
+91 6002993949
submission@iarconsortium.org
Open Access
ISSN (Print) : 2788-9475
ISSN (Online) : 2788-9483
Background: Acute lower respiratory tract infection is the leading cause of mortality and one of the common causes of morbidity in children under-five years of age. Aim: The aim of the present study is to provide a comprehensive description of the pattern of lower respiratory tract infections (LRTIs) in children under 5 years of age attended Children Hospital in Kirkuk City including the investigation of the frequency, severity, and types of LRTIs prevalent. Patients and Methods: This descriptive epidemiologic-observational, cross-sectional hospital-based study was conducted in Kirkuk city from November 1, 2023, to March 31, 2024. A total of 267 children below five years old, admitted with acute lower respiratory tract infections to the emergency department and pediatric wards of Children Hospital in Kirkuk city, were included in the study. Consecutive non-probability sampling was employed, including all eligible patients over one autumn and one winter season to account for potential seasonal variations in respiratory infections. Children under 5 years presenting with acute symptoms of cough and rapid respiration or difficulty in breathing, consistent with WHO criteria for ALRI, were included. The clinical history included recurrent chest infections, asthma, drug or food allergies, steroid use, cow milk allergies, atopic conditions, family history of allergies and LRTIs, and vaccination history. Diagnosis of lower RTIs was based on specific clinical signs such as tachypnea, chest wall indrawing, abnormal auscultatory findings (e.g., wheezes, crepitations, or bronchial breath sounds), and abnormal chest X-rays. Results: The study investigated factors influencing the duration of lower respiratory tract infections (LRTI) in children, revealing that infants (0-12 months) are the most vulnerable, comprising 68.54% of cases, with infection rates decreasing as age increases. Males had a higher prevalence (57.68%), and urban children showed a higher prevalence (74.16%) than rural children. Although urban children had a slightly shorter illness duration (7.52 days) compared to rural children (7.83 days, p = 0.67), no significant association was found between maternal education level and illness duration (p = 0.61). Feeding type significantly impacted illness duration (p = 0.023), with bottle-fed children experiencing the longest illness duration (8.74 days) and exclusively breastfed children the shortest (6.75 days). Children with a history of steroid use had significantly longer illness durations (p = 0.0011), whereas factors such as history of asthma, allergies, and vaccine status did not show significant differences. Common symptoms lasted around 7-8 days, with productive cough being the shortest (5.75 days). Most children (69.40% of 0-12 months) stayed in the hospital for 1-3 days. The study highlights the need for early intervention and tailored care based on demographic and socio-economic factors to effectively manage LRTI in children.
Acute lower respiratory tract infection is the primary cause of death and a frequent cause of illness in children under the age of five. Respiratory infections are a diverse and intricate collection of disorders caused by a wide array of pathogens, including viruses, bacteria, and fungus (1). The lower respiratory tract comprises the trachea, bronchi, bronchioles, and alveoli. In 2015, pneumonia was responsible for the deaths of 9,20,136 children under the age of 5, which accounted for 16% of all fatalities in this age group (2). Untreated respiratory infections in young children can have life-threatening consequences. Acute respiratory infection is more prevalent in underdeveloped nations than to industrialized countries. The increased occurrence is ascribed to factors such as overcrowding, high HIV prevalence, low birth weight, and the absence of pneumococcal and measles vaccination (3). Additionally, variables such as zinc and vitamin A insufficiency, low maternal education, and residing in locations with high pollution levels all contribute to the problem. While the exact cause of pneumonia is often unknown in a clinical setting, the primary culprits responsible for this condition in children are often Streptococcus pneumoniae, Hemophilus influenzae, and to a lesser degree, Staphylococcus aureus. Bronchiolitis is a significant contributor to child mortality. RSV is involved in the majority of cases. Additional viruses in this category are parainfluenza virus 1, 2, and 3, adenovirus, and influenza virus (4). Research has demonstrated the significance of socioeconomic determinants in relation to mortality and morbidity caused by acute respiratory infections (ARI), such as the number of individuals in a household, level of education, and population density in the place of residence. Therefore, it is crucial to prioritize social elements while contemplating preventative interventions. According to reports, the prevalence of Acute Respiratory Infections (ARI) is higher in urban regions and slums compared to rural areas. The expenses associated with lower respiratory tract infection in both outpatient and hospital settings impose a significant financial burden on national healthcare budgets (5,6). When dealing with instances of lower respiratory tract infections (LRTI), it is crucial to focus on modifiable risk factors including as breastfeeding, overcrowding, undernutrition, delayed weaning, and prelacteal feeding. IMNCI categorizes cases into four classifications based on respiratory rate, presence or absence of chest retraction, and general patient status: no pneumonia, pneumonia, severe pneumonia, and very severe pneumonia. Treatment options encompass the administration of oral antibiotics. Severe cases necessitate hospitalization and the use of intravenous antibiotics, as well as other supportive measures like as oxygen/ventilator support and ICD draining (7,8). Respiratory infections pose a significant problem in children and adolescents. Recurrent respiratory illnesses impose both financial strain on parents and contribute to increased absenteeism from school. This study aimed to determine the distribution pattern of lower respiratory tract infection and its associated risk factors, as well as identify the bacterial pathogens responsible for it (9,10). The aim of the present study is to provide a comprehensive description of the pattern of lower respiratory tract infections (LRTIs) in children under 5 years of age attended Children Hospital in Kirkuk City including the investigation of the frequency, severity, and types of LRTIs prevalent.
This descriptive epidemiologic-observational, cross-sectional hospital based study was carried out in Kirkuk city from the period 1st November 2023 to the end of March 2024.
The study included 267 children with age below five years old who admitted with acute lower respiratory tract infections to the emergency department of and pediatric wards of Children Hospital in Kirkuk city. The sampling method employed was consecutive non-probability sampling, where patients meeting the selection criteria over the study period were included. The study encompassed one autumn and one winter season to capture potential seasonal variations in respiratory infections.
Inclusion criteria
Children younger than 5 years old who had a recent history of coughing and fast breathing or trouble breathing were included in the study based on WHO guidelines for ALRI (21). Additionally, patients with indications of lower RTIs, such as bronchitis, bronchiolitis, and pneumonia, were included.
Exclusion criteria
Children with congenital heart disease, hypotonia , cerebral palsy, peripheral circulatory failure, severe anemia, dehydration and Asthma were excluded.
Ethical approval
Approval of the council of College of Medicine/ Tikrit University was obtain for the proposal of the study .
Approval permission was presented to the director of Kirkuk Health directorate
Questionnaire was developed by the researcher for the purpose of the study to assess the domains related to LRTI children included Age, Gender, Residence, Clinical features
Informed consent was obtained from guardians after thorough explanation of the study's objectives.
History of recurrent chest infections, asthma, allergies to drugs or food, steroid use, cow milk allergies, atopic conditions, family history of allergies, family history of LRTIs, history of vaccinations, asthma, known allergies to drugs or food, history of steroids use, cow milk allergies, atopic conditions in the child or family members, family history of allergies and LRTIs, and following vaccination schedules.
Some of the signs that helped doctors figure out that someone had a lower RTI were tachypnea, chest wall indrawing, abnormal auscultatory finds (like wheezes/crepitations or bronchial breath sounds), and abnormal chest X-rays.
Data underwent meticulous scrutiny for completeness and logical consistency prior to analysis. Pre-coded data were entered into Microsoft Office Excel Software Program 2019 and later transferred to the Statistical Package for Social Science version 26 for comprehensive statistical analysis. Descriptive statistics were utilized to portray qualitative variables in terms of frequencies and percentages. The chi-square and Fisher exact tests were employed to ascertain significance levels (p < 0.05).
The study found that infants are highly vulnerable, with 68.54% of cases occurring between 0-12 months. As age increases, infection rates decrease with mean age 10.2 ± 2.1 moths. Males had a higher prevalence of 57.68% cases, while urban children had a higher prevalence of 74.16%.
Table 1: Demographic characteristics of children with LRTI
Demographic characteristics of children with respiratory tract infection | No. | % | |
Age range (months) | 0-12 | 183 | 68.54% |
13-24 | 49 | 18.35% | |
25-36 | 23 | 8.61% | |
37-48 | 12 | 4.49% | |
Gender | Male | 154 | 57.68% |
Female | 113 | 42.32% | |
Residence | Urban | 198 | 74.16% |
Rural | 69 | 25.84% | |
Total | 267 | 100% | |
The data reveal that the majority of mothers (46.07%) were classified as illiterate, followed by those with primary education (23.97%), secondary education (12.73%), and college education (17.23%), Figure 1
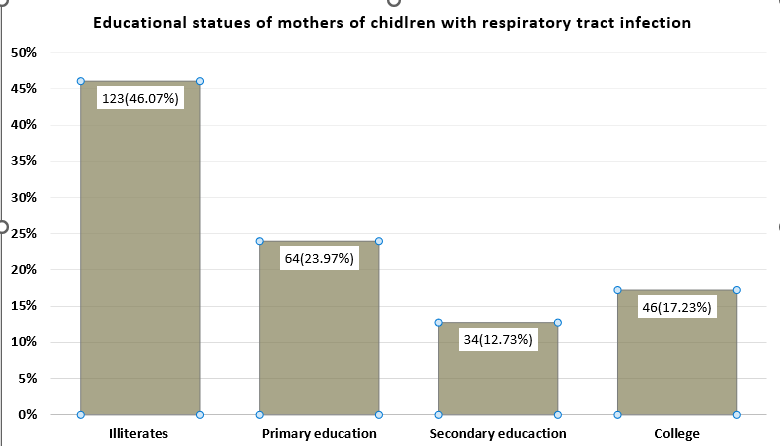
Figure 1: Distribution of LRTI children according to educational statues of mothers
The study categorizes children into rural and urban areas based on their residence. Rural children had a mean duration of illness of 7.83 days, while urban children had a slightly shorter duration of 7.52 days. The p-value was calculated to be 0.67. The study found a significant difference in illness duration between rural and urban children, Table 2
Table 2: Relation of duration of illness with residence of LRTI children
Residence | No. | Duration of illness (days) Mean±SD |
Rural | 69 | 7.83±4.54 |
Urban | 198 | 7.52±5.39 |
P-value: 0.67
The mean duration of illness is 7.04 days for children with college-educated mothers, 7.37 days for children with illiterate mothers, 7.77 days for children with primary education-educated mothers, and 8.90 days for children with secondary education-educated mothers. However, a p-value of 0.61 suggests no significant association between maternal education and illness duration, Table 3.
Table 3: Relation of duration of illness with mother educational status of LRTI children
Educational statues of mother | No. | Duration of illness (days) Mean±SD |
College | 46 | 7.04±4.22 |
illiterates | 123 | 7.37±5.63 |
Primary | 64 | 7.77±4.41 |
Secondary | 34 | 8.90±5.93 |
P-value: 0.61
The study found a significant association between the type of feeding and the duration of illness in LRTI children. Bottle-fed children had the longest illness duration at 8.74 days, while exclusively breastfed children had the shortest at 6.75 days. Mixed feeding and solid food children had shorter durations at 7.34 and 7.05 days, respectively, Table 4
Table 4: Relation of duration of illness with feeding types of LRTI children
Type of feeding | No. | Duration of illness (days) Mean±SD |
Bottle feeding | 86 | 8.74±5.46 |
Breast feeding | 39 | 6.75±5.23 |
Mixed feeding | 60 | 7.34±5.13 |
Solid Food (normal feeding) | 82 | 7.05±4.91 |
P-value: 0.023
Children with a history of asthma had a shorter mean duration of illness. However, children with a history of using steroids had a significantly longer mean duration of illness. Similarly, children with a family history of allergy had a longer mean duration of illness. However, there were no significant differences in illness duration based on receiving vaccines, Table 5
Table 5: Relation of duration of illness with clinical characteristics
Clinical characteristics | No. | Duration of illness (days) | P-value | |
Recurrent chest infection | Yes | 136 | 7.99±5.29 | 0.18 |
No | 131 | 7.10±5.05 | ||
History of asthma | Yes | 36 | 7.86±4.40 | 0.12 |
No | 231 | 7.56±5.30 | ||
History of allergy to drug or food | Yes | 53 | 7.61±4.13 | 0.98 |
No | 214 | 7.60±5.42 | ||
History of using steroid | Yes | 24 | 10.1 ±6.04 | 0.0011 |
No | 243 | 7.37±5.04 | ||
Received vaccine | Yes | 207 | 7.23±4.94 | 0.24 |
No | 60 | 8.89±5.79 | ||
The mean duration of fever is 7.80 days, while loss of appetite has a slightly longer mean duration of 7.97 days. Vomiting lasts for an average of 7.73 days. The duration of a productive cough is notably shorter, averaging 5.75 days, compared to a dry cough which averages 7.65 days . Other symptoms like a runny nose and tachypnea persist for 7.39 days and 7.60 days respectively. Wheezing and cyanosis have mean durations of 7.70 days and 7.24 days respectively, while dyspnea lasts for an average of 7.63 days, Table 6
Table 6: Relation of duration of illness with signs and symptoms of LRIT
signs and symptoms of children with LRTI | Duration of illness (days) (Mean±SD) |
Fever | 7.80±5.20 |
loss of appetite | 7.97±5.41 |
Vomiting | 7.73±5.72 |
Productive cough | 5.75±2.87 |
Dry cough | 7.65±5.24 |
runny nose | 7.39±5.30 |
Tachypnea | 7.60±5.01 |
Wheezing | 7.70±5.35 |
Cyanosis | 7.24±5.30 |
dyspneic | 7.63±5.00 |
The study showed that infants aged 0-12 months exhibit the highest incidence of symptoms, with vomiting (74.42%), tachypnea (71.70%), wheezing (68.31%), loss of appetite (67.12%), and productive cough (67.19%) being particularly common. Recurrent chest infections are also prevalent in this age group at 49.26%. As children age, the prevalence of these symptoms generally decreases. For instance, in children aged 13-24 months, the rates drop notably for all symptoms, with vomiting at 15.70% and fever at 20.63%. Dry cough is unique in its distribution, being present equally in the youngest two age groups (50%) but absent in the older groups, Table 7
Table 7: Relation between clinical features of LRTI children with age
Clinical features of children with LRTI | Age range (months) | |||
0-12 months | 13-24 months | 25-36 months | 37-48 months | |
Recurrent chest infection | 49.26% | 26.47% | 15.44% | 8.82% |
Fever | 64.57% | 20.63% | 9.87% | 4.93% |
loss of appetite | 67.12% | 19.18% | 9.59% | 4.11% |
vomiting | 74.42% | 15.70% | 7.56% | 2.33% |
Dry cough | 50% | 50% | 0% | 0% |
Productive cough | 67.19% | 19.14% | 8.98% | 4.69% |
runny nose | 60.92% | 20.11% | 12.64% | 6.32% |
Tachypnea | 71.70% | 18.40% | 7.08% | 2.83% |
wheezing | 68.31% | 18.11% | 8.64% | 4.94% |
The study showed that most children with lower respiratory tract infections (LRTIs) stay in the hospital for 1-3 days, with 69.40% of children aged 0-12 months, 69.39% of those aged 13-24 months, 69.57% of those aged 25-36 months, and 75% of those aged 37-48 months staying in the hospital. Table 8
Table 8: Relation between duration of hospital stays of LRTI children with age
duration of hospital stays | Age range (months) | |||||||
0-12 | 13-24 | 25-36 | 37-48 | |||||
No. | % | No. | % | No. | % | No. | % | |
1-3 | 127 | 69.40% | 34 | 69.39% | 16 | 69.57% | 9 | 75% |
4-6 | 44 | 24.04% | 14 | 28.57% | 6 | 26.09% | 3 | 25% |
7-10 | 8 | 4.37% | 1 | 2.04% | 1 | 4.35% | 0 | 0% |
>10 | 4 | 2.19% | 0 | 0% | 0 | 0% | 0 | 0% |
Total | 183 | 100% | 49 | 100% | 23 | 100% | 12 | 100% |
P-value: 0.65
The study found that kids with lower respiratory tract infections (LRTIs) were sick for an average of 7.83 days in rural areas and 7.52 days in urban areas, with a p-value of 0.67 the difference. This means that there isn't a statistically significant difference in the length of illness based on where someone lives, even though there is a small number difference. These results are similar to those of other studies that looked at how location affects the length and severity of respiratory illnesses in kids. A study by Nair et al. (1) and Yang et al. (2) explored the incidence and duration of respiratory infections among children in different regions and found no significant difference in the duration of illness between urban and rural children. The researchers suggested that while access to healthcare and socioeconomic factors can vary, these do not necessarily translate into differences in illness duration for LRTIs when healthcare access is sufficiently available in both settings. Further, a systematic review by Cortes-Ramirez et al. (3) looked at pediatric respiratory illnesses in various demographic contexts, including urban and rural settings. The review found that while rural children might have higher initial rates of infection due to factors like higher exposure to indoor pollutants from biomass fuel use, the course of the illness, including duration, did not differ significantly from urban children when both groups received timely and adequate medical treatment.
The study's findings indicated that the mean duration of illness for children with lower respiratory tract infections (LRTIs) varies slightly based on the education level of their mothers: 7.04 days for children with college-educated mothers, 7.37 days for children with illiterate mothers, 7.77 days for children with mothers who completed primary education, and 8.90 days for children with mothers who completed secondary education. However, the p-value of 0.61 suggests that these differences are not statistically significant, indicating no substantial association between maternal education and the duration of illness. This conclusion aligns with existing research in the field. A study by Bush et al. (4) examined the impact of parental education on health outcomes in children, particularly focusing on respiratory infections. The researchers found that while higher maternal education levels are generally associated with better overall health outcomes and more effective management of illnesses due to increased health literacy and better access to healthcare resources, the duration of specific illnesses like LRTIs did not show significant variation. The study's finding indicated that the type of feeding significantly affects the duration of illness in children with lower respiratory tract infections (LRTIs) is consistent with existing research. Specifically, the study reported that bottle-fed children had the longest duration of illness at 8.74 days, while exclusively breastfed children had the shortest at 6.75 days. Breastfeeding is widely recognized for its protective effects against various infections, including respiratory tract infections. According to a study by Lee and Binns (5), exclusive breastfeeding provides infants with essential nutrients and antibodies that enhance their immune response, leading to shorter and less severe illnesses. The antibodies and immune factors present in breast milk help to protect infants from pathogens and boost their immune systems, which can result in a quicker recovery from infections like LRTIs. A comprehensive review by Victora et al. (6) also supports these findings. The review analyzed numerous studies on breastfeeding and child health outcomes and found that exclusively breastfed infants had lower rates and shorter durations of respiratory infections compared to those who were bottle-fed or mixed-fed. This can be attributed to the unique composition of breast milk, which includes immunoglobulins, lactoferrin, and other bioactive molecules that provide direct antimicrobial effects and enhance the infant's immune system. Moreover, the difference in illness duration between exclusively breastfed and bottle-fed children can also be attributed to other factors associated with feeding practices. Breastfeeding promotes better overall health and nutritional status, which can strengthen the child's immune system. In contrast, bottle-fed infants might be exposed to higher risks of contamination and less optimal nutrition, which can adversely affect their ability to recover from infections (1,2). The study's findings indicated that various factors, including a history of asthma, use of steroids, and a family history of allergies, influence the duration of illness in children with lower respiratory tract infections (LRTIs). These findings align with existing research that explores how these variables impact the clinical course of respiratory illnesses in children. Children with a history of asthma had a shorter mean duration of illness. This might seem counterintuitive, as asthma is a chronic condition that often complicates respiratory infections. However, it is possible that these children are more frequently monitored and receive prompt and effective treatment when respiratory symptoms arise. Studies like that by Papi et al. (7) suggested that children with asthma often have personalized asthma action plans, leading to quicker intervention and management of symptoms, which could result in shorter illness durations. Conversely, children with a history of using steroids had a significantly longer mean duration of illness. Steroids are often prescribed for severe asthma and other inflammatory conditions to reduce inflammation and immune response(8). While effective in controlling chronic conditions, steroids can suppress the immune system, potentially leading to prolonged recovery from acute infections. A study by Lin et al. (9) and Chellappan et al. (10) have indicated that steroid use can delay the resolution of infections due to its immunosuppressive effects, which can extend the duration of respiratory illnesses like LRTIs. Children with a family history of allergies also experienced longer mean durations of illness. Allergic conditions often reflect an underlying hyperreactive immune system, which can exacerbate and prolong the inflammatory response during infections (1). According to a study by Edwards et al. (12) children with familial allergies may have more intense and prolonged inflammatory responses, leading to longer durations of respiratory illnesses. Interestingly, the study found no significant differences in illness duration based on receiving vaccines. This might be because vaccines are primarily designed to prevent the onset of specific infections rather than reduce the duration of illness once an infection has occurred (12). In the current study findings , the mean duration of LRTI children who suffered form fever at 7.80 days, this was in consistent with studies indicating that fever is often one of the primary and prolonged symptoms of respiratory infections. A study by Nijman et al (13) noted that fever can persist for about a week in pediatric lower respiratory infections. Fever can persist for about a week in pediatric lower respiratory infections due to the nature of these infections and the physiological responses in children. Viral infections, such as those caused by respiratory syncytial virus (RSV) or influenza, are common culprits and tend to result in prolonged fever as the immune system works to clear the virus. Bacterial infections, like bacterial pneumonia, can also cause sustained fever as antibiotics take time to combat the bacteria effectively. Additionally, children's immune systems are still developing, which can lead to a more prolonged inflammatory response(14,15,16).
The study found that infants aged 0-12 months have the highest incidence of lower respiratory tract infection symptoms, including vomiting (74.42%), tachypnea (71.70%), wheezing (68.31%), loss of appetite (67.12%), and productive cough (67.19%). Recurrent chest infections are prevalent in this age group (49.26%). Symptoms decrease as children age, with vomiting at 15.70% and fever at 20.63% in those aged 13-24 months. Dry cough is equally common in the youngest two age groups but absent in older ones. Infants aged 0-12 months exhibit the highest incidence of symptoms, reflecting their vulnerability to respiratory infections due to immature immune systems and smaller airways (17,18,19). Studies done by Penela-Sánchez et al.(20) and Brittan et al. (21) have similarly found that infants are at the highest risk for respiratory illnesses, with symptoms like vomiting, tachypnea, wheezing, loss of appetite, and productive cough being commonly reported. This age-related decline in symptom prevalence is consistent with findings from longitudinal cohort studies by Macias et al. (22) and Soriano et al. (23), which demonstrated a decrease in respiratory illness burden as children grow older and indicated that the decline in symptoms, such as vomiting and fever, as children transition from infancy to toddlerhood, suggests a decreasing susceptibility to common viral infections. Dry cough in infants and toddlers may indicate various underlying conditions, including respiratory infections, asthma, or environmental irritants. Studies by Divarathna et al. (24) and Kwiyolecha et al. (25) have highlighted the prevalence of dry cough in young children and its association with viral respiratory infections. Recurrent chest infections in infants are concerning due to their potential impact on long-term respiratory health and development. Longitudinal studies by Bush (26) and Kyvsgaard et al. (27) have demonstrated the adverse respiratory outcomes associated with early-life respiratory infections, including increased risk of asthma and reduced lung function in later childhood and adulthood. The study indicated that most children with LRTIs stayed in the hospital for 1-3 days, regardless of age group, with slightly higher percentages observed in older children aged 37-48 months. This finding suggested a common trend of short hospital stays for pediatric LRTIs, which is consistent with current guidelines emphasizing early discharge and outpatient management for uncomplicated respiratory infections in children (28). Studies by Biagi et al. (29) and King et al. (30) have highlighted the increasing use of observation units and short-stay protocols for managing pediatric LRTIs, enabling timely evaluation, treatment, and discharge of patients with mild to moderate illness severity.
Infants (0-12 months) are highly vulnerable to lower respiratory tract infections (LRTI), with males and urban children being more prone. Maternal education doesn't significantly affect illness duration, but type of feeding does. Steroid use history significantly prolongs illness duration. Common symptoms usually last 7-8 days, and most children are hospitalized for 1-3 days. Healthcare providers should prioritize early detection and intervention, promote breastfeeding, increase awareness, monitor steroid use, support urban families, conduct further research, and improve healthcare access in rural areas to reduce LRTI duration
