+91 6002993949
submission@iarconsortium.org
Open Access
ISSN (Print) : 2788-8843
ISSN (Online) : 2788-8851
Groove pancreatitis (GP) is a rare form of chronic pancreatitis that imitate pancreatic malignancy specifically adenocarcinoma. Groove pancreatitis involves pancreaticoduodenal groove whichis potential space between the head of the pancreas, duodenum and common bile duct (CBD). Accurate radiological diagnosis of groove pancreatitis is a challenging task because of overlapping imaging findings with the pancreatic head neoplasm.Common radiological findings in groove pancreatitis include duodenal wall thickening, CBD stricture, enlargement of pancreatic head, pancreatic duct dilatation.In this paper we report a case of male patient with groove pancreatitis diagnosed on computed tomography and also review clinical and imaging features of groove pancreatitis.
Groove pancreatitis is a less commonly found type of chronic pancreatitis which involve the pancreaticoduodenal groove. It is the “groove” between pancreatic head, the duodenum and the common bile duct. In 1970 Potet and Duclert first described it as cystic dystrophy of heterotopic pancreatic tissue in the duodenal wall [1]. Becker in 1973 described segmental pancreatitis in the groove area with the German word ‘Rinnenpankreatitis' [2]. Term “groove pancreatitis” was coined by Stolte et al [3].Adsay and Zamboni coined term “paraduodenal pancreatitis” in 2004 and included groove pancreatitis, cystic dystrophy of the pancreas, pancreatic hamartoma of duodenum, paraduodenal wall cyst and myoadenomatosis in it [4].Becker and Mischke in 1991 divided groove pancreatitis into two types: Pure form and segmental form. In pure form only pancreaticoduodenal groove is involved and in segmental form fibro inflammatory changes involve pancreatic head in its dorsocranial part and affect main pancreatic duct along with the pancreaticoduodenal groove [5].Various etiological factors include gastric ulcer disease, gastric surgeries, biliary system diseases, duodenal pathologies like duodenal wall cysts and pancreatitis in duodenal pancreatic heterotopia, pancreatic head cysts, disturbances of pancreatic juice outflow in Santorini's duct in the absence of the minor papilla, and hyper stimulation in consequence of chronic alcoholism [3]. Accurate radiological diagnosis of groove pancreatitis is a challenging task because of overlapping imaging findings with the pancreatic head neoplasm and gastrointestinal neoplasms of this area.Common radiological findings in groove pancreatitis include duodenal wall thickening, CBD stricture, enlargement of pancreatic head, pancreatic duct dilatation [6]. Ultrasonography specifically endoscopic ultrasonography (EUS), computed tomography (CT) and magnetic resonance imaging (MRI) are very useful radiological investigations to demonstrate imaging findings and make diagnosis of groove pancreatitis, but in number of patients specific diagnosis is difficult to make because of overlapping findings of pancreatic head, CBD, duodenal malignancies. In these cases biopsy is required for making a specific diagnosis because in pancreatic, CBD or duodenal wall cancer prompt surgical intervention is needed, in contrast to groove pancreatitis where conservative treatment is done.
Case
A 40yr old male with history of repeated episodes of the abdominal pain with nausea, vomiting and weight loss of 3 kg in past 4 weeks was referred to radiology department for CECT abdomen. The patient was a smoker with history of alcohol abuse. His serum amylase and lipase levels were raised. CECT abdomen of the patient was done which showed enlargement of the pancreatic head with loss of fat planes between the duodenum and the pancreas. Ill defined hypo enhancing soft tissue was seen in the pancreaticoduodenal groove with thickened medial wall of the duodenum.There was presence of duodenal wall cyst along the medial border leading to the narrowing of the lumen of duodenum. The main pancreatic duct was dilated. CBD was normal in its caliber.Body and tail of pancreas was normal in size and post contrast CT attenuation.Based on these findings diagnosis of the segmental form of groove pancreatitis was made. Diagnosis of pure form of groove pancreatitis was excluded because of involvement of the pancreatic head.
Other differential diagnosis that was considered was of pancreatic head malignancy ,but imaging finding of bulky head of pancreas, thickened medial wall of duodenum, duodenal wall cyst, dilated pancreatic duct, well maintained peripancreatic vessels without any signs of thrombosis and infiltration were more in favour of diagnosis of groove pancreatitis.
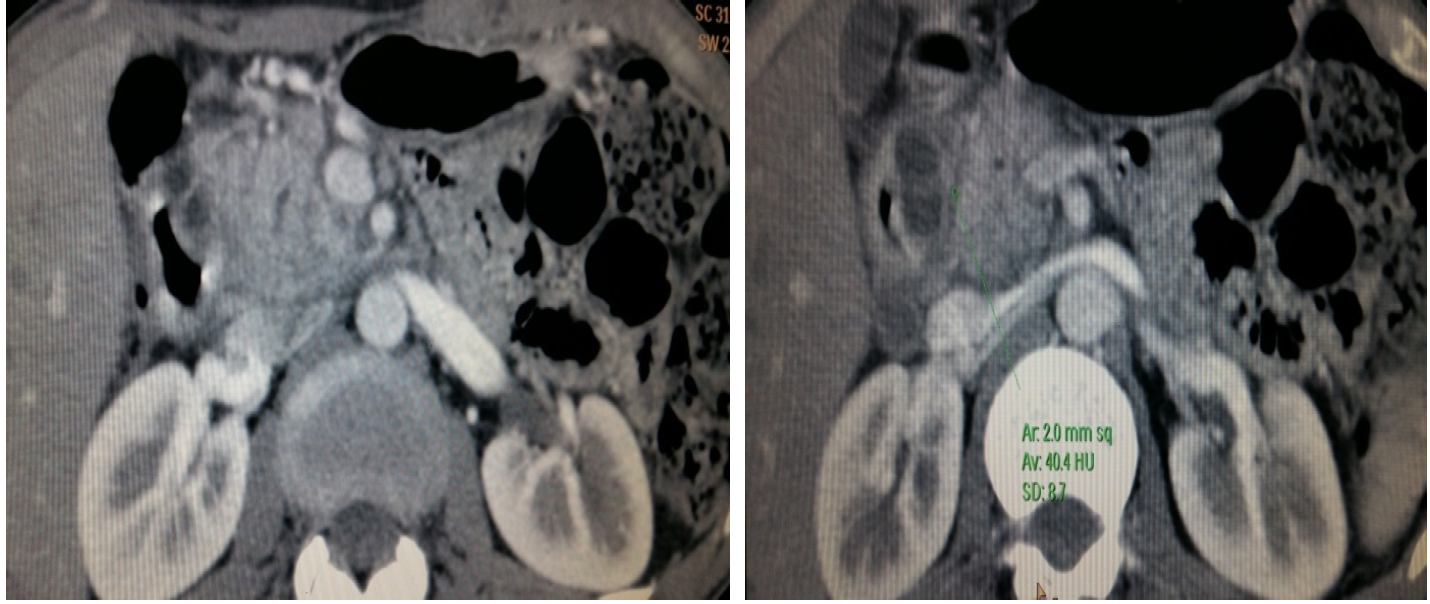
Figure 1: (a, b). Axial CECT Imagesshowing Enlargement of the Pancreatic Head with Loss of Fat Planes between the Duodenum and the Pancreas. Ill Defined Hypoenhancing Soft Tissue is also Seen in the Pancreaticoduodenal Groove. Medial Wall of the Duodenum is Thickened and there is Presence of Intramural Cyst
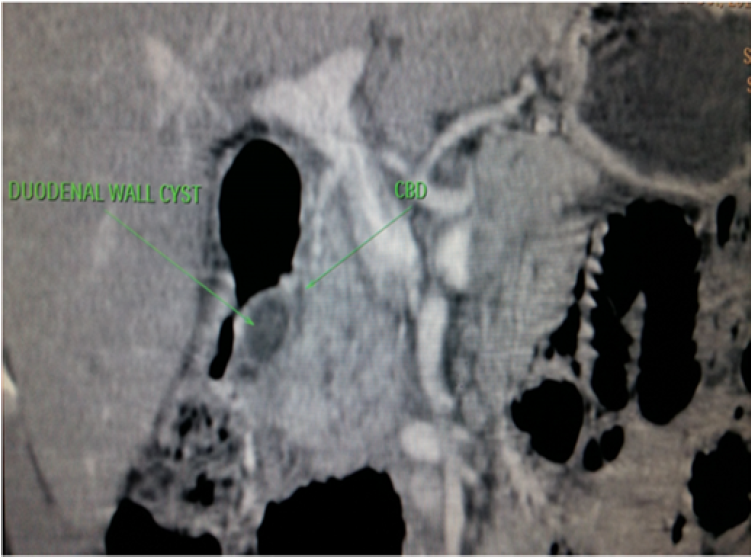
Figure 2: Coronal CECT Image Shows Duodenal Wall Cyst Leading to Narrowing of the Lumen of Duodenum, Enlarged Pancreatic Head and Relatively Hypoenhancing Tissue in the Pancreaticoduodenal Groove
Groove pancreatitis is a less commonly found type of chronic pancreatitis which involve the pancreaticoduodenal groove, a potential space between head of pancreas, CBD and duodenum. Pancreatic-duodenal artery (PDA) is an important anatomical landmark in this groove and lesions medial to PDA have pancreatic origin and those lateral to PDA have origin from duodenum or pancreaticoduodenal groove [7]. Various radiological modalities including ultrasonography, CT, MRI are very useful in making diagnosis. CT imaging features includeloss of fat planes between head of pancreas and the duodenum, ill-definedhypoenhancing soft tissue mass in pancreaticoduodenal groove which shows delayed enhancement, thickening of the medial duodenal wall, duodenal wall cysts, cysts in the pancreatic-duodenal groove, bulky pancreatic head and upstream dilatation of the MPD (in segmental form of GP), smooth narrowing of distal CBD [8,9,10]. In long standing ceases duodenal strictures can occur.MRI will also show the similar changes.MRCP is more useful in accessing caliber of distal CBD, MPD, any dilatation of the ampulla of Vater [11].
The important differential diagnosis of segmental form of GP, is adenocarcinoma of the head of the pancreas and it is very challenging to differentiate between the two preoperatively. But there are certain findings that are found in GP and not in malignancy, these are:thickening of the duodenal wall,duodenal wall cyst, cyst in groove area,smooth narrowing of intrapancreatic CBD [12,13]. GP can be differentiated from duodenal cancer, ampullary carcinoma and cholangiocarcinoma of the distal CBD as they show abrupt narrowing of CBD. It is very important to differentiate GP from the pancreatic adenocarcinoma which show pancreatic double duct cut off, upstream atrophy, infiltration into retroperitoneum and encase adjacent vessels.GP is also different from other types of acute pancreatitis as they involve greater area of pancreas and show peripancreatic inflammation (stranding, fluid) tracking into the pararenal spaces[6].
GP is a type of chronic pancreatitis that involves pancreaticoduodenal groove and have multiple aetiologies, varied clinical presentations, few specific imaging findings along with imaging findings that overlap with other disease entities. Ifthe imaging finding of GP as duodenal wall cysts, cysts in pancreaticoduodenal groove, duodenal wall thickening are absent or not conspicuous and FNAC reports are non conclusive then making a correct diagnosis is very challenging as neoplasm can't be totally excluded and pateint usually undergo pancreaticoduodenectomy (Whipple procedure). Due to this it is very important to know all the imaging features of GP which differentiate it from other disease entities, so that radiologist can confidently suggest the diagnosis and major surgery can be avoided in such cases.
Potet, F., and Duclert, N. “Cystic dystrophy on aberrant pancreas of the duodenal wall.” Archives Françaises des Maladies de l’Appareil Digestif vol. 59, no. 4, 1970, pp. 223–238.
Becker, V. “Bauchspeicheldrüse.” In Spezielle pathologische Anatomie, edited by W. Doerr, G. Seifert, and E. Uhlinger, Springer, Berlin, vol. 4, 1973.
Stolte, M. et al. “A special form of segmental pancreatitis: ‘groove pancreatitis’.” Hepato-Gastroenterologyvol. 29, no. 5, 1982, pp. 198–208.
Adsay, N.V., and Zamboni, G. “Paraduodenal pancreatitis: a clinico-pathologically distinct entity unifying ‘cystic dystrophy of heterotopic pancreas’, ‘para-duodenal wall cyst’, and ‘groove pancreatitis’.” Seminars in Diagnostic Pathology vol. 21, no. 4, 2004, pp. 247–254.
Becker, V., and Mischke, U. “Groove pancreatitis.” International Journal of Pancreatology vol. 10, year 1991, pp. 173–182.
Addeo, G. et al. “Groove pancreatitis: a challenging imaging diagnosis.” Gland Surgery vol. 8, suppl. 3, 2019, pp. S178–S187.
Raman, S.P. et al. “Groove pancreatitis: spectrum of imaging findings and radiology-pathology correlation.” American Journal of Roentgenology vol. 201, year 2013, pp. W29–W39.
Rahman, S.H. et al. “Pancreatico-duodenectomy for complicated groove pancreatitis.” HPB vol. 9, year 2007, pp. 229–234.
Vullierme, M.P. et al. “Cystic dystrophy of the duodenal wall in the heterotopic pancreas: radiopathological correlations.” Journal of Computer Assisted Tomography vol. 24, year 2000, pp. 635–643.
Ray, S. et al. “Groove pancreatitis: report of three cases with brief review of literature.” Indian Journal of Surgery vol. 79, year 2017, pp. 344–348.
Blasbalg, R. et al. “MRI features of groove pancreatitis.” American Journal of Roentgenology vol. 189, year 2007, pp. 73–80.
Shanbhogue, A.K. et al. “A clinical and radiologic review of uncommon types and causes of pancreatitis.” Radiographics vol. 29, year 2009, pp. 1003–1026.
Gabata, T. et al. “Groove pancreatic carcinomas: radiological and pathological findings.” European Radiology vol. 13, year 2003, pp. 1679–1684.
