
+91 6002993949
submission@iarconsortium.org
Open Access
ISSN (Print) : 2788-9475
ISSN (Online) : 2788-9483
Background and Objectives: Each year, various Indian states are facing the challenge of vector-borne diseases, which inflict a significant economic and healthcare challenge on the country's population. The epidemiology of malaria and dengue in India in the year 2015-2021 was studied. Methods: The burden of malaria and dengue was analyzed by estimates obtained from different government agencies’ databases, statistical data websites, media reports, and research publications in the years. Results: Total malaria cases reported in India in the years 2015-2021 were 1,864,032 and 729,450 dengue cases were reported in India during this period. This is contrary to various claims about a reduction in malaria cases. States like Odisha have made significant progress to curb malaria cases, whereas Chhattisgarh has undertaken commendable initiatives to control the menace. However, in 2020 the public healthcare scenario was totally diverted to Covid-19 pandemic management and not enough attention was given to other diseases, in terms of diagnosis and treatment. This results in a reduced number of cases of malaria and dengue fever across the country, which was incorrect. Thus, by July of 2021, there was a sharp rise in the number of dengue cases, as Maharashtra state reported 3,356 dengue cases. Interpretation and Conclusion: Findings indicate the geographical variation of vector-borne diseases which are associated with increased population density, unplanned urbanization and various government policy interventions. Overall, this study unravels the high prevalence of vector-borne diseases in India.
Malaria and Dengue are some of the most life-threatening vector-borne diseases (VBDs). They are known for quickly proliferating mosquito saliva originating diseases are posing worldwide public health concerns. Mortality and morbidity resulting from vector-borne diseases have reached alarmingly high i.e. 17% levels1. Malaria is one of the deadliest diseases in this category, causing an estimated 627,000 deaths in 2012. However, with a 30-fold increase in disease incidence over the last fifty years, dengue is the world's fastest-growing disease in this category [1]. Due to a complex set of demographic, environmental and social factors, vector-borne diseases are spreading at an alarming rate. The impact of factors such as increased globalization, travel, trade, unorganized urbanization and alarmingly growing climate change are contributing to disease transmission. Besides, cases of other group members like Chikungunya, Japanese encephalitis, West Nile and Zika virus show their notable presence [1].
Malaria is caused by protozoan parasites, like Plasmodium spp., believed to be delivered by the Anopheles spp. P. falciparum, P. malariae, P. ovale and P. vivax are some of the major Plasmodium strains infecting humans [2]. These parasites colonize and multiply initially in liver cells and later on in the red blood cells. However, clinically malaria is detectable during the erythrocyte cycle. Parasites reproduce sexually in mosquitoes guts, once the gametocytes are consumed by the female Anopheles mosquito during the blood-feeding. The formation of oocyst and sporocyst takes place by the fusion of gametocytes. The sporozoite forms of parasites appear after 10-18 days of incubation in mosquito salivary glands [2]. During blood feeding, sporozoites pass the infection to another host, and the cycle starts again. Malaria exerts massive healthcare and socio-economic impact on mankind. The countrywide prevalence of malaria infection is complex due to diverse geo-climatic conditions. The API (Annual Parasite Index) is a malariometric index that shows malaria incidence per thousand people [3]. In the majority of states, the API index score was <2, whereas the API was 2-5 in some specific regions while >5 in the states of Odisha, Jharkhand, Chhattisgarh, Madhya Pradesh, Rajasthan, Gujarat, Karnataka, Goa and in northeastern states. In India, the most contributing malaria infection is from the eastern state of Odisha [3].
Dengue fever is another Aedes aegpti mosquito-borne disease caused due to infection by four different serotypes (serotype 1-4) of single-stranded RNA Dengue virus (DENV) [4]. DENV also transmits through mosquito bites to a previously infected person, then subsequently to the next host during blood-feeding. Thus, DENV has the potential of species cross-over from animals to humans. Initially, DENV passes through salivary glands infects and multiplies in the midgut, then, later on, invades haemocoel and finally accumulates back in salivary glands. This is from DENV getting transmitted to other humans [4]. In recent years, there is a dramatic growth in the incidence of dengue around the world [1]. The vast majority of dengue cases are not that severe or sometimes asymptomatic and easily treatable. Therefore, the actual numbers of dengue cases are under-reported. As with other feverish illnesses, many dengue cases also remain misdiagnosed.
In recent times, India has witnessed a significant reduction in the number of deaths due to dengue fever [1]. This may be because of the epidemiological transition from infectious to chronic diseases also owing to the disease eradication policy undertaken by various government and public healthcare agencies. These findings could be attributed to overall development in housing conditions, town planning, such as improved sanitation, increased affordability and access to medicines. Even though there is a decline in cases, still Dengue fever has been a matter of concern and challenge to the nation [5]. The overall prevalence of dengue infection based on testing was 38.3% [5]. Integrated disease surveillance programs point to the fact that many areas in the country are encountering frequent seasonal outbreaks. Therefore, it makes important to study the epidemiology of malaria and dengue in the country from 2015 to 2021. For this purpose data from the Government of India’s National Vector Borne Disease Control Program (NVBDCP) [3,6] served as an important source. However, issues like no notification (cases being treated at small clinics), inadequate case reporting and secondary hospital data are the limitations of the source of surveillance data. Also in such data proper mosquito genus and pathogen’s strain level details may not have been carried out.
The data was collated from National Vector Borne Disease Control Programme webpage [6], various other sources (as indicated) and these numbers were used to draw the heat maps. In order to calculate state wise disease burden, number of cases were divided by particular state’s total population based on data given on the Indian population census [36] (https://www.indiacensus.net/density.php). The graph was plotted using Microsoft Excel tools.
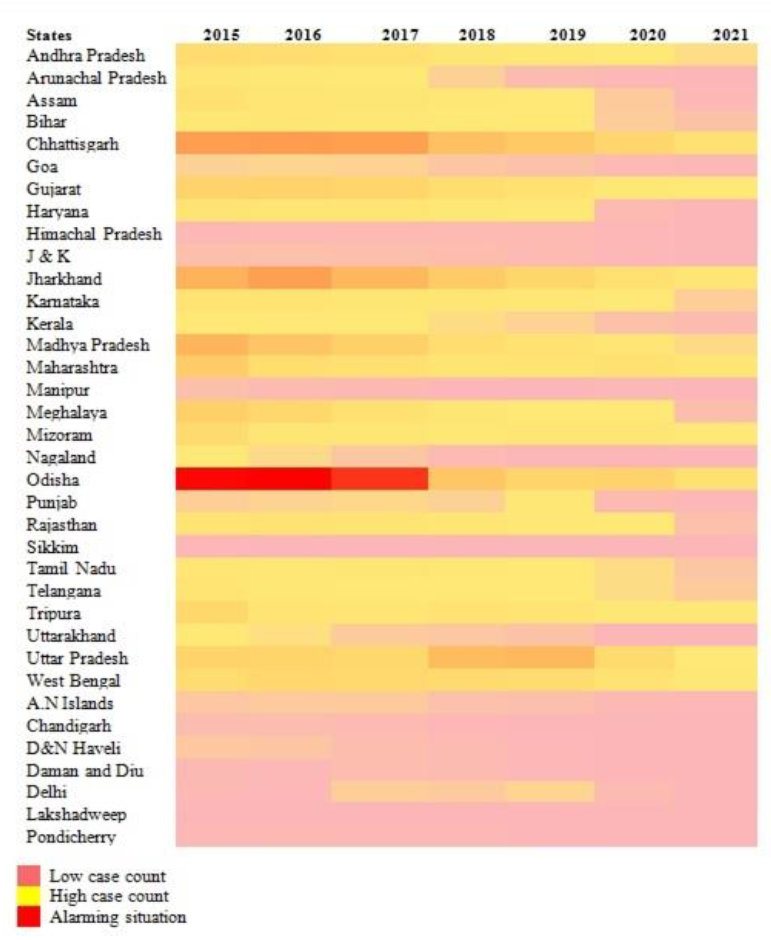
Figure 1: Heat-Map State-Wise Trends of Malaria Infection in India from the Year 2015-2021
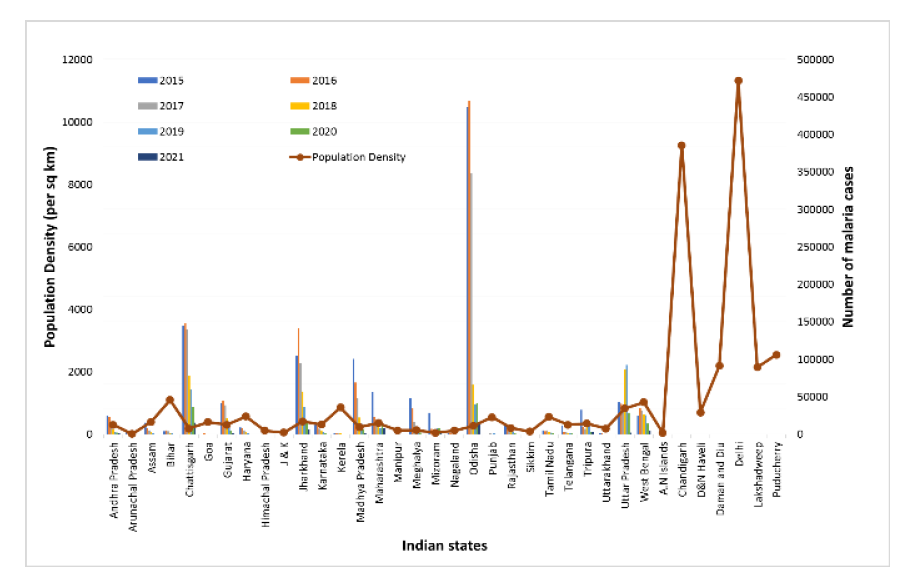
Figure 2: State Population Density vs. Malaria Infections in India from the Year 2015-2021
State-wise Prevalence of Malaria in India
India is one of the high endemic countries to report a decline of 17.6% in the year 2019 in malaria cases as compared to the year 2018 [7]. The diseases prevalence trend throughout the country is moderate to low. However, high infection numbers were seen in north-eastern parts of the country and many parts of Odisha, Chhattisgarh, Madhya Pradesh and Jharkhand (Figure 1-2). Odisha is one of the most affected states by malaria infection and the strains that are mainly responsible for the high number of cases in the state i.e. P. vivax and P. falciparum (Figure 1-2) [8].
In the 1950s there were an estimated 75 million cases and approximately 0.8 million deaths per year [1]. Globally, there is a decline in the cases of malaria cases. This might be attributed to a set of factors that are linked to socio-economic development and initiatives undertaken by national malaria control programs [1]. Even though there is a decline in the total number of cases of malaria infection and a reduced death rate, it is still a matter of concern for the nation [9]. It is our duty to take action to control future malaria outbreaks. Malaria control in Madhya Pradesh is a bit complex because of dense forests with tribal settlements in the region [10]. Over millions of people of various ethnic origins that accounts for 8% of the total community of the country, contributed 30% of total malaria infection, 60% of total P. falciparum cases and 50% of malaria deaths in India [7]. However, the main challenge is to improve these services. During the past decade, in India sibling species of the dominant mosquito vector taxa, like An. culicifacies and An. fluviatilis which account for nearly 80% of malaria cases [11]. Although, despite the accessibility of effective intervention tools for the elimination and control of malaria infection, P. falciparum malaria infection cases remain unstoppable and there is no such decline seen in the death rate [10]. A reduction in the prevalence of malaria cases was also seen in the year-on-year tally. The number of cases and fatalities have declined significantly by 21.27% and 20%, respectively in the year 2019 (338,494 cases, 77 deaths) as compared to 2018 (429,928 cases, 96 deaths) [1].
Trends of Malaria Infection in India from 2015-2021
In the year 2015, a total of 1,169,261 cases of malaria infection were recorded in the country and around 384 deaths were reported throughout the country [12]. The highest numbers of cases were reported from Odisha taking the toll to 436,850 (Figure 1-2). The number of cases in Chhattisgarh mounted to 144,886 cases [6]. The Union territory that reported the least number of cases is Lakshadweep reporting four cases with no casualties [13]. Malaria eradication efforts began in the country in the year 2015 and increased after the launch of the National Framework for Malaria Elimination (NFME) in the year 2016.
Looking at the year 2016, the total malaria cases reported in India are 1087,285 with 331 deaths in total (Figure 1-2). This year also Orissa reported the highest number of cases taking the count to 444,843 and the highest number of deaths seventy-seven in the state and thus remains the worst-hit state. Himachal Pradesh reported cases as low as 106 with no deaths in the state followed by Manipur with only 122 cases with no casualties in the state. India is co-endemic for P. vivax malaria and P. falciparum and they both have biological characteristics that hinder malaria eradication efforts14. In the year 2016, 698 million i.e. over half of the country’s population was at risk. India was among the major contributor i.e. 6% of malaria cases and about an equal number of deaths in the world [14]. In addition to this, the country had a burden of 51% of the global P. vivax cases. In alarming revelations, India had 1.31 million and 23,990 casualties. Dramatically, a 24% decrease in malaria cases was reported in 2016 - 2017.
In the year 2017, the total numbers of reported malaria cases in India are 844,558 with 194 total deaths in the country (Figure 1-2). Sikkim reported the least number of cases this year and the number is twelve with zero deaths. Many other states like Punjab, Rajasthan, Uttar Pradesh, Tamil Nadu, Tripura, Telangana, Uttarakhand also reported no casualties this year. Odisha is the most affected state reporting 352,140 cases and twenty-five deaths (Figure 1-2). Chhattisgarh has seen a sudden spike in malaria cases taking the toll of 140,727 with eighty-one deaths in the state. In the state of Odisha, a mixed Plasmodium species infection has been observed, especially P. ovale and P. malariae (Figure 1-2). Many PCR positive cases show that forty-two cases (38.2%) had P. falciparum infection, 10 (9.1%) had P. malariae and thirty-five cases (31.8%) had P. vivax single infections, whereas, twenty-three (20.9%) had mixed infections[15]. A project with the name Durgama Anchalare Malaria Nirakaran (DAMaN) was started in 2017 by the state of Chhattisgarh[16], targeting the locally identified high endemic places in twenty-three districts. DAMaN comprises mass screening of people and giving them the right treatment, equipping them of the long-lasting insecticidal net and behavioral changes.
There was a decline of 28% in the total malaria cases in 2018 when compared to the year 2017 [1]. In 2018, 429,928 malaria cases and ninety-six deaths were reported. The eastern state of Odisha, which had the highest malaria burden, reported a reduction in cases by over 80% during the same time period1. Odisha’s innovative malaria control measures could serve as a success model for other disease prevalent states. This year Uttar Pradesh reported maximum cases taking the number to 86,486 with no casualties though (Figure 1-2). Chhattisgarh reported 78,717 total cases and thirty-nine deaths in 2018. Whereas, the third-highest number of cases were reported in Odisha 66,311 with three deaths. Interestingly, there was a decline in the transmission with a 50% fall of cases in 2018 [1]. A 48% decrease was also seen in the P. falciparum infections in India this year. Yet a malaria infection burden of close to half a million infections was reported in 2018, which was the reason for concern [17].
India was among the country to record a decline of 17.6% in malaria infection cases [18]. India reported a decline in malaria-related deaths. In 2019 however, the number of cases reduced to around 338.5 thousand in India (Figure 1-2). Thus, the number of cases and casualties has dropped by 21.27% and 20% respectively [19]. With 92,732 cases, Uttar Pradesh reported the highest number of cases. The second-highest number of cases was reported in the state of Chhattisgarh taking the count of the state to 60,458. Jharkhand state reported 37,133 cases (Figure 1-2). This suggests the notable burden of infections despite good disease management reports.
In 2020, India has been able to accomplish a noticeable success in reducing the malaria burden in terms of the total cases of infection by 84.5% and the fatality rate by 83.6% [20]. Total 116 districts in India reported zero malaria cases in the year 2020. Odisha still remains the state to report a maximum number of cases i.e. 41,739 and Chhattisgarh in the second position reporting 36,667 cases (Figure 1-2). Sikkim is one of the states to report as low as four cases and Chandigarh reported seven cases. Looking at the year2021, WHO India has highly supported the high burden to high impact approaches to the states like Madhya Pradesh, West Bengal, Chhattisgarh and Jharkhand. The National Strategic Plan for Malaria Elimination (2017-2022) by India has led to a fast scale-up in the process of quality diagnosis and treatment among the vulnerable population in the dense remote areas of the country [21]. The highest number of cases reported in the country was from the state of Chhattisgarh taking the toll to 15,719 which when compared to other years is substantially low. Odisha reported 15,040 cases which show a gradual decline in the malaria infections in the state. Nagaland, Sikkim, Chandigarh, Arunachal Pradesh, Himachal Pradesh reported less than ten cases, whereas Uttarakhand reported zero [21].
Trends of Dengue Infection in India from 2015-2021
In 2015, a total of 99,913 instances were reported and attended to by various states and union territories, resulting in roughly 220 deaths (Figure 1-2). This year, the infection was evenly dispersed across the country, with the exception of northeastern states such as Sikkim, Meghalaya, and Nagaland, which saw extremely few or no cases on average. The number of cases in Delhi has increased to 15,867, with sixty deaths, the greatest mortality rate in the last 20 years, thus it was one of the most serious disease outbreaks in Delhi since 1996 (Figure 1-2).
In the year 2015, Delhi had been hit by the disease's most severe forms i.e. serotype 2 and 4, which are considered to be powerful strains of the virus emerged as the dominant strains [21]. Serotype-4 is the most dangerous strain, causing fever and shock syndrome. Dengue haemorrhagic fever type 2 is the most common cause worldwide. Similarly to Delhi, Punjab also saw a massive dengue fever outbreak, with about 14,128 cases reported in just a few days and eighteen people dying as a result of the infection (Figure 1-2). Such a massive outbreak has set a strain on patients handling facilities in hospitals to cope with dengue fever and patients. Haryana (9,921), West Bengal (8,516), Gujarat (5,590), Karnataka (5,077), Tamil Nadu (4,535), and Kerala (4,535) are the next most populous states (4,075) (Figure 1-2). Kerala had the second-highest number of casualties in the country, with twenty-five. As a result, if we follow the trend above, we can safely assume that the dengue virus wreaked havoc throughout the country's northern, southern, and western regions (Figure 1-2).
The number of dengue cases in India increased gradually in 2016. In all, 129,166 people died in the country, with 245 fatalities (Figure 1-2). This devastating illness claimed the lives of more than forty-five people. West Bengal was dealing with a dengue fever outbreak that had reached epidemic proportions in 2016. Civic indifference, administrative inefficiency, a lack of readiness, and half-hearted initiatives by the state government could all be factors [23]. With over 15,000 cases and nearly forty-two deaths, Uttar Pradesh became the second-worst affected state from the infection this year. Dengue fever incidences have increased unexpectedly in some northeastern states [24]. The dengue strain revealed that serotype-3 of dengue virus was circulating in the Northern part of the country during this period [25]. The reason behind this might be socio-economic developments such as rapid unplanned urbanization, population movement, poor vector-control measures, and improper waste management practices. Assam recorded 6,157, which is the highest among the ten states [24].
Dengue fever cases had increased dramatically in 2017 [24]. In 2016 there were 16,870 dengue cases registered, but in 2017 there were 28,702, which represents over a 1.7-fold rise in cases (Figure 3-4). India Dengue fever cases were reported to be at an all-time high of 188,401, with a 325% death rate. The southern and north-eastern states saw the greatest increase in instances. In comparison to the previous two years, Sikkim, Nagaland, Mizoram, and Tripura have had the most percentage increases [24]. In the year 2017, the southern states bore the brunt of population growth and increased urbanization, as Tamil Nadu had the most dengue cases with 22,197 (Figure 3-4). A total of 52 persons died as a result of the infection. In this outbreak, for the first time, DENV-4 was identified as the prevalent serotype during an outbreak in Tamil Nadu, with a mixed Th1/Th17 cytokine production profile associated with illness severity [26]. During the warmer months, the mating cycle and maturity of Aedes mosquito vectors is usually accelerated, and thus the incubation period of the dengue virus is shortened. In 2016 also Tiruvallur, in Tamil Nadu was known for having the most dengue epidemics (Figure 3-4). In Kerala, thirty-seven people have died and 19,776 cases of infection (Figure 3-4). In 2017, in Delhi, 9,169 cases were reported, with four deaths (Figure 3-4). While the illness remains a major source of concern, officials claim that because of the large geographical scope, population density, and improved diagnostic tools, the infection is less of a threat, and the number of cases reported, the infection figures are staggering.
In 2018, a modest drop in the number of cases was reported, disrupting the increasing trend of instances (Figure 3-4). A total of 101,192 cases were reported, with 172 people dying as a result of the illness. According to the data from the last few years, Punjab has the highest rate of dengue infections, with 14,980 people diagnosed positive for the disease and nine deaths (Figure 3-4). However, in comparison to 2017, these data were lower in number. The peak point of the dengue breeding season is usually in the first half of November. According to health officials at the time, 500 confirmed cases were recorded every day on average. After mid-November, when the night temperature consistently remained below 15 °C, the cases began to decline. Maharashtra has approximately 11,000 cases, making it the second most impacted state in the country (Figure 3-4). The country as a whole saw a decrease in cases, whereas Maharashtra saw the opposite. Regional diversity was observed with regard to the dominant circulating serotypes. However, DENV-2 was found to be a prevalent serotype across the country [27].
In 2017, 7,829 cases were reported, but in 2018, 11,011 persons were diagnosed, a 1.5-fold increase over the previous year. The death rate, which was twenty-one in 2017 and forty-four in 2018, had also doubled (Figure 3-4). The biggest number of deaths was serotype recorded in the Mumbai and Kolhapur regions of Maharashtra, with twelve and fourteen deaths, respectively. Nearly 68% of the instances this year were reported in metropolitan areas, according to state entomologists [28]. Poor solid waste management, such as garbage and tin cans discarded on the highways, is part of the problem. Water collects in them, making them great breeding grounds for mosquitoes. The increase in infections was attributed by an infectious disease specialist to better reporting and surveillance in the state last year. People were also coming forward earlier to seek treatment, which explains why the state was seeing an increase in instances. In 2018, dengue fever has been diagnosed in people of all ages. Kolhapur reported an unexpectedly high number of cases due to a severe lack of staff in the Kolhapur municipal corporation to locate breeding areas and conduct anti-larval actions [28]. In the year 2018, Delhi, Rajasthan, and Gujarat were among the top five worst-affected states.
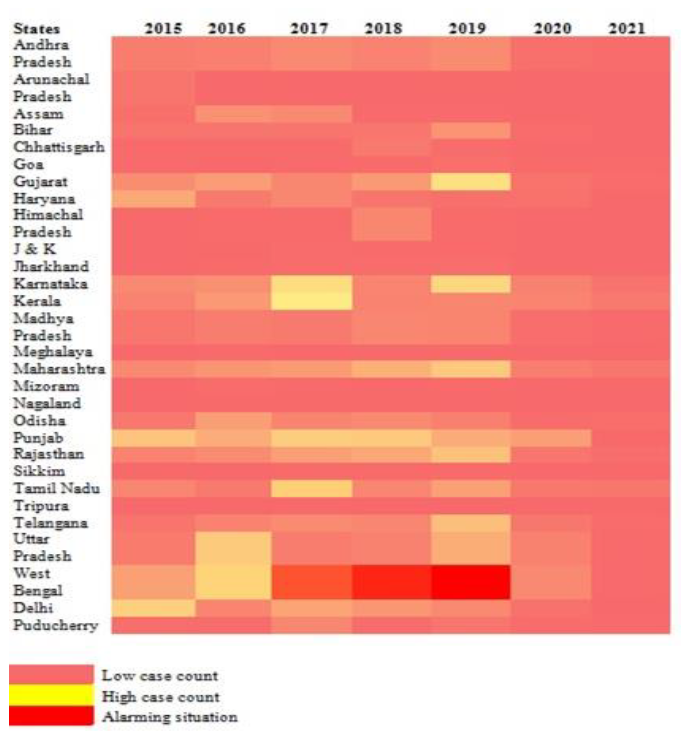
Figure 3: State-wise Trends of Dengue Infection in India from the Year 2015-2021
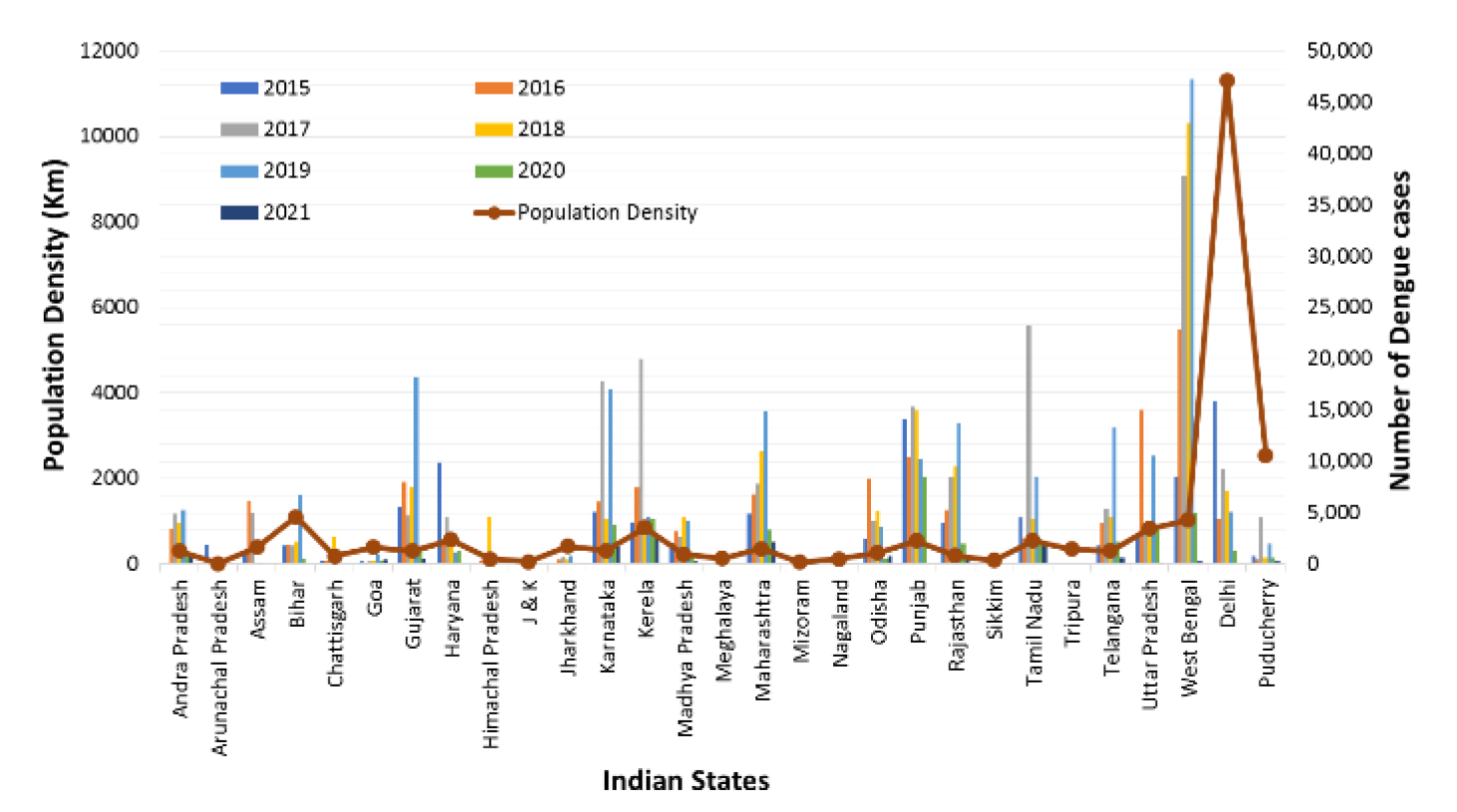
Figure 4: State Population Density vs. Dengue Infections in India from the Year 2015-2021
In the year 2019, there is resurgence in cases of dengue [6]. This sickness infected around 157,315 people, with 166 persons succumbing to the virus. This was about a 14.2 fold rise in the number of incidents, over the previous year. Unfortunately, the monsoon had brought a catastrophic wave of dengue fever in Karnataka this year, as it has in past years, far-reaching over the state and killing hundreds while sickening tens of thousands [29]. Karnataka came in second this year after consistently reporting the third-highest number of dengue cases in the country. Gujarat leads the list of total dengue cases with 16,565, followed by Karnataka with 15,929 cases reported from January to the first week of December this year [30]. Various ecological factors influence the propagation of dengue fever. Unplanned development activities, inappropriate water storage, and improper solid waste management could all contribute to the rise in dengue incidence [4]. However, several climatic factors could contribute to the rise in infections. Dengue fever was once connected with the monsoon season, but it is now prevalent throughout the year. Therefore, mosquitoes - tiny insects, have been a major source of concern for residents, particularly in Bengaluru, the state capital, which has the highest number of dengue-positive cases in Karnataka [4]. Thus, India encountered the risk of deteriorating public health conditions of dengue in the country in 2020, because of inadequate public healthcare resources and the essential focus on COVID-19 [31]. To make matters worse, same year Chikungunya cases have been on the rise [32].
However, in 2020 the public healthcare scenario was totally diverted to Covid-19 pandemic management and enough attention was not given to other diseases, in terms of diagnosis and treatment. This is reflected in dengue fever cases decreasing significantly in 2020, with a total of 39,419 persons infected across the country (Figure 3-4). Punjab, with 8,527 cases and twenty-two deaths, had the highest number of cases. With 3,356 instances, Maharashtra is the second most impacted state. When compared to 2019, Maharashtra, on the other hand, experienced a significant drop of 84% (Figure 3-4). In some circumstances, two possible sources may have led to the decrease. One was considerable variance in the reported data of dengue cases, and the other was a lesser transmission of the vector due to lockdowns across the country, restrictions on construction activity and other economic activities.
In 2021, from January to November end, across India, alarmingly high 1,36,422 cases were reported for dengue and 132 deaths were also reported6. Reasons, behind this outbreak, may be heavy rainfalls, flooding, deposition of stagnant water served as a good breeding ground for mosquitoes. These were the highest numbers since 2016 [33]. 1,378 dengue cases were reported in Maharashtra [6]. The state of Uttar Pradesh is the most severely afflicted by dengue fever. In Uttar Pradesh, the increase in dengue incidence was primarily noticed among youngsters. Dengue virus serotype-2, according to the Indian Council of Medical Research report, was the cause of the disease's rapid spread [34]. With over 1530 dengue cases so far this year, and that to 1200 cases alone in October month, this is perhaps the highest count in the last four years [35]. Since January, Mumbai has reported 305 instances of dengue fever, although no deaths have been reported. Madhya Pradesh and Haryana were also among the worst-affected states. In the light of Covid-19, nationwide mandatory and effective case reporting countrywide scale can help to access reliable assessment of disease menace. Furthermore, it is important to take initiative towards disease outbreak predictive measures for better planning and outbreak management steps. An account also needs to be maintained in case of co-infections situations. That will also help in taking adequate preventive measures [29].
Community health workers can play a crucial role in spreading awareness in the general public, particularly in high-risk areas about prevention measures, mosquito breeding control strategies, proper waste management and hygiene practices. It should be conveyed that disease prevention is the best tactic than treatment, and it is not only public administration and health authorities’ responsibility. Dealing this way can help to handle infectious disease outbreaks. It is also important to extend and replicate the successful disease prevention models nationwide.
Despite claims of the situation in control and appreciation of progress in disease management, the current epidemiological scenario of vector-borne disease outbreaks was fragile in most of the parts of the Country. Therefore, pathogens are sitting at the doors and can cause potential harm to public healthcare. Furthermore, disease prevention and control is not the sole responsibility of the government and public healthcare authorities. The public and society should also play an important role to prevent this catastrophe. India and states need multidisciplinary healthcare approaches integrating several societal realms. Maximum emphasis should focus on vector control and their breeding prevention, disease surveillance, early and reliable diagnosis, population’s training and education. That’s the only way to reduce the burden of infectious disease outbreaks in India.
Acknowledgements
The authors are thankful to Dr J. K. Pal, Dr. Neelu Nawani and Dr Minal Wani for their encouragement and support.
Conflict of interest
None
World Health Organization. “Vector-Borne Diseases.” WHO Fact Sheets, 2020, www.who.int/news-room/fact-sheets/detail/vector-borne-diseases.
Tuteja, Renu. “Malaria — an overview.” FEBS Journal, vol. 274, no. 18, 2007, pp. 4670–4679. https://doi.org/ 10.1111/j.174 2-4658.2007.05997.x
Kumar, Anil, et al. “Burden of malaria in India: retrospective and prospective view.” American Journal of Tropical Medicine and Hygiene, vol. 77, no. 6, 2007, pp. 69–78.
Mutheneni, Srinivas R., et al. “Dengue burden in India: recent trends and importance of climatic parameters.” Emerging Microbes & Infections, vol. 6, 2017, e70. https://doi.org/10.1038/emi.2017.57
Ganeshkumar, P., et al. “Dengue infection in India: a systematic review and meta-analysis.” PLoS Neglected Tropical Diseases, vol. 12, no. 7, 2018, e0006618. https://doi.org/10.1371/journal.pntd.0006618
National Vector Borne Disease Control Programme. NVBDCP, Government of India, nvbdcp.gov.in/index4.php? lang=1&level=0&linkid=431&lid=3715.
World Health Organization. World Malaria Report 2020: 20 Years of Global Progress and Challenges. WHO, 2020.
Dash, A.P., et al. “Malaria in India: challenges and opportunities.” Journal of Biosciences, vol. 33, no. 4, 2008, pp. 583–592. https://doi.org/10.1007/s12038-008-0076-x
Shretta, Rima, et al. “Malaria elimination and eradication.” Major Infectious Diseases, 3rd ed., World Bank, 2017, Chapter 12. https://doi.org/10.1596/978-1-4648-0524-0_ch12
Singh, V., et al. “Why is it important to study malaria epidemiology in India?” Trends in Parasitology, vol. 25, no. 10, 2009, pp. 452–457. https://doi.org/10.1016/j.p t.2009.06.004
Dev, V., and V.P. Sharma. “The dominant mosquito vectors of human malaria in India.” Anopheles Mosquitoes – New Insights into Malaria Vectors, edited by Sylvie Manguin, IntechOpen, 2013. https://doi.org/10.5772/55215
GBD 2015 Disease and Injury Incidence and Prevalence Collaborators. “Global, regional, and national incidence, prevalence, and years lived with disability for 310 diseases and injuries, 1990–2015.” The Lancet, vol. 388, no. 10053, 2016, pp. 1545–1602. https://doi.org/10.1016/S0140-6736(16)31678-6
GBD 2017 SDG Collaborators. “Measuring progress from 1990 to 2017 and projecting attainment to 2030 of the health-related Sustainable Development Goals.” The Lancet, vol. 392, no. 10159, 2018, pp. 2091–2138. https://doi.org/10.1016/S0140-6736(18)32281-5
Anvikar, A.R., et al. “Epidemiology of Plasmodium vivax malaria in India.” American Journal of Tropical Medicine and Hygiene, vol. 95, no. 6, 2016, pp. 108–120. https://doi.org/10.4269/ajtmh.16-0163
Pati, P., et al. “The prevalence of Plasmodium malariae in Odisha, India.” Tropical Biomedicine, vol. 34, no. 3, 2017, pp. 607–614.
Ompad, D.C., et al. “Effectiveness of malaria camps as part of the DAMaN program in Odisha, India: study protocol for a cluster-assigned quasi-experimental study.” Global Health Action, vol. 14, no. 1, 2021, 1886458. https://doi.org/10.1080/16549716.2021.1886458
Ghosh, S.K., and M. Rahi. “Malaria elimination in India—the way forward.” Journal of Vector Borne Diseases, vol. 56, no. 1, 2019, pp. 32–40. https://doi.org/10.4103/0972-9062.257771
World Health Organization. World Malaria Report 2020: India Continues to Make Impressive Gains in Reduction of Malaria Burden. WHO, 2020.
Dey, S. “India Only High Endemic Country to Report Decline of 17.6% in Malaria Cases in 2019.” Times of India, 2 Dec. 2020.
World Health Organization. “With Large Case Reductions, India Moves Closer to Zero Malaria by 2030.” WHO, 2021.
National Vector Borne Disease Control Programme. Strategic Plan for Malaria Control in India 2012–2017. Ministry of Health & Family Welfare, Government of India, 2017.
Chatterjee, P. “Delhi’s Tryst with Dengue—and Why It Was So Bad.” Indian Express, 28 Sept. 2015.
Talukdar, S. “Dengue Outbreak in Bengal: Mamata Banerjee’s Focus Is on Controlling the Spread of News, Not Virus.” Firstpost, 14 Nov. 2017.
Kumbhakar, D. “Dengue in Assam: A Public Health Challenge.” The Sentinel, 14 Nov. 2018.
Parveen, N., et al. “Circulation of single serotype of dengue virus (DENV-3) in New Delhi, India during 2016: a change in the epidemiological trend.” Journal of Infection and Public Health, vol. 12, no. 1, 2019, pp. 49–56. https://doi.org/10.1016/j.jiph.2018.08.008
Gowri Sankar, S., et al. “Emergence of dengue 4 as dominant serotype during 2017 outbreak in South India and associated cytokine expression profile.” Frontiers in Cellular and Infection Microbiology, vol. 11, 2021. https://doi.org/10.3389/fcimb.2021.681937
Alagarasu, K., et al. “Serotype and genotype diversity of dengue viruses circulating in India.” International Journal of Infectious Diseases, vol. 111, 2021, pp. 242–252. https://doi.org/10.1016/j.ijid.2021.08.045
Down To Earth Staff. “Number of dengue cases in 2017 was the highest in a decade.” Down To Earth, 29 June 2018.
Pratap, A. “Dengue deaths double in Maharashtra.” Hindustan Times, 15 Nov. 2018.
Afshan, Y. “Dengue cases highest in Gujarat and Karnataka.” The Hindu, 15 Dec. 2019.
Phadke, R., et al. “Dengue amidst COVID-19 in India: the mystery of plummeting cases.” Journal of Medical Virology, vol. 93, 2021, pp. 4120–4121.
Translational Research Consortia for Chikungunya Virus in India. “Current status of chikungunya in India.” Frontiers in Microbiology, vol. 12, 2021, 695173. https://doi.org/10 .3389/fmicb.2021.695173
Mishra, A. “Dengue outbreak: 23,128 cases reported in Uttar Pradesh, highest since 2016.” India Today, 10 Nov. 2021.
Times of India Staff. “Newer dengue variant, DENV-2 spotted.” Times of India, 22 Sept. 2021.
Mint Staff. “Delhi logs nearly 1200 dengue cases in Oct, highest for the month in 4 years.” Mint, 2 Nov. 2021.
“Indian census – state population data.” India Census, 2021, www.indiacensus.net/density.php.
