
+91 6002993949
submission@iarconsortium.org
Open Access
ISSN (Print) : 2788-9475
ISSN (Online) : 2788-9483
Background: Iron supplementation is a common recommendation for all pregnant women, regardless of their iron status. However, providing excess iron to non-anemic pregnant women may lead to iron overload, increasing the risk of oxidative stress and inflammation. Aim: The aim of the study was to assess the differential effect of iron supplementation on hematological parameters, oxidative stress, and inflammation in nonanemic and anemic pregnant women. Patients and Methods: A cross-sectional study with longitudinal follow-up was conducted at the Obstetric and Gynecology Unit of Tikrit Teaching Hospital, Tikrit City, from January 1 to December 31, 2024. A total of 80 pregnant women at 12 weeks of gestation were enrolled and categorized into two equal groups: a nonanemic group (hemoglobin >11 g/dL) and an anemic IDA group (hemoglobin <10 g/dL). The nonanemic group received 60 mg elemental iron once daily, while the anemic IDA group received 120 mg/day of elemental iron in addition to standard folic acid and calcium-vitamin D supplementation. Follow-up was conducted until 28 weeks of gestation. Blood samples were collected at 12 and 28 weeks for hematological analysis (hemoglobin and hematocrit) and biochemical markers (serum glucose, ferritin, malondialdehyde [MDA], total antioxidant status [TAS], and high-sensitivity C-reactive protein [hsCRP]). Standardized instruments and validated assays were used for all tests. Results: Before supplementation, anemic pregnant women had significantly lower levels of hemoglobin, RBC count, HCT, MCV, MCH, MCHC, and ferritin, and higher levels of MDA, MDA/TAS ratio, and hsCRP compared to non-anemic women, indicating greater oxidative stress and inflammation. After iron supplementation, non-anemic women showed a significant increase in MDA and MDA/TAS ratio and a slight rise in hsCRP, suggesting increased oxidative stress and inflammation. In contrast, anemic women exhibited an increase in hemoglobin levels, but a decrease in RBC count, HCT, MCV, MCH, MCHC, and ferritin, along with a mild increase in oxidative stress markers (MDA) and inflammation (hsCRP). The percentage change analysis revealed that non-anemic women experienced a more significant increase in oxidative stress markers and hsCRP, while anemic women showed a more significant decrease in TAS following iron supplementation. Conclusion: Iron supplementation may have differential effects on oxidative stress and inflammation in anemic versus non-anemic pregnant women. While it improves anemia, it may exacerbate oxidative stress and inflammation, particularly in non-anemic women. Monitoring biochemical markers, such as MDA, TAS, and hsCRP, is essential to balance the benefits and risks of iron supplementation during pregnancy.
Pregnancy is a dynamic physiological state characterized by profound anatomical, biochemical, and hematological adaptations that support fetal growth and development. Among these changes, alterations in hematological parameters are particularly important, as they reflect both maternal health status and the capacity to meet the metabolic demands of the fetoplacental unit [1.2]. During normal pregnancy, plasma volume increases by approximately 40–50%, while red blood cell mass rises to a lesser extent, resulting in hemodilution and a relative decline in hemoglobin concentration, commonly referred to as physiological anemia of pregnancy [3,4]. These changes are essential for optimizing uteroplacental perfusion and reducing blood viscosity, thereby enhancing oxygen and nutrient delivery to the fetus [5,6]. Despite being a normal adaptation, anemia during pregnancy remains one of the most common medical disorders worldwide and represents a major public health concern, particularly in developing countries [7,8]. Anemia is defined as a reduction in hemoglobin concentration, hematocrit, or red blood cell count below normal reference levels, leading to impaired oxygen transport to tissues [9]. According to the World Health Organization, anemia in pregnancy is diagnosed when hemoglobin levels fall below 11 g/dL, with severity classified into mild, moderate, severe, and very severe categories [10]. However, due to physiological hemodilution, some guidelines recommend trimester-specific thresholds, particularly a lower cutoff of 10.5 g/dL during the second trimester [11,12]. The etiology of anemia in pregnancy is multifactorial and includes nutritional deficiencies, infections, chronic diseases, genetic disorders, and obstetric factors [13,14]. Among these, iron deficiency is the most common cause and accounts for approximately half of all anemia cases globally [15]. Iron is a critical micronutrient involved in hemoglobin synthesis, oxygen transport, cellular respiration, DNA synthesis, and immune function [16,17]. During pregnancy, iron requirements increase substantially due to expansion of maternal red blood cell mass, placental development, fetal growth, and blood loss during delivery [18]. The total iron requirement during pregnancy is estimated to be approximately 1000–1200 mg, with the highest demand occurring in the third trimester [19,20]. Since many women enter pregnancy with inadequate iron stores, they are at high risk of developing iron deficiency anemia, particularly in resource-limited settings [21].
Assessment of iron status during pregnancy relies on a combination of hematological and biochemical parameters. While hemoglobin concentration is commonly used for screening, it does not accurately reflect iron stores [22]. Serum ferritin is considered the most reliable indicator of body iron reserves, whereas transferrin and total iron-binding capacity increase in iron deficiency as part of a compensatory mechanism to enhance iron transport [23,24]. However, interpretation of these markers can be complicated by inflammation, as ferritin is an acute-phase reactant and may be elevated in inflammatory states despite depleted iron stores [25]. Therefore, additional markers such as C-reactive protein are often used to differentiate iron deficiency anemia from anemia of chronic disease [26]. In addition to hematological alterations, pregnancy is associated with significant changes in oxidative stress and inflammatory responses. Oxidative stress occurs when there is an imbalance between the production of reactive oxygen species and the capacity of antioxidant defense systems to neutralize them [27]. The placenta is a major source of reactive oxygen species, especially after the first trimester when oxygen tension increases, leading to enhanced mitochondrial activity and oxidative metabolism [28]. Under normal conditions, antioxidant systems including enzymatic components such as superoxide dismutase, catalase, and glutathione peroxidase, as well as non-enzymatic antioxidants like vitamins C and E, help maintain redox balance [29]. However, excessive oxidative stress can lead to lipid peroxidation, protein damage, DNA mutations, and impaired placental function, contributing to adverse pregnancy outcomes [30].
Inflammation also plays a central role in pregnancy and is closely linked to both anemia and oxidative stress. C-reactive protein, a sensitive biomarker of systemic inflammation, is commonly elevated in pregnancy due to physiological and pathological processes [26,27]. Elevated levels of inflammatory markers have been associated with adverse maternal and fetal outcomes, including preeclampsia, preterm birth, and intrauterine growth restriction [28,29]. Furthermore, inflammation can disrupt iron metabolism by increasing hepcidin levels, reducing intestinal iron absorption, and limiting iron availability for erythropoiesis, thereby exacerbating anemia [30]. Given the complex interplay between iron metabolism, hematological parameters, oxidative stress, and inflammation during pregnancy, understanding the response to iron supplementation is of critical importance. Differences in baseline iron status may influence therapeutic outcomes, particularly between anemic and nonanemic pregnant women. Therefore, this study aims to evaluate the differential effects of iron supplementation on hematological parameters, oxidative stress, and inflammatory markers in these two groups, with the goal of improving maternal health and pregnancy outcomes.
tients and Methods
This cross-sectional study with longitudinal follow-up was conducted at the Obstetrics and Gynecology Unit of Tikrit Teaching Hospital, Tikrit City, from January 1st to the end of December 2024. A total of 80 pregnant women at 12 weeks of gestation (end of the first trimester) were recruited from the Obstetrics Outpatient Department. Participants were divided into two groups according to their hemoglobin levels: a nonanemic group consisting of 40 pregnant women with hemoglobin levels >11 g/dL, and an anemic iron deficiency anemia (IDA) group consisting of 40 pregnant women with hemoglobin levels <10 g/dL.
After obtaining written informed consent, demographic data including age and parity were recorded. Anthropometric measurements were performed, where height was measured using a portable stadiometer and weight was measured using a digital weighing scale. Body mass index (BMI) was calculated as weight in kilograms divided by the square of height in meters (kg/m²).
Pregnant women were excluded if they had multiple pregnancies, gestational diabetes mellitus, pregnancy-induced hypertension, thyroid disorders, hemoglobin levels between 10 and 11 g/dL, or a history of blood transfusion. Participants in the nonanemic group received ferrous sulfate (200 mg containing 60 mg elemental iron) once daily, folic acid at a standard preventive dose of 400–600 µg once daily, and a Vitcal tablet containing calcium carbonate (625 mg) and vitamin D₃ (125 IU) once daily. Participants in the anemic (IDA) group received ferrous sulfate (200 mg containing 60 mg elemental iron) twice daily (total 120 mg/day), folic acid (5 mg) once daily, and the same Vitcal supplementation regimen. Compliance with supplementation and any reported side effects were monitored during follow-up visits. All participants were followed from 12 weeks until 28 weeks of gestation.
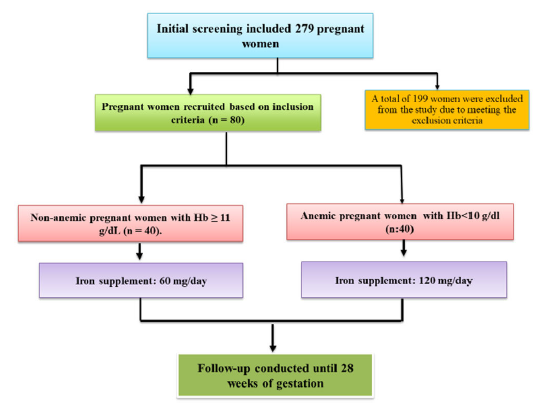
Figure 1: Flowchart of the study protocol
Data Collection and Laboratory Analysis
A total of five milliliters of venous blood was collected from each participant under fasting conditions at two time points: 12 weeks and 28 weeks of gestation. Of this, 2 mL was transferred into ethylenediaminetetraacetic acid (EDTA)-containing tubes for hematological analysis. The measured hematological parameters included hemoglobin concentration, hematocrit, red blood cell (RBC) count, mean corpuscular volume (MCV), mean corpuscular hemoglobin (MCH), and mean corpuscular hemoglobin concentration (MCHC). These parameters were analyzed using an automated hematology analyzer (Sysmex XS-1000i). The remaining 3 mL of blood was centrifuged at 3000 rpm for 15 minutes to separate the serum. The obtained serum samples were stored at −40°C until further biochemical analysis. Serum glucose levels were determined using the glucose oxidase–peroxidase endpoint colorimetric method with an Accent autoanalyzer (Poland). Serum malondialdehyde (MDA), serum ferritin, and high-sensitivity C-reactive protein (hsCRP) levels were measured using enzyme-linked immunosorbent assay (ELISA) kits (Sunlong Co., China). Total antioxidant status (TAS) was assessed using the ferric reducing ability of plasma (FRAP) assay, with absorbance measured at 593 nm.
Patient Follow-Up and Laboratory Testing Protocol
Each participant attended two visits during the study period. The first visit was conducted at 12 weeks of gestation (baseline), during which blood samples were collected and baseline hematological and biochemical parameters were assessed. The second visit was conducted at 28 weeks of gestation, during which the same procedures and laboratory tests were repeated. This allowed for evaluation of changes in hematological indices, oxidative stress markers, and inflammatory parameters following iron supplementation.
Statistical Analysis
Statistical analysis was performed using the Statistical Package for the Social Sciences (SPSS), version 26.0. Data distribution was assessed using the Kolmogorov–Smirnov test. Normally distributed data were presented as mean±standard deviation (SD), while non-normally distributed data were expressed as median and interquartile range. Comparisons between groups were performed using the independent Student’s t-test for continuous variables, whereas the Mann–Whitney U test was used for non-normally distributed variables such as hsCRP. Within-group comparisons before and after iron supplementation were conducted using paired t-tests for normally distributed data and Wilcoxon’s signed-rank test for non-parametric data. A p-value of less than 0.05 was considered statistically significant.
Table 1 presents a comparison of various characteristics between non-anemic and anemic IDA groups of pregnant women, each consisting of 40 participants. The variables analyzed include age, height, weight, BMI, gestational age at recruitment, and gestational age at follow-up. The mean age was slightly higher in the non-anemic group (26.34±4.20 years) compared to the anemic IDA group (25.67±3.90 years), but this difference was not statistically significant (P=0.713). Similarly, other variables such as gravidity, height, weight, BMI, gestational age at recruitment, and gestational age at follow-up showed no significant differences between the two groups
The anemic IDA group showed significantly lower Hb levels (9.67±1.25 g/dL) compared to the non-anemic group (13.24±0.72 g/dL). RBCs count was also significantly lower in anemic women (3.54±0.65 x10^6/mL) compared to non-anemic women (4.56±0.41 x10^6/mL). Hematocrit (HCT) levels, mean corpuscular volume (MCV), mean corpuscular hemoglobin (MCH), and mean corpuscular hemoglobin concentration (MCHC) were all significantly reduced in the anemic IDA group compared to the non-anemic group. Ferritin levels were markedly lower in anemic women (8.15±4.23 ng/mL) than in non-anemic women (24.70±11.32 ng/mL). MDA was higher in the anemic IDA group (8.32±1.92 mmol/L) compared to the non-anemic group (6.9±1.47 mmol/L), while total antioxidant status was significantly lower in anemic women (300.61±78.43 mmol/L) versus non-anemic women (420.85±168.47 mmol/L) (p=0.001). The MDA/TAS ratio was significantly higher in anemic women (0.029±0.011) compared to non-anemic women (0.019±0.008). High-sensitivity CRP levels were also
Table 1: General and maternal properties of non-anemic and anemic IDA groups of pregnant women significantly elevated in the anemic IDA group (5708.92 ng/mL) compared to the non-anemic group (5032.67 ng/mL).
| Variables | Pregnant women | P-Value | |
Non-anemic group (n:40) | Anemic IDA group (n:40) | ||
Age (years) | 26.34±4.20 | 25.67±3.90 | 0.713 |
Height (cm) | 156.42±3.10 | 157.25±4.10 | 0.642 |
Weight (kg) | 52.18±7.15 | 50.47±6.12 | 0.092 |
BMI (kg/m2) | 21.48±2.83 | 21.09±2.50 | 0.145 |
Gestational age at recruitment (weeks) | 11.98±0.50 | 12.04±0.31 | 0.234 |
Gestational age at follow-up (weeks) | 28.19±0.28 | 28.12±0.26 | 0.927 |
Table 2: Comparison of hematological and biochemical parameters in nonanemic and anemic pregnant women before iron supplementation (at 12 weeks of gestation)
Parameters | Nonanemic Group | Anemic IDA Group | p Value |
Hemoglobin (g/dL) | 13.24±0.72 | 9.67±1.25 | 0.001 |
RBC count (10^6/mL) | 4.56±0.41 | 3.54±0.65 | 0.002 |
HCT (%) | 36.88±2.34 | 27.31±3.02 | 0.001 |
MCV (fL) | 87.12±6.35 | 73.18±10.21 | 0.001 |
MCH (pg) | 30.4±1.95 | 21.5±3.89 | 0.001 |
MCHC (g/dL) | 35.45±2.57 | 28.67±2.11 | 0.001 |
Ferritin (ng/mL) | 24.70±11.32 | 8.15±4.23 | 0.001 |
MDA (mmol/L) | 6.9±1.47 | 8.32±1.92 | 0.001 |
TAS (mmol/L) | 420.85±168.47 | 300.61±78.43 | 0.001 |
MDA/TAS | 0.019±0.008 | 0.029±0.011 | 0.001 |
hsCRP (ng/mL) | 5032.67 | 5708.92 | 0.012 |
Table 3 Hemoglobin levels showed a slight decline from 13.24±0.72 g/dL to 12.17±0.65 g/dL (p = 0.342). Similarly, the red blood cell (RBC) count decreased slightly from 4.56±0.41 x10^6/mL to 4.40±0.40 x10^6/mL (p = 0.711). HCT levels dropped from 36.88±2.34% to 35.52±2.36% (p = 0.122), while MCV decreased marginally from 87.12±6.35 fL to 86.12±6.55 fL (p = 0.089). MCH levels exhibited a non-significant decrease from 30.4±1.95 pg to 28.97±2.15 pg (p = 0.623), and MCHC decreased from 35.45±2.57 g/dL to 34.20±2.15 g/dL (p = 0.054). Ferritin levels remained relatively stable, with a slight change from 24.70±10.02 ng/mL to 24.90±10.12 ng/mL (p = 0.432). However, MDA levels, increased significantly from 6.9±1.47 mmol/L to 10.90±2.78 mmol/L (p = 0.001). TAS significantly declined from 420.85±168.47 mmol/L to 320.48±130.67 mmol/L (p = 0.029). Consequently, the MDA/TAS ratio significantly increased from 0.019±0.008 to 0.035±0.014 (p = 0.001). The hsCRP levels showed a slight increase from 5032.67 ng/mL to 5298.70 ng/mL (p = 0.041),
Table 3: Hematological and biochemical parameters in non-anemic pregnant women before and after iron supplementation
| Parameters | Non-anemic group (n:40) | p Value | |
Before supplementation (at 12th weeks of gestation) | After supplementation (28th week of gestation) | ||
Hemoglobin (g/dL) | 13.24±0.72 | 12.17±0.65 | 0.342 |
RBC count | 4.56±0.41 | 4.40±0.40 | 0.711 |
HCT (%) | 36.88±2.34 | 35.52±2.36 | 0.122 |
MCV (fL) | 87.12±6.35 | 86.12±6.55 | 0.089 |
MCH (pg) | 30.4±1.95 | 28.97±2.15 | 0.623 |
MCHC (g/dL) | 35.45±2.57 | 34.20±2.15 | 0.054 |
Ferritin (ng/mL) | 24.70±10.02 | 24.90±10.12 | 0.432 |
MDA (mmol/L) | 6.9±1.47 | 10.90±2.78 | 0.001 |
TAS (mmol/L) | 420.85±168.47 | 320.48±130.67 | 0.029 |
MDA/TAS | 0.019±0.008 | 0.035±0.014 | 0.001 |
hsCRP (ng/mL) | 5032.67 | 5298.70 | 0.041 |
Hemoglobin levels significantly increased from 8.70±1.20 g/dL to 9.67±1.25 g/dL (p=0.001), indicating an improvement in anemia. However, the RBC count showed a significant decrease from 3.85±0.50 x10^6/mL to 3.54±0.65 x10^6/mL (p=0.015). Hematocrit (HCT) values also decreased significantly from 29.00±2.95% to 27.31±3.02% (p=0.001), and mean corpuscular volume (MCV) decreased from 76.50±12.00 fL to 73.18±10.21 fL (p=0.001). Similarly, mean corpuscular hemoglobin (MCH) decreased from 23.1±4.70 pg to 21.5±3.89 pg (p=0.001), and mean corpuscular hemoglobin concentration (MCHC) decreased from 30.20±2.30 g/dL to 28.67±2.11 g/dL (p=0.001). Ferritin levels significantly decreased from 10.00±4.80 ng/mL to 8.15±4.23 ng/mL (p=0.001), reflecting possible depletion of iron stores. Malondialdehyde (MDA) levels, which indicate oxidative stress, increased slightly from 8.10±1.90 mmol/L to 8.32±1.92 mmol/L (p=0.035). Total antioxidant status (TAS) also decreased significantly from 315.00±86.50 mmol/L to 300.61±78.43 mmol/L (p=0.031), showing reduced antioxidant capacity. The MDA/TAS ratio remained relatively stable, with a slight change from 0.028±0.011 to 0.029±0.011 (p=0.460), suggesting that oxidative stress relative to antioxidant defense did not change significantly. High-sensitivity C-reactive protein (hsCRP) levels slightly increased from 5600.00 ng/mL to 5708.92 ng/mL (p=0.008), indicating a mild increase in inflammatory response following iron supplementation.
Table 4: Hematological and biochemical parameters in anemic pregnant women before and after iron supplementation
| Parameters | Anemic IDA pregnant women (n:40) | p Value | |
Before supplementation | After supplementation | ||
Hemoglobin (g/dL) | 8.70±1.20 | 9.67±1.25 | 0.001 |
RBC count | 3.85±0.50 | 3.54±0.65 | 0.015 |
HCT (%) | 29.00±2.95 | 27.31±3.02 | 0.001 |
MCV (fL) | 76.50±12.00 | 73.18±10.21 | 0.001 |
MCH (pg) | 23.1±4.70 | 21.5±3.89 | 0.001 |
MCHC (g/dL) | 30.20±2.30 | 28.67±2.11 | 0.001 |
Ferritin (ng/mL) | 10.00±4.80 | 8.15±4.23 | 0.001 |
MDA (mmol/L) | 8.10±1.90 | 8.32±1.92 | 0.035 |
TAS (mmol/L) | 315.00±86.50 | 300.61±78.43 | 0.031 |
MDA/TAS | 0.028±0.011 | 0.029±0.011 | 0.460 |
hsCRP (ng/mL) | 5600.00 | 5708.92 | 0.008 |
The study found that the percentage of increase in serum MDA, MDA/TAS, and hsCRP was significantly more among the nonanemic group when compared with anemic pregnant women. For the TAS, there was a statistically significant decrease in nonanemic and an increase in anemic pregnant women following iron supplementation. This comparison is shown in Table 5.
Table 5: Comparison the percentage changes in biochemical parameters between anemic and non-anemic pregnant women after iron supplementation
| Parameters | Percentage Change | |
| Anemic IDA group | Non-Anemic group | |
| MDA (mmol/L) | 57.97 | 2.72 |
TAS (mmol/L) | -23.85 | -4.57 |
MDA/TAS | 84.21 | 3.57 |
Ferritin (ng/mL) | 0.81 | -18.50 |
hsCRP (ng/mL) | 5.29 | 1.95 |
The data presented in Table 3.6 highlights the distribution of anemic pregnant women according to severity, with the majority classified as having moderate anemia (45%), followed by mild anemia (37.5%) and severe anemia (17.5%). Notably, no cases of very severe anemia were reported. The predominance of moderate anemia suggests a significant burden of nutritional deficiencies or other contributing factors, emphasizing the need for effective screening and management strategies during pregnancy. The presence of severe anemia in nearly one-fifth of the cases underscores the importance of targeted interventions to prevent complications. Table 6
Table 6: Distribution of anemic pregnant women according to severity
IDA Anemia Severity | Number of Cases (n = 40) | Percentage |
Mild Anemia | 15 | 37.5% |
Moderate Anemia | 18 | 45% |
Severe Anemia | 7 | 17.5% |
Very Severe Anemia | 0 | 0% |
Elevated hsCRP levels were observed in both the preterm labor group (6305.32±198.3 ng/mL) and abortion group (6100.4±175.2 ng/mL) relative to the healthy pregnancy group (5032.67±134.50 ng/mL), with a significant P-value (0.011), indicating an inflammatory response associated with adverse outcomes. Similarly, MDA levels, a marker of oxidative stress, were significantly higher in complicated pregnancies, while TAS, reflecting antioxidant capacity, was notably lower in these groups (P = 0.001), suggesting impaired antioxidant defenses. The increased MDA/TAS ratio in the preterm labor (0.030±0.010) and abortion groups (0.028±0.009) compared to healthy pregnancies (0.019±0.008) further emphasizes a shift toward oxidative stress dominance (P = 0.01) Table 7.
Table 7: Inflammation markers in relation to clinical complications in pregnant women
Clinical Complication | hsCRP (ng/mL) | MDA (mmol/L) | TAS (mmol/L) | MDA/TAS Ratio |
Preterm Labor | 6305.32±198.3 | 8.75±1.85 | 290.72±75.41 | 0.030±0.010 |
Abortion | 6100.4±175.2 | 8.45±1.70 | 295.18±80.28 | 0.028±0.009 |
Healthy Pregnancy | 5032.67±134.50 | 6.90±1.47 | 420.85±168.47 | 0.019±0.008 |
P-value | 0.011 | 0.017 | 0.001 | 0.01 |
Iron deficiency anemia is more common during pregnancy, particularly in developing countries, and remains associated with increased maternal morbidity, mortality, and adverse pregnancy outcomes [14,15]. Because of this high burden, the World Health Organization recommends routine daily iron supplementation of 30–60 mg elemental iron during pregnancy as part of standard antenatal care [12]. Nevertheless, universal iron supplementation remains a subject of debate, since administration of iron to women who are not iron deficient may increase the risk of oxidative stress and iron excess, with possible unfavorable biological effects [31]. The present study was designed to evaluate the differential effects of iron supplementation on hematological parameters, oxidative stress, and inflammation in nonanemic and anemic pregnant women. Our findings demonstrated that iron supplementation had no significant effect on hematological indices or serum ferritin in nonanemic pregnant women. This finding is in agreement with Falahi et al. [32], who reported that prophylactic iron supplementation in healthy pregnant women did not result in significant improvement in hemoglobin or ferritin levels. In contrast, iron supplementation significantly improved hematological parameters in anemic pregnant women, supporting the established benefit of iron therapy in iron-deficient states [23,25]. Similar observations were reported by Khalid et al. [33], who showed hematologic improvement after oral iron therapy in pregnant women with iron deficiency anemia, and by Rogozińska et al. [34], whose systematic review confirmed the efficacy of iron preparations in reproductive-age women with iron deficiency anemia during pregnancy. Rajendran et al. [35] likewise demonstrated that iron supplementation was beneficial in anemic women but was associated with biochemical evidence of oxidative stress in nonanemic women. Before supplementation, oxidative stress appeared to be higher in anemic pregnant women than in nonanemic women. This is consistent with the general understanding of iron deficiency and its systemic effects on metabolism and redox balance [24,27]. A possible explanation is that iron deficiency itself may impair the function of iron-dependent antioxidant enzymes while simultaneously increasing lipid peroxidation, thereby worsening oxidative imbalance [28,30]. In the present study, iron supplementation increased malondialdehyde levels in both nonanemic and anemic pregnant women, indicating enhanced lipid peroxidation after supplementation. These findings support the concept that ferrous iron, although therapeutically essential in deficiency states, may also act as a pro-oxidant by participating in redox reactions that generate reactive oxygen species [27,30,31]. An important observation in this study was that oxidative stress appeared more pronounced in nonanemic pregnant women despite the administration of only a prophylactic low dose of iron. Although these women received half the dose given to the anemic group, they still showed a significant reduction in total antioxidant status after supplementation. This may reflect iron-induced free radical generation in women who were already relatively iron replete, with subsequent consumption of antioxidant defenses. A possible mechanism is reduced activity of antioxidant enzymes such as superoxide dismutase in the presence of increased reactive oxygen species [27]. On the other hand, total antioxidant status increased significantly in the anemic iron deficiency anemia group after supplementation, suggesting that correction of iron deficiency may restore antioxidant balance once adequate iron becomes available for normal enzyme function. This interpretation is supported by the concept that iron plays a critical role in enzymatic antioxidant systems [24,25]. The inflammatory profile in our study also differed between groups. Before supplementation, C-reactive protein levels were higher in anemic women, which may indicate the coexistence of iron deficiency and low-grade systemic inflammation. This is in line with Asemi et al. [26], who reported associations between inflammatory and oxidative stress markers in pregnant women. After supplementation, C-reactive protein decreased in the anemic group despite a mild rise in oxidative stress markers, a finding that may be explained by improvement in iron status and restoration of antioxidant defenses. In contrast, nonanemic women experienced increased inflammatory activity after supplementation, probably as a consequence of iron-induced oxidative stress and free radical generation. These results suggest that iron supplementation is clearly beneficial when iron deficiency anemia is present, but it may exert deleterious oxidative and inflammatory effects when given to iron-replete women. Although current WHO recommendations continue to support routine daily oral iron supplementation in settings with a high prevalence of anemia [12], emerging evidence suggests that supplementation strategies may need to be individualized to balance benefits and risks [21]. Taken together, the findings of this study indicate that the response to iron supplementation during pregnancy differs substantially according to baseline anemia status. In anemic women, supplementation improved hematological parameters and was associated with a more favorable antioxidant and inflammatory response. In nonanemic women, however, iron supplementation produced little hematological benefit while increasing oxidative stress and inflammatory burden. These findings highlight the importance of a more selective and individualized approach to iron supplementation during pregnancy, particularly in populations where not all women are iron deficient.
World Health Organization. Worldwide Prevalence of Anaemia 1993–2005: WHO Global Database on Anaemia. World Health Organization, 2008.
Cunningham, F. Gary, et al. Williams Obstetrics. 25th ed., McGraw-Hill Education, 2018.
Bain, Barbara J. Blood Cells: A Practical Guide. 5th ed., Wiley-Blackwell, 2015.
Guyton, Arthur C., and John E. Hall. Textbook of Medical Physiology. 14th ed., Elsevier, 2021.
Blackburn, Susan T. Maternal, Fetal, and Neonatal Physiology. 5th ed., Elsevier, 2018.
Weiss, G., and L. T. Goodnough. “Anemia of Chronic Disease.” New England Journal of Medicine, vol. 352, no. 10, 2005, pp. 1011–1023.
Milman, N. “Iron and Pregnancy—A Delicate Balance.” Annals of Hematology, vol. 85, no. 9, 2006, pp. 559–565.
Scholl, Theresa O. “Iron Status during Pregnancy: Setting the Stage for Mother and Infant.” American Journal of Clinical Nutrition, vol. 81, 2005, pp. 1218S–1222S.
Centers for Disease Control and Prevention. Recommendations to Prevent and Control Iron Deficiency in the United States. MMWR, 1998.
Bothwell, T. H. “Iron Requirements in Pregnancy and Strategies to Meet Them.” American Journal of Clinical Nutrition, vol. 72, 2000, pp. 257S–264S.
Allen, Lindsay H. “Anemia and Iron Deficiency: Effects on Pregnancy Outcome.” American Journal of Clinical Nutrition, vol. 71, 2000, pp. 1280S–1284S.
World Health Organization. Iron Deficiency Anaemia: Assessment, Prevention and Control. World Health Organization, 2001.
Pavord, S., et al. “UK Guidelines on the Management of Iron Deficiency in Pregnancy.” British Journal of Haematology, vol. 156, no. 5, 2012, pp. 588–600.
Stevens, G. A., et al. “Global, Regional, and National Trends in Haemoglobin Concentration…” The Lancet Global Health, vol. 1, no. 1, 2013, pp. e16–e25.
Balarajan, Y., et al. “Anaemia in Low-Income and Middle-Income Countries.” The Lancet, vol. 378, no. 9809, 2011, pp. 2123–2135.
Hytten, F. E., and I. Leitch. The Physiology of Human Pregnancy. 2nd ed., Blackwell Scientific Publications, 1971.
Milman, N. “Postpartum Anemia I: Definition, Prevalence, Causes, and Consequences.” Annals of Hematology, vol. 90, no. 11, 2011, pp. 1247–1253.
Hoffbrand, A. V., and P. A. H. Moss. Essential Haematology. 7th ed., Wiley-Blackwell, 2016.
World Health Organization. Global Nutrition Targets 2025: Anaemia Policy Brief. World Health Organization, 2014.
McLean, E., et al. “Worldwide Prevalence of Anaemia…” Public Health Nutrition, vol. 12, no. 4, 2009, pp. 444–454.
Lynch, S. “The Rationale for Iron Supplementation in Pregnancy.” Journal of Nutrition, vol. 130, 2000, pp. 440S–442S.
Daru, J., et al. “Serum Ferritin as an Indicator of Iron Status…” American Journal of Clinical Nutrition, vol. 106, 2017, pp. 1634S–1639S.
Camaschella, Clara. “Iron-Deficiency Anemia.” New England Journal of Medicine, vol. 372, no. 19, 2015, pp. 1832–1843.
Ganz, T., and E. Nemeth. “Iron Homeostasis in Host Defence and Inflammation.” Nature Reviews Immunology, vol. 15, no. 8, 2015, pp. 500–510.
Means, R. T. Jr. “Iron Deficiency and Iron Deficiency Anemia…” Nutrients, vol. 12, no. 2, 2020, p. 447.
Asemi, Z., et al. “Association between Markers of Systemic Inflammation…” ARYA Atherosclerosis, vol. 9, no. 3, 2013, pp. 172–178.
Sies, Helmut. “Oxidative Stress: A Concept in Redox Biology and Medicine.” Redox Biology, vol. 4, 2015, pp. 180–183.
Burton, G. J., and E. Jauniaux. “Oxidative Stress.” Best Practice & Research Clinical Obstetrics & Gynaecology, vol. 25, no. 3, 2011, pp. 287–299.
Agarwal, A., et al. “Role of Oxidative Stress in Female Reproduction.” Reproductive Biology and Endocrinology, vol. 3, 2005, p. 28.
Myatt, L., and X. Cui. “Oxidative Stress in the Placenta.” Histochemistry and Cell Biology, vol. 122, no. 4, 2004, pp. 369–382.
Aly, S., et al. “Effects of Oral Iron (Ferrous versus Ferric) Supplementation…” Egyptian Journal of Haematology, vol. 41, no. 2, 2016, pp. 31–41.
Falahi, E., et al. “Impact of Prophylactic Iron Supplementation…” Food and Nutrition Bulletin, vol. 32, no. 3, 2011, pp. 213–217.
Khalid, S., et al. “Effects of Oral Iron Supplements in Pregnancy…” Pakistan Journal of Public Health, vol. 14, 2024, pp. 133–137.
Rogozińska, E., et al. “Iron Preparations for Women…” The Lancet Haematology, vol. 8, no. 7, 2021, pp. e503–e512.
