricular complexes were significantly more common during exacerbated compared to stable COPD states. Kusunoki et al. [21] reported both ventricular and supraventricular arrhythmias in stable COPD, with ventricular arrhythmias likely linked to hypoxemia and structural cardiac strain [21]. The mechanisms underlying arrhythmias in COPD are multifactorial. Hypoxemia, hypercapnia and respiratory acidosis increase sympathetic tone and myocardial excitability [13]. Structural changes such as right ventricular hypertrophy and pulmonary hypertension contribute to electrical remodeling [22]. Autonomic dysfunction, reflected by reduced heart rate variability and QT interval abnormalities, further predisposes to arrhythmias [12,23]. Pharmacologic therapy may also influence arrhythmia risk. Beta-agonists and theophylline can increase heart rate and atrial automaticity [24]. Although large trials have not consistently shown major increases in serious arrhythmias with long-acting beta-agonists, caution is warranted in high-risk patients [25]. Electrolyte disturbances such as hypokalemia further aggravate electrical instability [26].
In our study, pulse rate and Oxygen Saturation (SpO₂) were significantly associated with abnormal ECG and Holter findings. This supports the concept that physiologic stress during exacerbation plays a pivotal role in arrhythmogenesis. Early identification of rhythm disturbances in AECOPD is therefore clinically important, as arrhythmias may prolong hospitalization and worsen prognosis [14,27]. Overall, our findings confirm that arrhythmias are common during COPD exacerbations, particularly when assessed using ambulatory monitoring. Routine cardiac evaluation-including ECG and selective Holter monitoring-should be considered in hospitalized AECOPD patients to improve risk stratification and guide management.
Ethical Approval
Ethical approval was obtained from the Internal Medicine Scientific Committee of the Iraqi Board. Official permission to conduct the study was secured from hospital authorities. Written informed consent was obtained from all participants prior to enrollment. Confidentiality of patient data was strictly maintained throughout the study.
Vestbo, J. et al. “Global strategy for the diagnosis, management and prevention of chronic obstructive pulmonary disease: GOLD executive summary.” American Journal of Respiratory and Critical Care Medicine, vol. 187, no. 4, 2013, pp. 347–365.
Lozano, R. et al. “Global and regional mortality from 235 causes of death for 20 age groups in 1990 and 2010.” The Lancet, vol. 380, no. 9859, 2012, pp. 2095–2128.
Adeloye, D. et al. “Global and regional estimates of COPD Prevalence: Systematic Review and Meta-Analysis.” Journal of Global Health, vol. 5, no. 2, 2015, p. 020415.
Barnes, P.J. “Chronic obstructive pulmonary disease: Effects beyond the lungs.” PLoS Medicine, vol. 7, no. 3, 2010, p. e1000220.
Schneider, C. et al. “Chronic obstructive pulmonary disease and the risk of cardiovascular diseases.” European Journal of Epidemiology, vol. 25, no. 4, 2010, pp. 253–260.
Konecny, T. et al. “Relation of chronic obstructive pulmonary disease to atrial and ventricular arrhythmias.” American Journal of Cardiology, vol. 114, no. 2, 2014, pp. 272–277.
Perera, P.N. et al. “Acute exacerbations of COPD in the United States: Inpatient burden and predictors of costs and mortality.” COPD, vol. 9, no. 2, 2012, pp. 131–141.
Polatli, M. et al. “COPD and associated healthcare resource consumption in the Middle East and North Africa: The BREATHE Study.” Respiratory Medicine, vol. 106, 2012, pp. S75–S85.
Miravitlles, M. et al. “Comorbidities of patients in tiotropium clinical trials.” International Journal of Chronic Obstructive Pulmonary Disease, vol. 10, 2015, pp. 549–560.
Ritchie, A.I. and J.A. Wedzicha. “Definition, causes, pathogenesis and consequences of COPD exacerbations.” Clinics in Chest Medicine, vol. 41, no. 3, 2020, pp. 421–438.
Titova, E. et al. “Procalcitonin, CRP, WBC and clinical status in diagnosing pneumonia in AECOPD.” Chronic Respiratory Disease, vol. 16, 2018, p. 1479972318769762.
Corbo, G.M. et al. “C-Reactive protein, lung hyperinflation and heart rate variability in COPD.” COPD, vol. 10, no. 2, 2013, pp. 200–207.
Wang, X. et al. “Cardiac autonomic function in patients with AECOPD with and without ventricular Tachycardia.” BMC Pulmonary Medicine, vol. 16, 2016, p. 75.
Desai, R. et al. “The burden and impact of arrhythmia in COPD.” International Journal of Cardiology, vol. 281, 2019, pp. 49–55.
Kumar, W. et al. “Electrocardiographic abnormalities in AECOPD.” Cureus, vol. 13, no. 12, 2021, p. e20759.
Anturlikar, S.S. et al. “A clinical study of COPD with special reference to arrhythmia.” MedPulse International Journal of Medicine, vol. 11, no. 3, 2019, pp. 175–179.
Proietti, M. et al. “Impact of COPD on prognosis in atrial fibrillation.” American Heart Journal, vol. 181, 2016, pp. 83–91.
Barrett, P.M. et al. “Comparison of 24-Hour Holter monitoring with 14-day adhesive patch ECG monitoring.” American Journal of Medicine, vol. 127, no. 1, 2014, pp. 95.e11–95.e17.
Rusinowicz, T. et al. “Cardiac arrhythmias in patients with exacerbation of COPD.” Clinical Management of Pulmonary Disorders and Diseases, Springer, 2017, pp. 53–62.
Einvik, G. et al. “Premature ventricular complex is more prevalent during AECOPD.” COPD, vol. 14, no. 3, 2017, pp. 318–323.
Kusunoki, Y. et al. “Atrial and ventricular arrhythmia-associated factors in stable COPD.” Respiration, vol. 91, no. 1, 2016, pp. 34–42.
Sakao, S. “Chronic obstructive pulmonary disease and early Cor Pulmonale.” Respiratory Investigation, vol. 57, no. 4, 2019, pp. 325–329.
Goudis, C.A. et al. “ECG abnormalities and arrhythmias in COPD.” International Journal of Cardiology, vol. 199, 2015, pp. 264–273.
Barnes, P.J. “Theophylline.” American Journal of Respiratory and Critical Care Medicine, vol. 188, no. 8, 2013, pp. 901–906.
Donohue, J.F. et al. “Long-Term safety of nebulized formoterol.” Therapeutic Advances in Respiratory Disease, vol. 2, no. 4, 2008, pp. 199–208.
Gennari, F.J. “Hypokalemia.” New England Journal of Medicine, vol. 339, 1998, pp. 451–458.
Ye, J. et al. “Impact of COPD on atrial fibrillation patient outcome: Systematic review and meta-analysis.” Heart and Lung, vol. 51, 2022, pp. 67–74.
Harvey, M.G. and R.J. Hancox. “Elevation of cardiac troponins in COPD exacerbation.” Emergency Medicine, vol. 16, no. 3, 2004, pp. 212–215.
Bhatt, S.P. et al. “Arrhythmias as trigger for acute exacerbations of COPD.” Respiratory Medicine, vol. 106, no. 8, 2012, pp. 1134–1138.
Caglar, I.M. et al. “Evaluation of atrial conduction features in COPD.” Clinical Research in Cardiology, vol. 101, no. 8, 2012, pp. 599–606.
Otake, S. et al. “Clinical Utility of ECG P-Wave Axis in COPD.” Respiration, vol. 100, no. 11, 2021, pp. 1087–1095.
Hognon, L. et al. “Heart rate variability in COPD Rehabilitation.” Frontiers in Physiology, vol. 12, 2021, p. 668343.
Wang, R.T. et al. “Mean platelet volume during AECOPD.” Respirology, vol. 18, no. 8, 2013, pp. 1244–1248.
