+91 6002993949
submission@iarconsortium.org
Open Access
ISSN (Print) : 2788-8843
ISSN (Online) : 2788-8851
Key findings:
Key findings include: a total of [insert number] participants were included in the cross-sectional study, with [insert number] individuals in the diabetic patients and [insert number] in the non-diabetic patients. Significant differences were found in the levels of sodium, potassium, calcium, and magnesium between the two groups, providing valuable insights into the serum electrolyte imbalance in diabetes mellitus patients.
What is known and what is new?
What is known is the importance of electrolyte balance in diabetes management. What is new is the specific study comparing serum electrolyte levels in diabetic and non-diabetic patients, providing valuable insights into the serum electrolyte imbalance in diabetes mellitus patients and its potential clinical implications.
What is the implication, and what should change now?
The implication is that diabetic patients have significant differences in serum electrolyte levels compared to non-diabetic patients. Changes needed include further research to explore the clinical implications of these differences and their potential impact on overall health and well-being, as well as potential adjustments to treatment plans to address these imbalances.
Assessing serum electrolytes in both diabetic and non diabetic patients is crucial for understanding their overall health and managing specific conditions .Electrolytes are minerals in the body that have an electric charge and are essential for various physiological function .In the context of diabetes mellitus, monitoring serum electrolyte levels is particularly important due to the potential imbalances caused by the disease and its complications.
In Diabetic Mellitus Patients:
Hyperglycemics Impact : High blood sugar levels in diabetes can lead to increased urination and subsequent loss of electrolytes, especially urine .
Electrolyte Imbalance: Diabetic ketoacidosis (DKA) is a severe complication of diabetes where the body starts breaking down fat for energy, leading to ketone production and electrolyte imbalances, including low potassium levels.
Renal Function: Diabetes can impair kidney function. The kidneys play a vital role in maintaining electrolyte balance, and their dysfunction can lead to imbalances such as high potassium levels (hyperkalemia).
Monitoring: Regular blood tests, including serum electrolyte panels, are necessary to monitor potassium, sodium, chloride, and bicarbonate levels. Abnormalities can indicate complications and guide appropriate interventions.
In Non-Diabetic Mellitus Patients:
Baseline Measurement: Electrolyte levels in non-diabetic patients serve as a baseline for comparison when evaluating patients with diabetes. Deviations from these baseline values can indicate diabetes-related complications.
Differential Diagnosis: Certain electrolyte imbalances, like hyperkalemia, can occur in both diabetic and non-diabetic patients. Investigating the cause is crucial for accurate diagnosis and treatment planning.
Chronic Conditions: Non-diabetic patients might have underlying chronic conditions that can affect electrolyte balance, such as kidney disease or hypertension. Monitoring electrolyte levels helps in managing these conditions effectively.
Treatment Response: For non-diabetic patients with electrolyte imbalances, regular assessments are essential to evaluate the response to treatments such as diuretics, supplements, or dietary modifications.
In both cases, healthcare providers use the results of serum electrolyte assessments to tailor treatments, prevent complications, and ensure overall patient well-being. Regular monitoring and appropriate interventions based on these assessments are essential components of managing diabetes mellitus and other health conditions.
Diabetes is a chronic disease that occurs either when the pancreas does not produce enough insulin or when the body cannot effectively use the insulin it produces. Insulin is a hormone that regulates blood sugar. Hyperglycemia, or raised blood sugar, is a common effect of uncontrolled diabetes and over time leads to serious damage to many of the body's systems, especially the nerves and blood vessels.
In India, there are estimated 77 million people above the age of 18 years are suffering from diabetes (type 2) and nearly 25 million are prediabetics (at a higher risk of developing diabetes in near future). More than 50% of people are unaware of their diabetic status which leads to health complications if not detected and treated early.
Effect Of Electrolytes In Diabetic Mellitus
Diabetic patients frequently develop a constellation of electrolyte disorders. These disturbances are particularly common in decompensated diabetics, especially in the context of diabetic ketoacidosis or nonketotic hyperglycemic hyperosmolar syndrome. These patients are markedly potassium-, magnesium- and phosphate-depleted.
Diabetes mellitus (DM) is linked to both hypo- and hyper-natremia reflecting the coexistence of hyperglycemia-related mechanisms, which tend to change serum sodium to opposite directions. The most important causal factor of chronic hyperkalemia in diabetic individuals is the syndrome of hyporeninemic hypoaldosteronism.
Impaired renal function, potassium-sparing drugs, hypertonicity and insulin deficiency are also involved in the development of hyperkalemia.
1.A Review Of Diabetes Mellitus And Its Complications. By Ansu Ismail And Safeera Ali. On May 30, 2022
Diabetes mellitus has quadrupled in global prevalence during the last three decades, which is now the ninth leading cause of mortality. Around 1 in 11 persons globally today has diabetes, with 90% of those suffering from diabetes mellitus (DM). Asia is a significant hotspot for global DM epidemic, with China and India serving as the top two epicenters. Individual vulnerability to DM is partly determined by genetic predisposition,but a poor diet and sedentary lifestyle are major drivers of the current global epidemic;early developmental variables (such as prenatal exposures) also have a role in susceptibility to DM later in life.
2. A Literature Review Of Complementary And Alternative Medicine Used Among Diabetes Mellitus Patients. By Snita Joeliantina, Oedojo Soedirham, Mangstuti Agil. June 1:2019
Diabetes is a chronic disease that requires regular and sustainable health management that involves proper treatment. Some diabetic patients use CAM, as well as conventional medicine, to maintain their health and control their blood sugar. This literature review aimed to 1)determine the prevalence of CAMused by patients with diabetes, summarize and evaluate the CAM use that includes:characteristics,patterns types and reason, 2) propose a conceptual model associated with CAM used by patients with diabetes. Systematic reviews were searched using an electronic database. The systematic reviews were published between 2005 and 2015 by using specific keywords. The number of systematic reviews obtained as a search result is 14 articles from 14 countries.
3. Challenges Of Type 2 Diabetes Mellitus Management From The Perspective Of Patients: Conventional Content Analysis. By Soghra Nikpour, Neda Mehrdad, Mahnaz Sanjari, Ramin Heshat. 15:8:2022
Patients with type 2 diabetes mellitus (T2DM) face significant challenges in the treatment process, which can have a negative impact on disease management. Proper management of the disease can reduce symptoms and complications, improve glycemic indices, and reduce mortality and readmission.
4. Comparative Analysis Of Fasting Blood Glucose And Salivary Electrolytes Concentration Among Individuals With Type Ll Tarela Diabetes. By Victor Onyemaechi Egboh , Pegee Ejiro Ohwin, Melish Elias Daubry.30 May 2022
Salivary gland dysfunction is common in people with diabetes.this study aimed to compare the measurements of salivary electrolyte (SE):Na+, K+, Cl- between diabetes and age matched control group and assess the relationship between fasting blood glucose (SG). Eighty-five human participants [diabetes group, n=45 (23 males and 20 females)] aged between 25 and 65 years were tested. Saliva samples were taken between 7.00am and 8.00am after an overnight fast and SG and AE concentrations were analyzed.
Site Of Study : Central Laboratory Of Acs Medical College And Hospital.
Period Of The Study : Six (6) Months
Type Of Study : Cross-Sectional
Sample Size :100 Blood Sample
* Estimation of FBS and PPBS to determine the difference in serum electrolytes Na+ ( sodium) , k+ ( potassium), Cl- ( Chloride) between diabetic and non diabetic patients by Beckman Coulter fully automated machine.
* The study was conducted as a cross sectional study. The study population was derived from the apparently ambulatory persons from ACS MEDICAL COLLEGE AND HOSPITAL. The proposal of the study was put forth in the meeting of the ethical committee of the institute and necessary permission and clearance were obtained.
* These subjects were selected randomly.
Details To Be Recorded:
Samples collected (i.e. blood [which tubes and how many and in which order]).
Date and time the samples were taken (blood).
Last time the subject consumed food/drink.
Venepuncture Procedure
Select a vein by observation and palpitation (lightly tapping the vein). Listen to the subject as they will often advise on the best or only site for venipuncture.
Place the tourniquet around the subject’s upper arm or lower arm 10 cm above the venipuncture site. Note: To avoid pinching of the skin, place the tourniquet over the subject’s sleeve. Alternatively, place a cotton wool pad under the buckle of the tourniquet.
Ask the subject to clench their fist. If the vein is not visible or palpable, ask the subject to “pump hand” or dangle arms over the hand rest of the chair.
If still not visible, lightly tap antecubital fossa or dorsal surface of hand.
Disinfect the puncture site well with alcohol skin wipe and allow the skin to dry. Note: It is important that the skin is completely dry to avoid discomfort when inserting the needle.
Ask the subject to relax hand/arm in a downward position.
Remove the cap from the needle, position the needle parallel with the vein with the bevel uppermost and insert it into the vein.
Push the first tube into the needle holder and onto the needle valve, puncturing the rubber stopper. Hold the tube vertically, below the donor’s arm during blood collection.
Techniques To Prevent Hemolysis (Which Can Interfere With Many Tests)
Avoid drawing blood from a hematoma; select another draw site.
If using a needle and syringe, avoid drawing the plunger back too forcefully.
Make sure the venipuncture site is dry before proceeding with draw.
Avoid a probing, traumatic venipuncture.
Avoid prolonged tourniquet application (no more than 2 minutes; less than 1 minute is optimal).
Avoid massaging, squeezing, or probing a site.
Avoid excessive fist clenching.
If blood flow into the tube slows, adjust needle position to remain in the center of the lumen.
Centrifugation
Inspect the centrifuge to ensure it is working properly, there is no damage, and that the centrifuge is able to move freely.
Select the appropriate centrifuge tubes or containers, inspect them to make sure there are no cracks or flaws. Discard any tubes/containers that are cracked or flawed.
Fill tubes with the desired liquid. a. Never overfill or underfill the tubes or containers (follow the manufacturer’s limits).
Make sure that the centrifuge tubes are balanced, use a balance to ensure that the weights of both tubes match. a. Do not balance based purely on volume! This is especially true for solutions with different samples or different concentrations of the same sample.
Tightly secure the lids on the centrifuge tubes.
Make sure that the outside of the centrifuge tubes are clean and dry before placing them in the centrifuge.
Balance the tubes within the centrifuge.
Close the lid. Make sure the lid has a tight fit.
Set the run speed and run time. (Never use the rotor’s maximum run speed).
I used the Beckman Coulter Au480 fully automated analyzer from ACS Medical College and Hospital for glucose and electrolyte parameters.
Prepare Sample For Analysis
Before starting analysis, dispense a sample into sample cups/tubes and set these cups/tubes in the correct rack.
Racks are placed on the rack supply unit. Racks can be continuously loaded on the rack supply unit as space is available.
Place The Sample Cups/Tubes In A Rack
Place each sample in the correct rack. Racks are color coded. Each color indicates a different type of analysis.
To analyze the samples, I utilized a white color rack.
Look at each opening in the rack and ensure the barcode is aligned in the center. 2 mm is the most each barcode should deviate from the center.
Placing Racks On The Rack Supply Unit
Open the sample protection cover.
Place the racks on the rack supply unit
Close the sample protection cover.
Enter Manual Requisitions For Routine And Emergency Samples
Select Home > Rack Requisition Sample > Sample > Test Requisition
Select Switch for Sample Kind to select Routine. ( Routine): Routine analysis in a white rack.
Select the sample type from the "Type" drop-down list.
Select Start Entry (F1). The window changes to the edit mode.
For Sample ID, enter the sample barcode number.
If a manual dilution was made on the sample, select Sample Dilution (F7) and enter the sample dilution rate.
Select the test(s) to run on the sample glucose ,sodium, potassium and chloride.
A test highlights in blue when it is requisitioned. Select the test again to cancel the requisition. Tests highlighted in gray are not operational for the sample type selected.
When selecting a profile, perform one of the following operations: a. Select Profile to open the profile window and select a profile (or multiple profiles). b. Use the keyboard to enter a profile number into Profile and press.
Select the Demographics tab to enter any required patient demographic information.
Confirm the entered information and select Entry (F1). The entered information is programmed.
Repeat steps 5 through 10 to requisition additional samples in the same Sample Kind and Type. To change the Sample Kind or Type, select Exit (F2) and repeat steps 2 through 10.
View Sample Information
Select Sample Status to view sample information, time to completion, and results
Select Home > Sample Status
Highlight a sample, then select Detail to view detailed sample information. The test name displays with the result when the result is complete.
Select Real Time Display to view the sample results.
Results can be printed from Home > Sample Manager at any time.
General Precautions
Gloves must be worn at all times when handling specimens. This includes during removal of the rubber stopper from the blood tubes, centrifugation, pipetting, disposal of contaminated tubes, and clean up of any spills. Tubes, needles, and pipets must be properly disposed of in biohazard containers, in accordance with institutional requirements.
Universal precautions and institutional requirements should be followed, including gloves, eye protection or working in a biosafety cabinet for blood processing. All equipment (storage, shipping, and centrifuge) must be labeled as biohazard.
It is important to take steps to prevent hemolysis in blood samples. A vacutainer is recommended. If a needle is used, a 21 gauge needle is recommended.
Contents of tubes that contain chemical additives may be irritating to eyes, respiratory system and skin.
For safety information regarding sample tubes and risks associated with venepuncture please refer to the manufacturer's product guidelines and/or your institution's risk assessment.
The sample tubes contain additives. It is important to follow the correct order of draw to prevent contamination of samples.
Data were analyzed with the help of the software program statistical package for social sciences(SPSS). The statistical differences in serum electrolytes (Na+, K+, Cl-) between diabetic and non diabetic people . The p-value 0.005 were considered as statistically highly significant
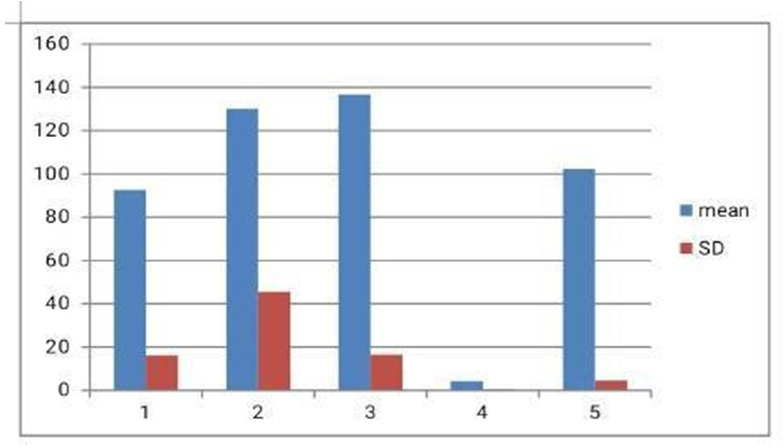
This Graph Represent The Non Diabetic Patients Mean And Standard Value :
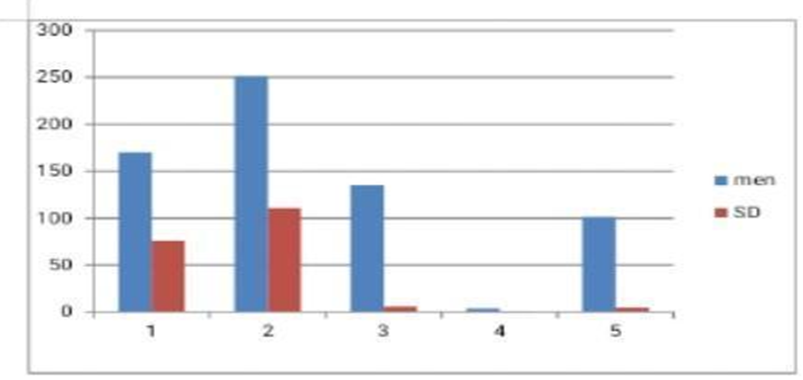
This Graph Is Represent The Diabetic Patients Mean And Standard Values :
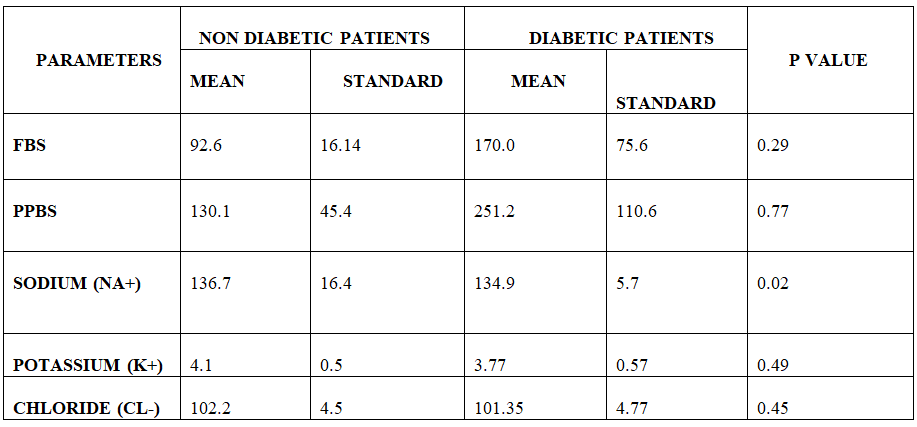
Pearson correlation * P < 0.05 is statistically significant
The assessment of serum electrolytes in both diabetic mellitus (DM) patients and non-diabetic patients is crucial for understanding their overall health status. Here's a discussion comparing the assessment of serum electrolytes in these two groups:
Diabetic Mellitus Patients:
Potassium (K+): DM patients are at risk of hyperkalemia due to kidney dysfunction, a common complication. Elevated potassium levels can lead to heart rhythm abnormalities. Monitoring potassium levels is essential, especially if they are on medications that affect potassium balance.
Sodium (Na+): Hyponatremia can occur due to increased urination and dehydration in DM patients. Low sodium levels can cause confusion, seizures, and coma. Hypernatremia might occur if excessive thirst leads to increased sodium intake.
Chloride (Cl-): Chloride levels might be affected due to changes in sodium and potassium levels. Imbalances can impact blood pH and fluid balance.
Non-Diabetic Mellitus Patients:
Potassium (K+): Typically, potassium levels in non-diabetic individuals are maintained within the normal range. Imbalances might occur due to kidney disorders, medications, or dietary factors.
Sodium (Na+): Non-diabetic individuals generally maintain stable sodium levels. Imbalances can result from dehydration, kidney issues, or certain medications.
Chloride (Cl-): Chloride levels are usually regulated within a narrow range in non-diabetic patients. Imbalances might occur due to underlying health conditions affecting the kidneys or digestive system.
In conclusion, serum electrolyte levels in diabetic mellitus patients and non-diabetic individuals can vary based on several factors, including kidney function, medication, diet, and overall health. Diabetic mellitus patients are at an increased risk of electrolyte imbalances, such as hyperkalemia and hyponatremia, due to complications related to their condition. Regular monitoring of electrolyte levels is crucial for both diabetic and non-diabetic individuals to detect and manage imbalances promptly. Healthcare professionals play a vital role in assessing these levels, tailoring treatment plans, and ensuring the overall well-being of their patients. It's important to consult with a healthcare provider for specific conclusions based on individual cases and test results.
The serum electrolyte parameters values,
Serum Na+ (Sodium) in diabetic patients are too prone to hyponatremia.
Serum K + (Potassium) in diabetic patients are too prone to hypokalemia condition.
Serum Cl- (chloride) in diabetic patients are not affected that much.
In this statistical the outcome of electrolytes P value :
P value of sodium ( Na+) -0.02
P value of potassium ( K+) – 0.049
P value of chloride (Cl-) -0.45
The serum electrolytes are statistically significant in diabetic patients as compared to the non diabetic patient.
Funding: No funding sources.
Conflict of interest: None declared.
Ethical approval: The study was approved by the Institutional Ethics Committee of DR.MGR Education and Research Institute.
1. Ashraf R, Naikoo NA, Bashir H, et al. Research Article Electrolyte Imbalance in the Patients Admitted to the Emergency Department of the Tertiary Care Hospital of Smhs Hospital. Srinagar; (2018).
2. Anago EAA, Medehouenou TCM, Akpovi CD, Tchehouenou H. Electrolyte disturbances in diabetic patients in Cotonou, Benin. Int J Res Med Sci. (2016);4(12):5430–5435.
3. Ahmed SS, Nur F, Ullah R, Al Mamun A. Factors precipitating hypokalemia in diabetic patients: a cross sectional study. J Enam Med Col. (2014);4:145–150. doi: 10.3329/jemc.v4i3.20940
4. Article O. Prevalence of abnormal serum sodium and potassium concentration in paediatric new onset type 1 diabetes with ketoacidosis: a retrospective study from two Nigerian teaching hospitals. Sri Lanka J Diabetes Endocrinol Metab. 2018;8(1):32–39.
5. Bhave G, Neilson EG. Volume depletion versus dehydration: How understanding the difference can guide therapy. Am J kideny dis. 2011;58(2):302–309.
6. Bishop ML, Fody EP, Schoeff LE. Clinical Chemistry: Techniques, Principles Correlations. Philadelphia: Library of Congress; 2010.
7. Barkas F, Elisaf M. Diabetes Mellitus and Electrolyte Disorders. World J clin cases. 2014.
8. Billah MM, Rana SMM, Akter N, Hossain MS. Analysis of serum electrolyte and lipid profile in young Bangladeshi female with type II diabetes. Cogent Biol. 2018;4(1):1–10. doi: 10.1080/23312025.2018.1431474
9. Braun MM, Army M, Barstow WCH, et al. FEFF diagnosis and management of sodium disorders: hyponatremia and hypernatremia. Am Fam Physician. 2015;91(5).
10. Chatterjee R, Yeh HC, Edelman D, Brancati F. Potassium and risk of type 2 diabetes. Expert Rev Endocrinol Metab.2011;6(5):665–672. doi:
11.1586/eem.11.60. Clinic M, Hospital Z, Clinical N, Hospital J. Acid-base and electrolyte managements in chronic kidney disease and end-stage renal disease: case-based discussion. Blood Purif. 2018;55905:179–186.
12. Engwa GA, Nwalo FN, Attama TC, Abonyi MC. Influence of type 2 diabetes on serum electrolytes and renal function indices in patients. J Clin Diagn Res. 2018;12(6)13–16.
13. . Global report on diabetes.
14. G. D. .Shoback, “New York: McGraw-Hill Medical.,” Greenspan’s basic & clinical endocrinology (9th ed.)., 2011
15.Houston MC, Harper KJ. Potassium, magnesium, and calcium: their role in both the cause and treatment of hypertension. J Clin Hypertens (Greenwich). 2008
16. Hasona NA, Elasbali A. Evaluation of Electrolytes Imbalance and Dyslipidemia in Diabetic Patients. Med.Sci. 2016;
17. Id KT, Nymo H, Louch WE, Ranhoff AH, Erik Ø. Electrolyte imbalances in an unselected population in an emergency department: a retrospective cohort study. PloS one. 2019.
18. Icin T, Medic-stojanoska M. Multiple causes of hyponatremia: a case report. Medical Princ Pract. 2017.
19. Jha NK. Study of lipid profile & electrolyte levels in diabetes. J Med Health Res. 2017.
20. Liamis G. Diabetes mellitus and electrolyte disorders. World J Clin Cases. 2014
21. Liamis G, Rodenburg EM, Hofman A, Zietse R. Electrolyte disorders in community subjects: prevalence and risk factors. AJM. 2013.
22. Larry Jemson J. Harrison`s Endocrinology. New York, Chigago: McGraw-Hill Companies; 2010.
23. Liamis G, Tsimihodimos V, Elisaf M. Hyponatremia in diabetes mellitus: clues to diagnosis and treatment. J Diabetes Res Clin Metab. 2015.
24. Liamis G, Tsimihodimos V, Elisaf M. Hyponatremia in diabetes mellitus: clues to diagnosis and treatment. J Diabetes Res Clin Metab. 2015;6(6).
25. Mcpherson RA, Pincus MR. HENRY ’ S Clinical Diagnosis and Management by Laboratory Methods. New York: Elsevier; 2011.
27. Nagai K, Ueda S, Tsuchida K, Doi T, Minakuchi J. Low serum sodium concentration is a prognostic factor related to current blood glucose level in stable hemodialysis patients: an observational study. Renal Replacement Therapy. 2017
28. Perez GO, Oster GR, Rogers AW . Acid-Base Disturbances in Gastrointestinal Disease. Digestive diseases and sciences. 1987
29. Perez V, Chang ET. Sodium-to-potassium ratio and blood pressure, hypertension, and related factors .
30. Rana AK, Ray S. Dyselectrolytemia in hyperglycaemic crisis patients with uncontrolled non-insulin dependent diabetes mellitus. Int J Med Res Health Sci. 2017
33. Saito T, Ishikawa S, Higashiyama M. Inverse distri bution of serum sodium in patients with diabetes uncontrolled and potassium mellitus in. Endocr J. 1999
34. Sahay M, Sahy R. Hyponatraemia: A practical approach. Indian J Endocrinol Metab. 2014
35. Tzamaloukas AH, Ing TS, Siamopoulos KC, et al. Pathophysiology and management of fluid and electrolyte disturbances in patients on chronic dialysis with severe hyperglycemia. Semin Dial. 2008.
36. Topaloglu AK, Yildizdas D, Yilmaz HL, Mungan NO, Yuksel B, Ozer G. Bone calcium changes during diabetic ketoacidosis: a comparison with lactic acidosis due to volume depletion. Bone. 2005.
37. Vairo D, Bruzzese L, Marlinge M, et al. Towards addressing the body electrolyte environment via sweat analysis: pilocarpine iontophoresis supports assessment of plasma potassium concentration. Sci Rep. 2017.
38. WHO. Guideline: Potassium Intake for Adults and Children. Geneva: World Health Organization (WHO); 2012.
39 . Wang S, Hou X, Liu Y, et al. Serum electrolyte levels in relation to macrovascular complications in Chinese patients with diabetes mellitus. Cardiovasc Diabetol. 2013.
