+91 6002993949
submission@iarconsortium.org
Open Access
ISSN (Print) : 2789-5998
ISSN (Online) : 2789-6005
Ureaplasma species are the most prevalent genital Mycoplasma isolated from the urogenital tract of both men and women. Ureaplasma has 14 known serotypes and is divided into two biovars- Ureaplasma parvum and Ureaplasma urealyticum, they are parasitic organisms that lack a cell wall and are thus extremely sensitive to external factors, including antibiotics. In this study, 30 samples of vaginal swabs were taken by a specialized gynecologist using sterile cotton and speculum swabs from women in the city of Mosul visiting Al-Khansa Teaching Hospital and Al-Batoul Hospital, and other outpatient clinics. Samples were collected from women who use IUDs and have not used antibiotics, from the ages between 25-40 years. PCR was used to detect the presence of Ureaplasma by targeting a specific fragment from the urease gene. The results showed that 13 samples of vaginal swabs gave a positive result indicating a presence ratio of 43% for the presence of Ureaplasma. Our results indicate that the presence of Intrauterine Device (IUD) in women is often accompanied by genital tract infections, depending on personal hygiene. Our results show that molecular detection of Ureaplasma via specific primers in PCR is efficient in the direct detection in vaginal swabs.
Mycoplasmas are the smallest free-living, self-replicating organisms. They are widespread in nature as parasites of humans, mammals, reptiles, fish, arthropods and plants [1]. Mycoplasmas are found mainly in the mouth, the upper respiratory tract, and the distal parts of the genitourinary tracts of humans. Among the genital Mycoplasmas, Ureaplasma species are the most prevalent, potentially pathogenic bacteria isolated from the urogenital tract of both men and women [2].They are also frequently associated with preterm birth and other adverse pregnancy outcomes.
Ureaplasma parvum (serovars 1, 3, 6, and 14) and U. urealyticum (serovars 2, 4, 5 and 7–13) lack cell walls, hydrolyze urea to generate ATP, have limited biosynthetic functions, adhere to human mucosal surfaces of the genitourinary tract in adults and respiratory tract in newborns and are among the smallest free-living, self-replicating cells [3]. These organisms can be detected in vaginal flora in 40–80% of healthy women and their presence has been causally linked to infertility, early pregnancy loss, stillbirth, preterm birth and neonatal morbidities [4].
The most important way of transmission of Ureaplasma bacteria is sexual intercourse, where they enter the body through the urethra (inside the penis) or vagina. Since this is the most common method of transmission, these bacteria are classified as sexually transmitted diseases From the infected mother to the fetus. The present research focuses on Ureaplasma and recent developments in its pathogenesis and diagnosis.
Collection of Clinical Specimens: Between July and November 2023, approximately 30 samples (vaginal swab) were collected from women in the city of Mosul/Iraq visiting Al-Khansa and Al-Batoul hospitals in addition to outpatient clinics. The age group was between25-40 years, and those who suffer from vaginal infections, wear an IUD, and did not administer antibiotics.
The swabs were taken using sterile cotton swabs with the help of a specialist gynecologist. Speculum was used to take the swabs in order to reduce contamination with natural flora. Samples were placed in 2mL normal saline and placed on a cool pack and transported directly to the laboratory to perform the molecular detection.
DNA Extraction
Genomic DNA was extracted directly from samples (swabs) using a genomic DNA isolation kit provided by Geneaid. Steps were followed as recommended by the manufacturer. The concentration and purity of genomic DNA were measured and the DNA was then stored at −20°C until further used. Firstly 0.9 microliters of cultured bacterial cells was add into 1.5 ml Eppendorff tubes and then place them in centrifuge at 16,000 rpm for 1 minute to sediment the bacteria and get rid of the supernatant, then 180 µl of GT buffer was add, then the tube placed in the electrophoresis. Twenty µl of Proteinase K was added to the tube containing the sediment, then incubated the tubes at a temperature of 60°C for 10 minutes, the tubes are stirred every 3 minutes. Two hundred µl of GB buffer was add to the tubes containing the sample and mixed well for 10 minutes ,then incubated at 70°C for 10 minutes .Two hundred µl of 100% ethanol, was mix well in the stirring device, and then placed the mixture in the vortex stirring device, where the mixture is then placed in the filter containing the special column and then centrifuged at 16,000 rpm for 2 minutes, the floating part was removed, then the filter containing the column was replaced with a new column. Four hundred µL was added to the mixture of W1 solution, then centrifuged at 16,000 rpm for 30 seconds and discarded the clear solution. Then 600 µl of W2 solution was added, then centrifuged and the solution was discarded while the filter was kept. Centrifugation was repeated for 3 minutes at 16,000 rpm, then 100 µL from the standard elution buffer was added to the extracted DNA and stored at -20°C. Nanodrops were used to measure the concentration and purity of DNA [6].
The primers were prepared according to the manufacturer's instructions by dissolving each primer in nuclease-free water to obtain a stock solution of 100µM according to the manufacturer, 10µM forward and reverse primers were prepared from the stock solution and used in PCR experiments [5].
Table1: Primers for Urease Gene of Ureaplasma
Primer Name | Primer Sequence 5’-3’ | Product size (bp) |
U4-F | CAATCTGCTCGTGAAGTATAA | 429 |
U5-R | ACGACGTCCATAAGCAACT |
Table2: Optimal Conditions for Conducting the PCR Reaction for the U4 and U5 Primers for Ureaplasma
Number of Cycles | time | Tem. | Stage |
1 | 1min | 95 | Denaturation |
30 | 30 sec | 56 | Annealing |
1 | 1min | 72 | Extention |
Table 3: Contents and Volumes of the Reaction Mixture
Volume in Microliters | Contents of the reaction mixture |
10 | PCR Master mix |
1 | Forward Primer |
1 | Reverse Primer |
5 | DNA template |
3 | Nuclease-free water |
20 | Total volume |
Polymerase Chain Reaction
PCR was performed in a 20 μl reaction using GoTaq G2 Green Master Mix provided by Promega (USA). Specific Primers used by were used for PCR: primers U5 (forward; 5′-CAA TCT GCT CGT GAA GTA TTA C-3′) and U4 (reverse; 5′-ACG ACG TCC ATA AGC AAC T- 3′). A 429 bp fragment of the urease gene was amplified using this primer set. The final concentration of primers used in the reaction was (1 μM each) and the total amount of template DNA (100 ng) was added as recommended by the manufacturer. The PCR program for the oligonucleotide primers sequences lambda-U5 and lambda-U4 was set as follows: initial denaturation at 95°C for 3 minutes followed by 30 cycles of amplification including a denaturation step at 95°C for 30 seconds, annealing at 55°C for 30 sec and extension at 72 °C for 1 min. The final extension step was set at 72 °C. PCR products were separated on a 1% agarose gel and stained with Midori Green Advance DNA stain. A 100 bp DNA marker (New England Biolabs, UK) was used as a molecular weight marker.
Use of PCR Master mix by Promega, USA, according to the instructions provided by the company. Each tube contained the basic components of the PCR, which are Taq DNA polymerase and a mixture of nitrogenous bases d TTP, d ATP, d CTP, d GTP. It also contains Tris-Hcl, d Gcl. MgCl, thus adding only the DNA, primers, and free nuclease water to the PCR tube to perform the PCR. Table 3 shows the total volume of the PCR mixture, which is 20 µL of DNA amplification of bacterial isolates using a thermal cycler. The PCR mixture was prepared in PCR tubes: 5 microliters of DNA, 2 microliters of primers, and 10 microliters of PCR Master mix. The volume was completed to 20 µL using nuclease-free water. The tubes were closed and transferred to a thermal cycler device to perform the polymerase chain reaction under optimal thermal conditions as shown in Table 2.
After the device stopped, the tubes were removed and the PCR products were run on1.5% agarose gels to determine the size of the amplified products. Their molecular sizes were compared to the DNA ladder with known molecular weights.
Agarose gel was prepared at a concentration of 1.5% by dissolving 1.5 g of agarose in 100 ml of TAE buffer, then heated using a microwave for a few minutes while ensuring continuous stirring to ensure that the agarose completely dissolved, agarose was then cooled to 45-50 °C, and 3µL of red safe stain was added and poured in the appropriate tray, the comb was placed inside it from one end to form the wells. The gel was poured gently from one side, avoiding the formation of bubbles, then left to harden for 30 minutes, the comb was removed and samples were placed in each well while the first well contained 5µL of the 100bp DNA Ladder. 10 µL from the amplified PCR product was mixed well and added it to the following wells. Gel was covered completely with TAE buffer prior to loading the samples [6].
The electric current used was 80-100V for 45-60 minutes. After the transfer was completed, the gel was placed inside the UV-transilluminator to see the DNA bands and to determine their sizes by comparing them with the DNA ladder used. A camera was used to photograph the gel inside a dark room.
DNA Sequencing
DNA sequences were determined to detect the identity of the urease gene sequence of the bacterial isolates. DNA sequencing was performed at Psomagene sequencing company (Maryland/ USA). The results of the polymerase chain reaction (PCR) were sent for 3 samples for the U4 and U5 genes belonging to Ureaplasma isolates. The DNA sequences of the isolates were compared with global isolates through the NCBI-Gene bank website.
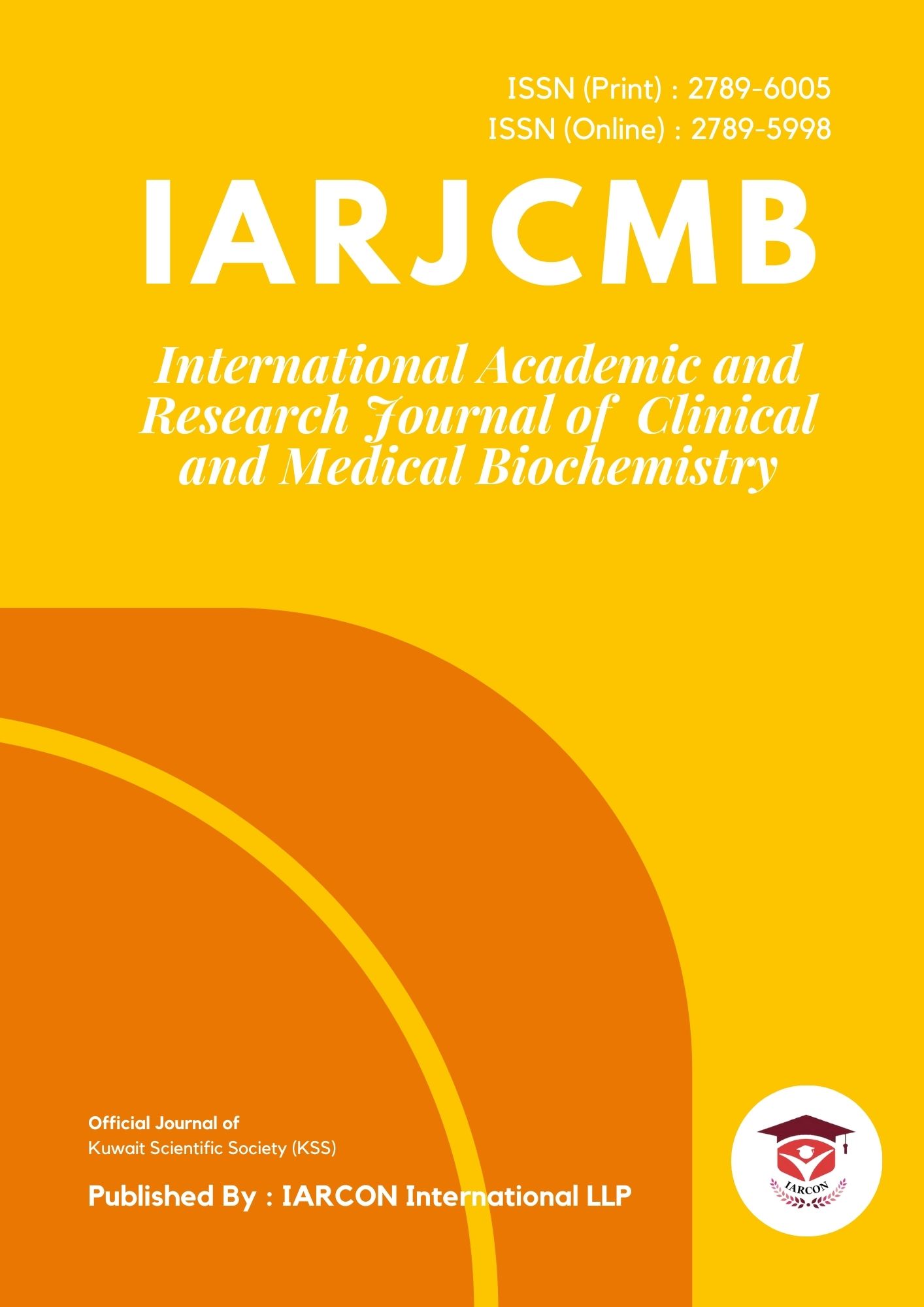
Vaginal swabs were collected from 30 women who use IUDs, and results showed that 13/30 (43%) samples of vaginal swabs were positive for growth of Ureaplasma. According to many studies, IUD users have an increased chance of developing cervical infection caused by Ureaplasma urealyticum [7]. A cross-sectional study performed by [8] in Anhui Province in China also showed that the use of an intrauterine device (IUD), male condoms, female sterilization, the rhythm method, and oral contraceptives (OC) was associated with respiratory tract infections (RTIs). The analysis showed that the use of IUD is a risk factor for cervicitis and bacterial vaginosis (BV). After the DNA was extracted, the NanoDrop was used to measure the concentration and purity, purity appeared to be 1.8-1.9. PCR was performed to detect a 426bp fragment of the urease gene specifically found in Ureaplasma, products were run on agarose gels by electrophoresis. Results showed that the product size of the amplified gene was identical as expected (426bp). PCR products of the amplified fragments are shown in the Figures 1,2,3, and 4. The size of the bands were compared to the 100bp DNA ladder.

Figure 1: PCR Product of the Gene Band size 426 bp. The Product was Electrophoresis on 1.5% Agarose at7 volt/cm2. 1x TBE Buffer for 1:30 hours. N: DNA ladder (100bp)
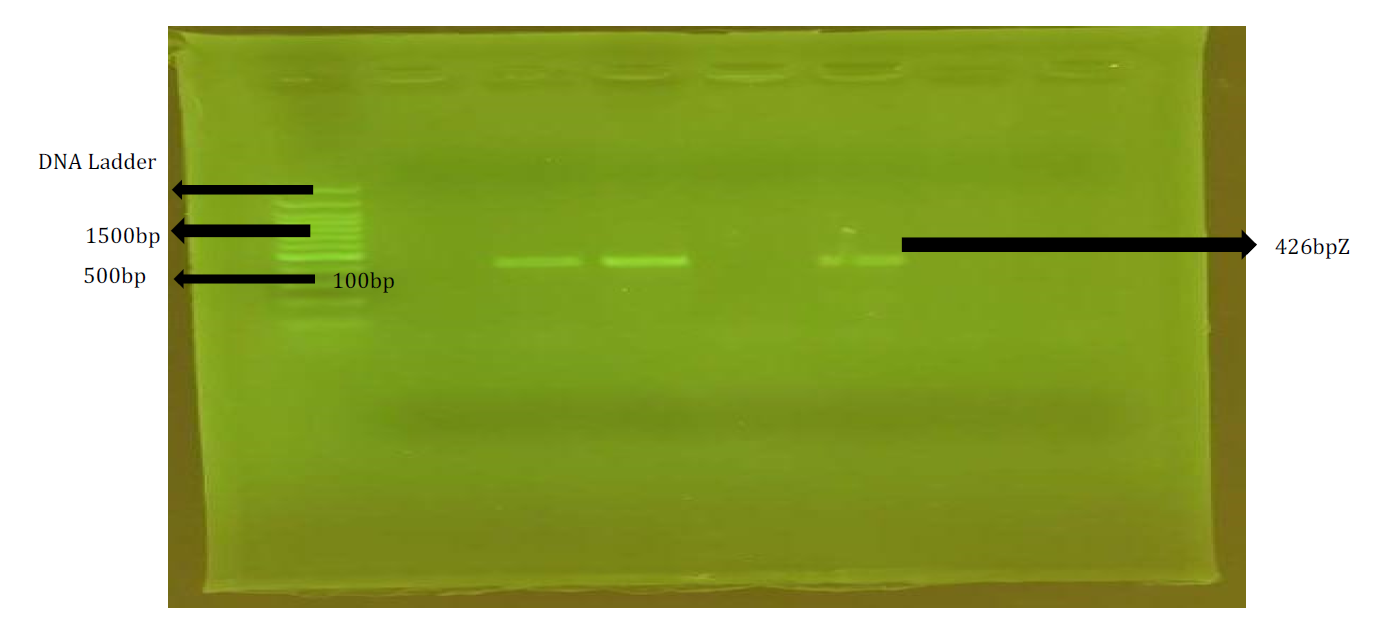
Figure 2: PCR Product of the Gene Band size 426 bp. The Product was Electrophoresis on 1.5% Agarose at7 volt/cm2. 1x TBE buffer for 1:30 Hours. N: DNA ladder (100bp)
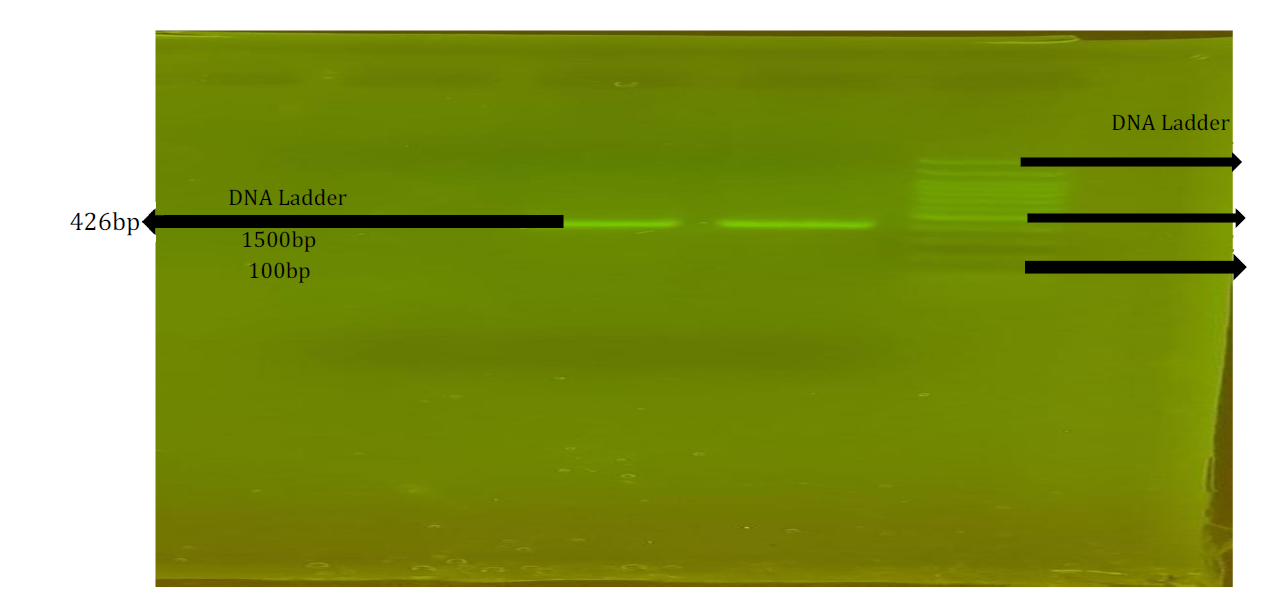
Figure 3: PCR Product of the Gene Band size 426 bp. The Product was Electrophoresis on 1.5% Agarose at7 volt/cm2. 1x TBE Buffer for 1:30 Hours. N: DNA Ladder (100bp)
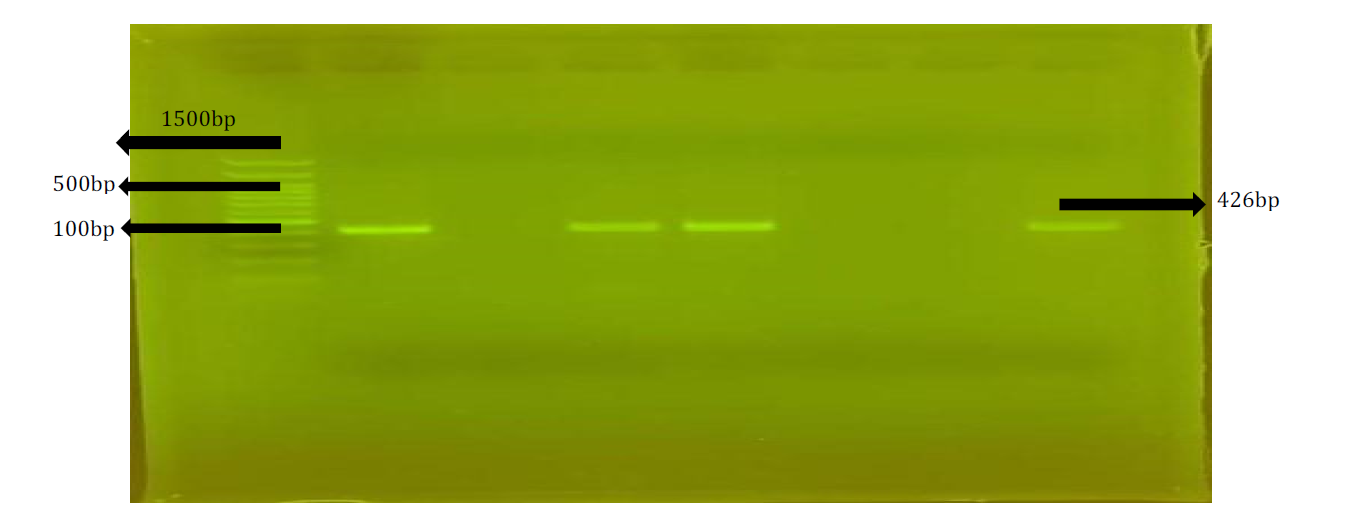
Figure 4: PCR Product of the Gene Band Size 426 bp. The Product was Electrophoresis on 1.5% agarose at7 volt/cm2. 1x TBE buffer for 1:30 hours. N: DNA Ladder (100bp)
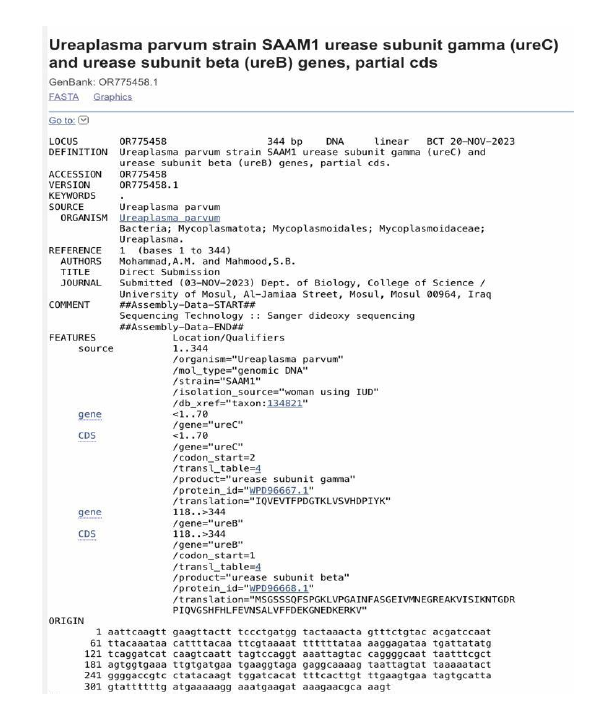
Figure 5: NCBI Submission of UreB and UreC Fragment from U. Parvum SAAM1
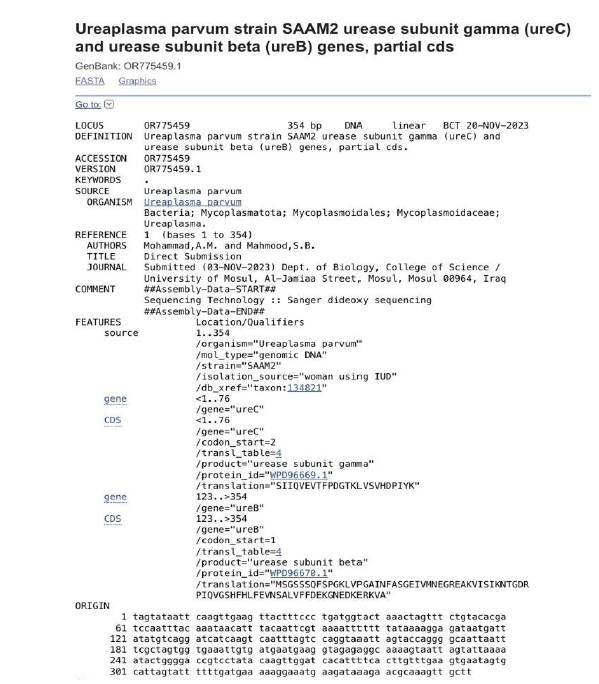
Figure 6: NCBI Submission of ureB and ureC Fragment from U. Parvum SAAM2
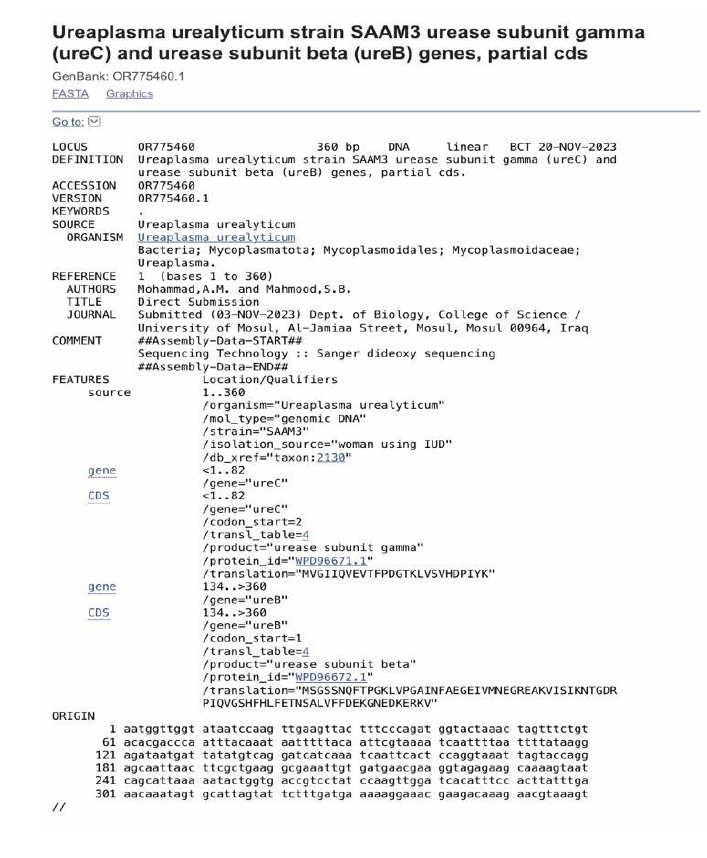
Figure 7: NCBI Submission of UreB and UreC Fragment from U. Urealyticum SAAM3
In order to confirm the detection, PCR products of the amplified urease gene detected in this study were subjected to Sanger sequencing and their sequences were compared to sequences submitted to the NCBI database to determine the identity of the bacterial species. Analysis of gene sequences obtained from swab samples showed that the product amplified was a fragment from the ureB and ureC gene subunits of the urease gene belonging to U. parvum and U. urealyticum. The sequence of the fragment was submitted to NCBI under the accession numbers OR7754458.1, OR7754459.1, and OR7754460.1 as shown in Figure 5-7.
IUDs are popular contraceptive choices for women however, the possible risk of PID associated with the use of an IUD has been a long-lasting important concern throughout the world. The connection between the development of any upper genital tract infection immediately after the insertion of the IUD, or due to the extended duration of IUD in place has been studied extensively during the past decades, but controversial results were obtained [9]. Although higher rates of PID immediately after insertion of IUDs has been noted in previous studies, some recent data allow for a finer analysis of this relation [10-11].
There is limited evidence regarding the association between a history of sexually transmitted infections (STIs) and the risk of Ureaplasma infection or IUD expulsion. Study in 2019 of [12] found that Ureaplasma urealyticum infection was significantly associated with factors such as intrauterine device (IUD) use, number of sexual partners, and age (<35 years).
In our study, samples were collected from women who use IUDs and do not use antibiotics using vaginal swabs sterile dry swabs can be used to detect Ureaplasma. Studies have shown that Ureaplasma can be detected using dry swabs without the need for transport media or liquid culture [13]. The accuracy of detection using dry swabs has been compared to other methods such as eSwab® and liquid culture, and the results have shown that dry swabs are effective in detecting Ureaplasma [14-15].
Therefore, sterile dry swabs can be a reliable and convenient method for detecting Ureaplasma infections and Using a speculum, as the potential risks and benefits of using a speculum to take vaginal swabs vary based on the design and use of the speculum. Some potential benefits include improved vision and access to the cervix, allowing for more accurate diagnosis and treatment [16]. In addition, adding a magnifier to the endoscope can enhance the monitoring of health and disease conditions in the body [17]. On the other hand, there are potential risks associated with using an endoscope. Current standard laparoscopy is not specialized enough to be used for all populations, such as obese patients, resulting in discomfort and inadequate care [18].
DNA extraction from Ureaplasma was performed in several studies [19]. Examined the DNA relatedness among different sero-groups and species of Ureaplasma [20]. Described a simple technique for culturing and isolating DNA from Mycoplasma hominis and Ureaplasma urealyticum [21].
DNA extracted from Ureaplasma has potential applications in various areas. One potential application is the development of a Ureaplasma urealyticum detection kit, which can rapidly and accurately detect Ureaplasma urealyticum -DNA in unknown samples such as genital tract secretions [22]. Another application is the development of DNA macroarrays, which enable rapid acquisition of information on changes in the microbial genome [23]. Additionally, DNA extracted from ureaplasma bacteria can be used for the prevention and/or treatment of Ureaplasma infections, including the development of vaccines [24]. Furthermore, DNA-based typing systems can be used to identify and subtype different Ureaplasma species and subtypes, providing a basis for studying the relationship between these bacteria and human diseases [25].
Nanodrops can be used to measure the concentration and purity of DNA. One method involves using a nanopore sensor, where a DNA solution is inputted into a vessel with nanopore membranes. Voltage is applied to electrodes, allowing the DNA to pass through the nanopores and move. The current of each ion passing through the nanopore membranes is measured, and the DNA concentration is obtained from these measurements [6].
Ureaplasma urealyticum in clinical samples can be rapidly, sensitively and accurately detected by using the specific primer pair disclosed by the invention, so that the primer pair has great significance in the early diagnosis, timely treatment and effective control of reproductive tract infection caused by Ureaplasma urealyticum [26].
Ureaplasma has unique genes that have evolved in a species-specific manner, particularly in transcription-related genes, uracil-DNA glycosylase, and glycolytic genes [27-28]. Ureaplasma has a unique ATP synthesis system coupled to urea hydrolysis, which leads to the breakdown of the glycolysis pathway. Ureaplasma urease genes have a unique evolutionary process and can be used as a diagnostic indicator for Ureaplasma strains.
There are 14 known serotypes of Ureaplasma species listed in the NCBI database.
In addition, M. hominis, U. urealyticum, M. genitalium have also been reported to be associated with some cases of pelvic inflammatory diseases (PID). How the frequency of the use of IUD and the bacteria, which may form a biofilm on it, influences the development of upper genital tract infection, is still a question.
Our study confirms the hypothesis that IUDs, independent of the type or duration of use can increase the possibility of an up-spreading gynecological infection. It is a therapeutic challenge to manage these cases because of the mixed bacterial biofilm flora found on the implant’s surface.
Funding
None to declare.
Conflict of Interest
Authors declare that they have no conflicts of interest.
Waites, K.B. et al. “Mycoplasma and Ureaplasma.” Manual of Clinical Microbiology, edited by P.R. Murray et al., 9th ed., ASM Press, 2007, pp. 1004–1020.
Cassell, G.H. et al. “Ureaplasma urealyticum intrauterine infection: Role in prematurity and disease in newborns.” Clinical Microbiology Reviews, vol. 6, 1993, pp. 69–87.
Waites, K.B. et al. “Molecular methods for the detection of Mycoplasma and Ureaplasma infections in humans.” Journal of Molecular Diagnostics, vol. 14, 2012, pp. 437–450.
Viscardi, R.M. “Ureaplasma species: Role in diseases of prematurity.” Clinics in Perinatology, vol. 37, 2010, pp. 393–409.
Khaleel, A.M. et al. “The efficiency of molecular methods compared to traditional methods in identifying bacteria from blood and cerebrospinal fluid samples.” Malaysian Journal of Microbiology, vol. 19, no. 2, March 2023.
Abdulrazzaq, R. et al. “Efficiency of hichrome Enterococcus faecium agar in the isolation of Enterococcus spp.” Journal of Life and Bio Sciences Research, vol. 3, no. 1, January 2022, pp. 1–6.
Vanja, K. et al. “An intrauterine device as a possible cause of change in the microbial flora of the female genital system.” Journal of Obstetrics and Gynaecology Research, vol. 37, no. 8, 2011, pp. 1035–1040.
Wang, L.-Y. et al. “The effect of contraceptive methods on reproductive tract infections risk.” Archives of Gynecology and Obstetrics, vol. 294, no. 6, 2016, pp. 1249–1256.
Hubacher, D. et al. “Pitfalls of research linking the intrauterine device to pelvic inflammatory disease.” Obstetrics & Gynecology, vol. 121, 2013, pp. 1091–1098.
Viberga, I. et al. “Microbiology profile in women with pelvic inflammatory disease in relation to IUD use.” Infectious Diseases in Obstetrics and Gynecology, vol. 13, 2005, pp. 183–190.
Hubacher, D. “Intrauterine devices and infection: Review of the literature.” Indian Journal of Medical Research, vol. 140, 2014, pp. S53–S57.
Puri, M. et al. “Provider and women characteristics as risk factors for postpartum copper IUD expulsion and discontinuation in Nepal.” International Perspectives on Sexual and Reproductive Health, vol. 46, 2020, pp. 235–245.
Pichon, M. et al. “Which sample for the transport of Mycoplasma, eSwab® or dry swab?” Annales de Biologie Clinique, vol. 77, no. 1, 2019, pp. 95–98.
Hong, X. et al. “A preliminary study on the associations between Ureaplasma, Mycoplasma and the vaginal microbiome.” Medical Mycology, 2021, article 100041.
Biros, E. et al. “Molecular detection of Ureaplasma urealyticum infection from clinical urogenital swabs.” Folia Microbiologica, vol. 52, no. 4, 2007, pp. 443–446.
Wong, K. et al. “The vaginal speculum: A review of literature focusing on specula redesigns and improvements to the pelvic exam.” Undergraduate Research Journal, vol. 5, no. 1, 2021.
Guo, Y. et al. “Gynaecological vaginal speculum.” 2012.
Dixon, R.A. et al. “A vaginal speculum.” 2010.
Harasawa, R. et al. “DNA relatedness among established Ureaplasma species and unidentified feline and canine serogroups.” International Journal of Systematic and Evolutionary Microbiology, vol. 40, no. 1, 1990, pp. 52–55.
Harasawa, R. et al. “DNA relatedness among established Ureaplasma species and unidentified feline and canine serogroups.” International Journal of Systematic and Evolutionary Microbiology, vol. 40, no. 1, 1990, pp. 52–55.
Walther, T. et al. “A simple technique to isolate DNA and supernatant of genital Mycoplasma hominis and Ureaplasma urealyticum.” Journal of Perinatal Medicine, vol. 26, no. 2, 1998, pp. 123–124.
Khaleel, A.M. et al. “Using recombinant DNA technology in bacterial identification from vaginal swabs.” Revista Bionatura, vol. 8, no. 3, 2023, pp. 113.
Dai, L. et al. “UU (Ureaplasma urealyticum) detection kit.” 2013.
Klyubin, A.V. et al. “Development of DNA macroarrays for genome scanning of Ureaplasma parvum strains.” Microbiology, vol. 78, no. 6, 2009, pp. 717–722.
Weisman, L.E. et al. “Ureaplasma vaccine and antibodies.” 2015.
Kim, D. et al. “DNA method and apparatus for measuring DNA droplet concentration.” 2020.
Diker, K.S. “Molecular diagnosis of bovine genital Mycoplasma and Ureaplasma infections by PCR.” Harran Üniversitesi Veteriner Fakültesi Dergisi, 2023.
Oshima, K. et al. “Detection of the genes evolving under Ureaplasma-specific selection.” Journal of Molecular Evolution, vol. 66, no. 5, 2008, pp. 529–532.
Nishida, H. “Ureaplasma urease genes have undergone a unique evolutionary process.” The Open Systems Biology Journal, vol. 2, no. 1, 2009, pp. 1–7.
