
+91 6002993949
submission@iarconsortium.org
Open Access
ISSN (Print) : 2788-953X
ISSN (Online) : 2788-9548
Pneumarthrosis or vacuum phenomenon is seen in many joints where excessive movement is there as a part of degenerative process. This causes a lot of potential confusion in the diagnosis and further to study the details of joint anatomy. The vacuum phenomenon of glenohumeral joint (GJVP) is as a result of normal physiological conditions where the gas collects in the joint. This is more common in intervertebral discs as compared to other locations. These are noticed as incidental findings in asymptomatic patients but may be noticed in other conditions associated with discogenic pain. We present 37-yr male with chronic kidney disease CKD) who underwent routine high resolution computed tomography (HRCT) of chest for evaluation of breathlessness. Though there was no complaint of either of the shoulder joint, but bilateral intraarticular gas was present. These findings were without any underlying degenerative changes or any infective joint pathology. Bilateral GJVP was noticed as incidental finding and was considered to be due to the disturbed underlying physiology because of long standing renal ailment. No treatment was advocated in this case except the permitted physiotherapy.
Glenohumeral joint is diarthroidal multiaxial ball and socket joint. There is articulation of humeral head with the glenoid cavity of scapula.Intraarticular gas or air is called as pneumarthrosis.Vaccum phenomenon is the collection of the gas within the joint GJVP have not been studied much in clinical practice [1].This could be because of various underlying causes and the most common is trauma compound injury.Pseudogout can also cause this type of presentation. Nitrogen bubbles can be seen in the form of this gas.Fick in 1910 reported pneumaarthrosis first time.
Case report
37-years male, a known case of CKD reported for HRCT of chest for evaluation of breathlessness of six months duration. Patient is having hypertension of ten years duration but now under control for the last one year.Patient was conscious with vitals stable but was regularly undergoing dialysis due to CKD. Serum creatinine was 11mg/dL and blood urea 70mg/dLPlain chest radiograph was essentially normal except both the shoulder show air lucencies (Figure 1). HRCT chest was done to rule out any lung pathology (Figure 2a, b and c). There was incidental finding of bilateral air in glenohumeral joints. The presentation on both sides was in the form of radiolucent crescent (Figure 3a and b). There were no degenerative changes seen in both the joints in the form of joint narrowing with subchondral cysts or associated sclerosis.
There was no need of any treatment and further work-up required in this case. Patient had been advised to continue the treatment for CKD and physiotherapy may be contemplated if there is pain in any of the shoulder.
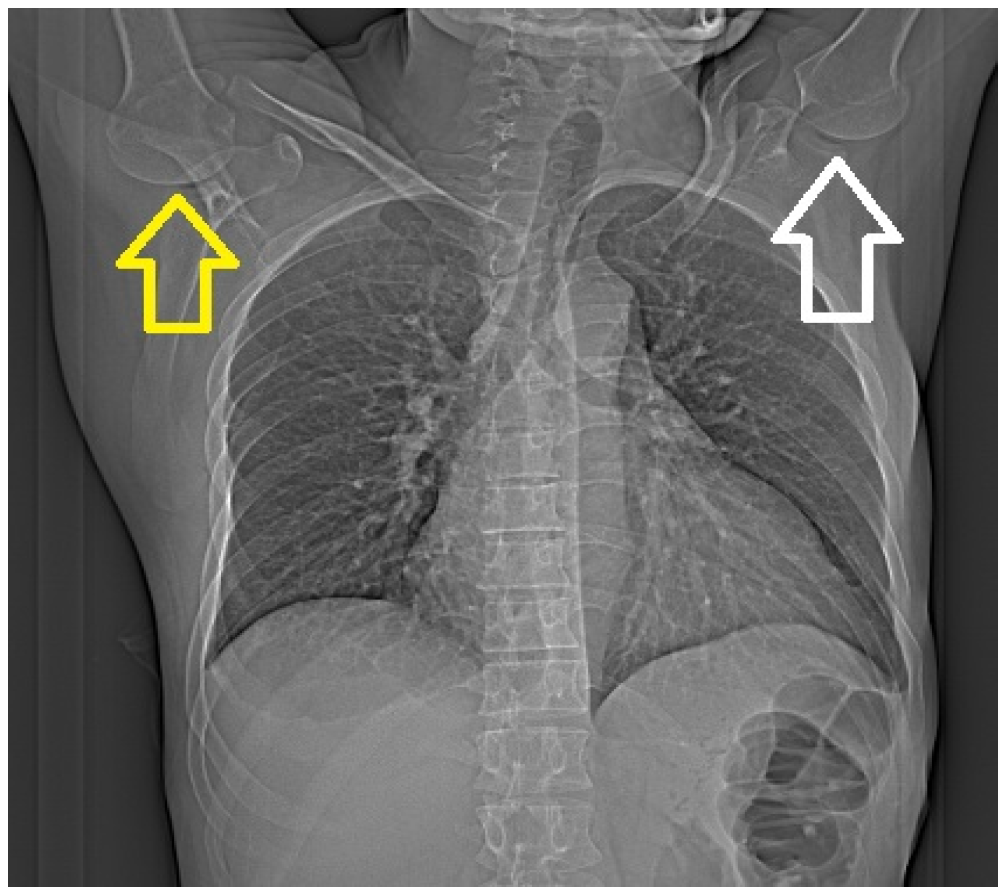
Figure 1: Plain Chest Radiograph Postero-Anterior View. There are Subtle Arc Shaped Lucencies in Both Right (Yellow Arrow) as Well as Left (White Arrow) Shoulder Joints.Rest of the Radiograph does not Show Any Abnormality
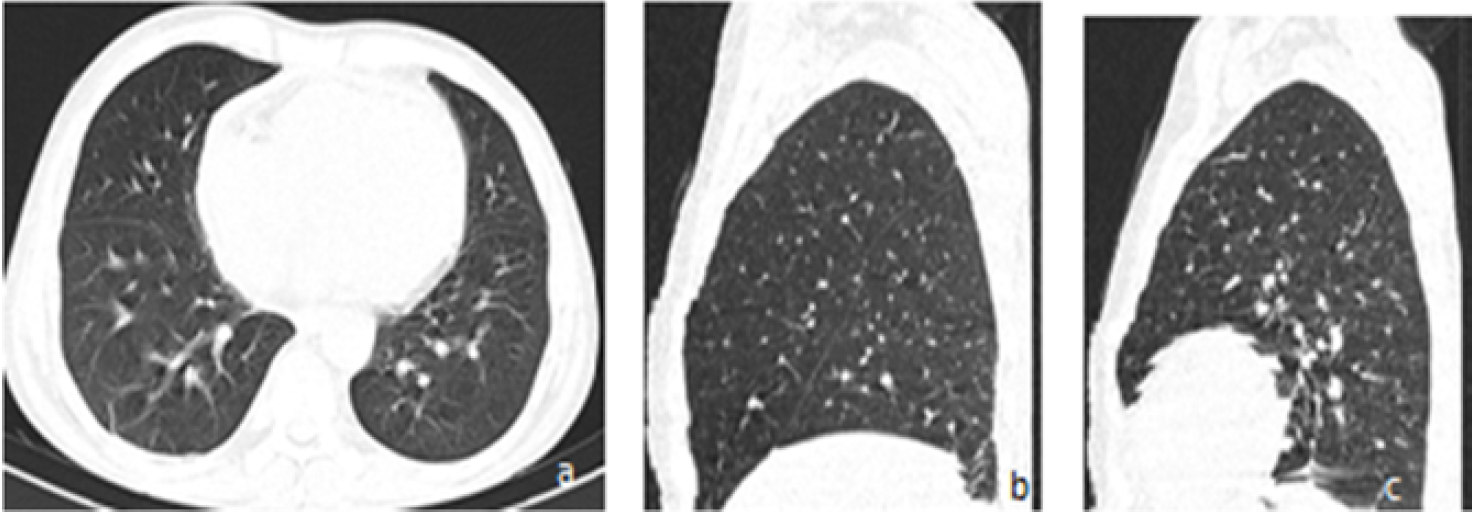
Figure 2: HRCT Chest in Lung Window.A) Axial Section in Mid Chest Region.B) Right Lung in Sagittal Section. C) Left Lung Insagittal Section. No Abnormality Noticed in Lung Parenchyma
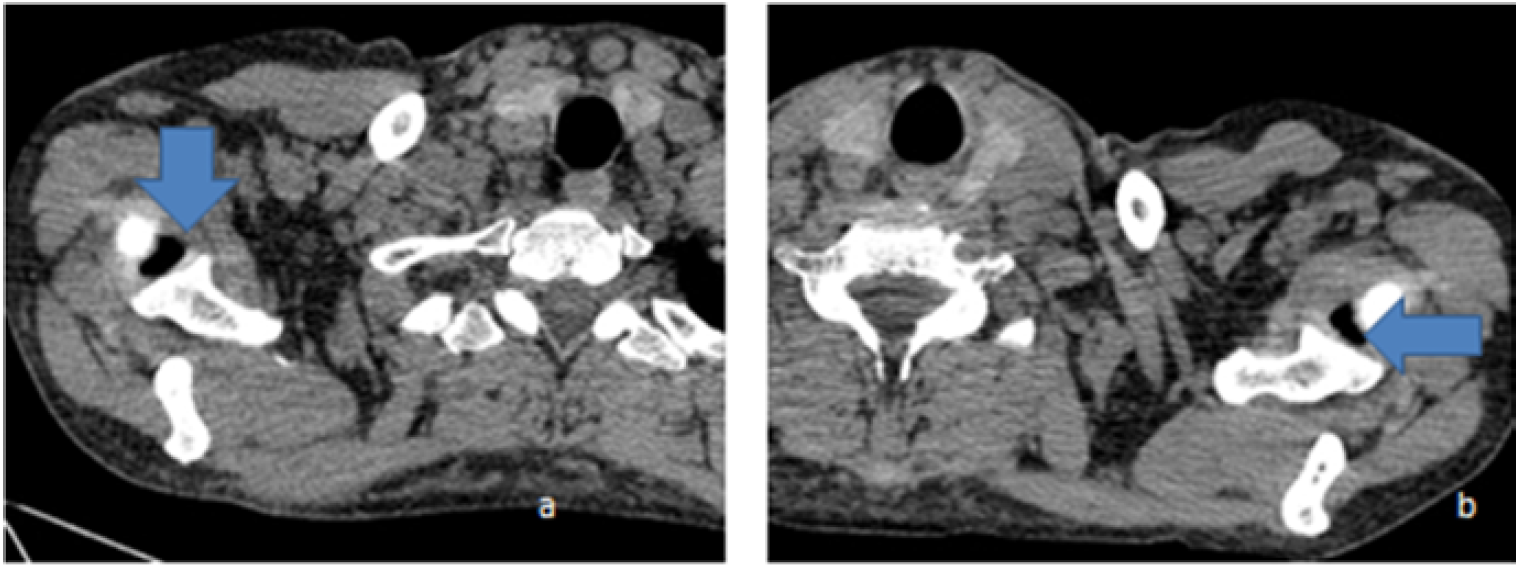
Figure 3: Axial Section of Upper Chaes in Mediastinal Window. A) Right Glenohumeral Joint Shows a Pocket of Air Lucency (Inverted Arrow) in the Joint Space. B) Left Glenohumeral Joint Shows Another Pocket of Air Lucency on the Medial Aspect of the Joint (Horizontal Arrow)
Vacuum phenomenon (VP) had been noticed more common in spine as compared to peripheral articulation. VP can be related to gas solubility,pressure-volume relationship in the background of human physiology.The incidence is considered to be due to negative pressure in the intraarticular region [2]. Arvidsson formulated that 400-600 n force is necessary to create the vacuum phenomenon.Glenohumeral joint is stabilized by superior, middle and inferior glenohumeral ligaments. This is synovial joint and the articular cartilage is covered by hyaline cartilage.Vaccum phenomenon is the presence of intraarticulr gas which is quite evident in external rotation. Trauma can lead the laceration of the capsule and subjected to exposing of the sterile internal component to the external environment. The gas in spinal region could be the reason for the unexplained backache (somatic and radicular pain). Gas chromatography had shown 90%-92% content as nitrogen.The air is withdrawn from the surrounding soft tissues which are rich in nitrogen.GRE MR images can highlight the foci of gas as linear or circular shadows of low signal intensities in the glenohumeral intraarticulr location. The diagnosis can avoid the pitfall of misinterpretation or misdiagnosis of loose bodies or chondrocalcinosis. This is a benign condition and frequently noticed in plain radiograph. The phenomenon had also been evaluated by ultrasound,CT and MRI [3,4]. US can pick up the quantity of gas as less as 0.5 ml in the form of echogenic foci in the intraarticular region. Plain radiograph requires at least 2 ml of air in the joint. CT and MRI are considered as gold standard investigation to detect vacuum phenomenon [5,6,7]. Vacuum sign can also be noticed in infants while conducting plain chest radiograph .This sign can disappear in delayed films. Ray et al.reported this phenomenon in a child of road traffic accident without any fracture. This could also be possible due to soft tissue injuries [8]. VP in shoulder joint must be compared to the underlying degenerative changes in the joint like joint space narrowing, subchondral cysts and sclerosis. Inferior humeral head can show “bearded goat sign” depicting osteophytes in osteoarthritis. In our case there were no degenerative changes but the phenomenon had appeared because of disturbed physiology due to CKD.
There are many lacunae in interpreting the air in the shoulder joint. Though this is benign condition but the history with the background is very important. The vacuum phenomenon may be incidental finding or in those patient who come with different symptomatology. This is more common in spinal region as compared to extra axial locations.The incidence of CP may be a common feature among the patients of comorbidities as was in our case who had CKD.
Acknowledgement
We are thankful to Mr Brijesh and Mr Arun our computer assistants for providing the necessary input in preparing this manuscript.
Conflict of interest
There was conflict of interest
Ethical issue
No ethical issue involved.
Financial support
None
Gohil I., Vilensky J.A. and Weber E.C. “Vacuum phenomenon: clinical relevance.” Clinical Anatomy vol. 27, 2014, pp. 455–462.
Cianci F. et al. “Comprehensive review on intravertebral, intraspinal, intra-articular and intradiscal vacuum phenomenon: from anatomy and physiology to pathology.” Modern Rheumatology 2020, pp. 1–9. https://doi.org/10.1080/14397595.2020.1764744
Lee T.H. et al. “Computed tomographic demonstration of the vacuum phenomenon in the subtalar and tibiotalar joints.” Foot and Ankle International vol. 15, 1994, pp. 382–385. https://doi.org/10.1177/107110079401500707
Patten R.M. “Vacuum phenomenon: a potential pitfall in the interpretation of gradient-recalled-echo MR images of the shoulder.” American Journal of Roentgenology vol. 162, no. 6, 1994, pp. 1383–1386. https://doi.org/10.2214/ajr.162.6.8192004
Grechenig W. et al. “Sonographic detection of air in the knee joint: an experimental study and clinical case report.” Ultraschall in der Medizin vol. 23, 2002, pp. 47–51. https://doi.org/10.1055/s-2002-2007
Stallenberg B. et al. “The vacuum phenomenon: a CT sign of nonunited fracture.” American Journal of Roentgenology vol. 176, no. 5, 2001, pp. 1161–1164. https://doi.org/10.2214/ajr.176.5.1761161
Ito H. et al. “MDCT demonstration of intra-articular gas in the glenohumeral joint and sternoclavicular joint with reference to arm position.” Radiation Medicine vol. 26, no. 7, 2008, pp. 422–425. https://doi.org/10.1007/s11604-008-0253-8
Ray P. et al. “Vacuum phenomenon in the shoulder of a child.” BMJ Case Reports vol. 12, 2019, e226724. https://doi.org/10.1136/bcr-2018-226724
