+91 6002993949
submission@iarconsortium.org
Open Access
ISSN (Print) : 2789-6056
ISSN (Online) : 2789-6064
Background: PHACE syndrome (posterior fossa anomalies, hemangioma, arterial lesions, cardiac abnormalities/coarctation of the aorta, eye anomalies) is characterized by large infantile hemangiomas (IH) of the face, neck, and/or scalp that are associated with developmental defects. Case Presentation: We report the case of a 75 years-old caucasian man who recently received diagnosis of possible PHACE syndrome. Conclusion: We think that clinicians, especially neurologists, should consider diagnosis of PHACE syndrome when evaluating patient with cerebral and cerebellar malformations, even without cutaneous hemangioma. We also suggest that the presence of multiple cavernous manifestations should be included among PHACE diagnostic criteria, also in adult patients
Background
PHACE syndrome (posterior fossa anomalies, hemangioma, arterial lesions, cardiac abnormalities/coarctation of the aorta, eye anomalies) is characterized by large infantile hemangiomas (IH) of the face, neck, and/or scalp that are associated with developmental defects [1]. The acronym was coined in 1996 to describe a constellation of clinical features [2].
Over 300 cases of PHACE syndrome have been reported, and it is considered one of the most common neurocutaneous vascular disorders in childhood [3]. Knowledge of the features and locations of lesions that imply a greater risk of systemic involvement is crucial for the diagnosis and proper management of PHACE syndrome patients [3].
In 2009, the diagnostic criteria for PHACE syndrome were established and then revised in 2016 by Garzon et al [1].
Mutations in a few specific regulatory genes mutually involved in capillary, neural, ophthalmologic, and sternal development have been implicated [2]. As described by Krings and colleagues, current theories on a developmental link for the abnormalities in PHACE syndrome point to neural crest [3], adjacent cephalic mesoderm, and, potentially, the neural plate to explain central nervous system (CNS) structural aberrancies but do not account for all potential abnormalities in PHACE syndrome [4]. As summarized by Hess et al., the vascular abnormalities, specifically arterial, may result from the disruption of normal arterial wall histologic architecture, leading to changes in the diameter and/or anatomic course of cerebral arteries [5]. The authors suggest that this arteriopathy during embryogenesis could lead to alterations in blood flow and, potentially, hypoxia, which could explain the formation of hemangiomas and brain structural abnormalities. Specifically, hemangiomas arise from endothelial progenitor/ stem cells derived from neural crest, and at birth, hemangiomas are “precursor” lesions that proliferate with time [4].
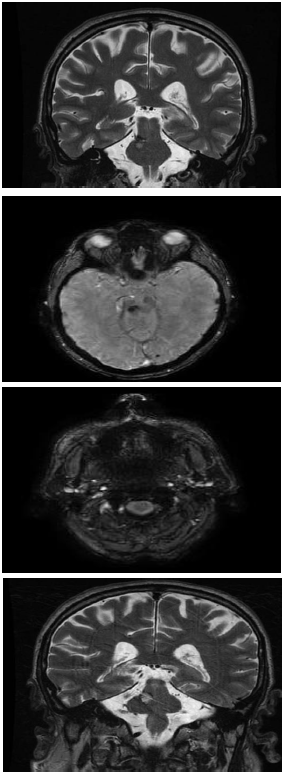
Figure 1-4: Brain MRI T2 Weighted Coronal Sequences Showing Left Vertebral Artery Hypoplasia and Right Pontine Tegmentum Cavernoma
Figure 5: Axial T1 Weighted Sequence Showing Left Cerebellar Hypoplasia
Case Presentation
We report the case of a 75 years-old caucasian man who recently received diagnosis of possible PHACE syndrome.
He was evaluated due to worsening of gait with recurrent falls. His medical history was positive for neurocognitive development delay, psychosis, left ear hearing loss. His familial history was negative. He is not married and lives alone, with two nephews grandchildren as major caregivers.
Neurological examination showed slowing down of articulatory movement with monotonous and “scanning speech”, upper limbs bilateral intention tremor, bilateral dysmetria and adyadocokinesis, marked ataxic gait, lower limbs hypotrophy with hypopallesthesia and areflexia.
No facial or neck hemangioma was present, while chest and abdomen computer tomography excluded aortic aneurism. Ocular evaluation excluded malformations. He performed brain magnetic resonance showing left cerebellar hemisphere hypoplasia, basilar artery and left vertebral artery hypoplasia, multiple cavernomas involving right pontine tegmentum (Zabramski II), left temporo-occipital and right frontal lobes (Zabramski III) (Figures 1-5). On the basis of 2016 consensus criteria and considering the presence of 2 major criterias without IH, diagnosis of possible PHACE syndrome was performed [1].
A multidisciplinary group of specialists with expertise in PHACE syndrome drafted initial diagnostic criteria which were stratified into 2 categories: (1) PHACE syndrome or (2) possible PHACE syndrome (3). Major and minor criteria were determined for the following organ systems: cerebrovascular, structural brain, cardiovascular, ocular, and ventral/midline. Definite PHACE requires the presence of a characteristic segmental hemangioma or hemangioma ≥5 cm on the face or scalp plus 1 major criterion or 2 minor criteria. Possible PHACE requires the presence of a hemangioma ≥5 cm on the face or scalp plus 1 minor criterion. The group recognized that it may be possible to have PHACE syndrome with hemangioma affecting the neck, chest, or arm only or no cutaneous hemangioma at all [1]. In our case basilar artery hypoplasia with agenesis of left vertebral artery associate with ipsilateral cerebellar hypoplasia could be considered as two major criteria which could allow us to perform diagnosis of PHACE syndrome. Unfortunately our patient presents motor and cognitive developmental delay with scarcity in compliance and he lives alone; consequently it has been difficult to perform all necessary exams for diagnosis. Ocular evaluation showed initial bilateral cataract, while chest and abdomen computer tomography excluded aortic involvement and sternal deformities. Our patient underwent neuropsychological evaluation which revealed poor trail making test (TMT) A and B performance, such as visuospatial impairment (Figure of Rey with Recall). Apparently he doesn’t present remnants of involuted cutaneous hemangioma and his two grandchildren don’t remember him with previous cutaneous manifestations.
At present, cavernous malformations are not listed among the diagnostic criteria for PHACE syndrome. To the best of our knowledge, they have not previously been reported in association with PHACE syndrome. PHACE syndrome is associated with a predominance of arterial anomalies, as opposed to other neurocutaneous disorders that involve venous and/or capillary aberrancies, including Sturge-Weber and cerebrofacial arteriovenous metameric syndrome [6-8]. In a previous study of 2016 four children (66.7 %) among six with PHACE diagnosis were found incidentally to have CCMs; all lesions measured less than 5 mm at the time of diagnosis and were asymptomatic. Consequently authors suggested the possible inclusion of other nonarterial cerebrovascular abnormalities, namely, cavernous malformations, among PHACE criteria [9].
We report a rare adult case with diagnosis of possible PHACE (or PACE considering the absence of cutaneous hemangioma) in an adult with cerebellar signs and neurocognitive impairment. We think that clinicians, especially neurologists, should consider diagnosis of PHACE syndrome when evaluating patient with cerebral and cerebellar malformations, even without cutaneous hemangioma. We also suggest that the presence of multiple cavernous manifestations should be included among PHACE diagnostic criteria, also in adult patients.
Conflict of interest
The authors declare that there is no conflict of interest regarding the publication of this Case Report.
Funding
No funding was required
Consent for Publication
Patient gave written consent
Ethical Approval
Is not required at our institution to publish an anonymous case report.
Garzon M.C. et al. "Phace syndrome: consensus-derived diagnosis and care recommendations." J Pediatr, vol. 178, 2016, pp. 24-33.e2.
Metry D.W. et al. "The many faces of phace syndrome." J Pediatr, vol. 139, no. 1, 2001, pp. 117-123.
Krings T. et al. "Segmental neurovascular syndromes in children." Neuroimaging Clin N Am, vol. 17, no. 2, 2007, pp. 245-258.
Hess C.P. et al. "Cervical and intracranial arterial anomalies in 70 patients with phace syndrome." Am J Neuroradiol, vol. 31, no. 10, 2010, pp. 1980-1986.
Frieden I.J. et al. "Phace syndrome: the association of posterior fossa brain malformations, hemangiomas, arterial anomalies, coarctation of the aorta and cardiac defects, and eye abnormalities." Arch Dermatol, vol. 132, 1996, pp. 307-311.
Rotter A. et al. "Phace syndrome: clinical manifestations, diagnostic criteria, and management." An Bras Dermatol, vol. 93, no. 3, 2018, pp. 405-411.
Brandon K. et al. "Arteriovenous malformation: a rare manifestation of phace syndrome." Pediatr Dermatol, vol. 28, 2011, pp. 180-184.
Metry D. et al. "Conference psr consensus statement on diagnostic criteria for phace syndrome." Pediatrics, vol. 124, 2009, pp. 1447-1456.
Foster K.A. et al. "Phace syndrome is associated with intracranial cavernous malformations." Childs Nerv Syst, vol. 32, no. 8, 2016, pp. 1463-1469.
