+91 6002993949
submission@iarconsortium.org
Open Access
ISSN (Print) : 2788-8843
ISSN (Online) : 2788-8851
Background and Aim: Liver diseases are associated with low testosterone. However, little is known about risk factors of changes in testosterone. This study determined skeletal mass index in liver cirrhosis and associated risk factors with the abnormal testosterone levels. Methods: In this descriptive hospital-based study, 50 patients with evidence of liver cirrhosis diagnosed on history, imaging and investigations were included for a period of 12 months. Sarcopenia was defined as value of ≤36.5 cm2/m2 in males and ≤30.2 cm2/m2 in females. Results: The mean age was 50.4±10.1 years. The most common symptom was abdominal distension (50%) followed by upper GI bleed (30%), altered sensorium (20%), and jaundice (10%). Majority of the patients (58%) in our study were in CTP class C, followed by 16 patients (32%) in CTP class B, and 5 patients (10%) in CTP class A. 66% of the patients had low skeletal mass index. SMI was not associated with CTP class (P=0.463). Conclusion: There is a significantly higher prevalence of loss of skeletal mass in liver cirrhotic patients in this region.
Sarcopenia is a muscle wasting syndrome that is defined by a reduction in muscle mass on cross-sectional imaging.1 Sarcopenia includes a reduction in muscle strength and/or function [1]. Cirrhosis is a catabolic state in which muscle protein breakdown exceeds synthesis resulting in sarcopenia [2]. It is associated with higher rates of complications of cirrhosis (eg hepatic encephalopathy and infections), hospital admissions and premature mortality. In addition, it is associated with poorer clinical outcomes after liver transplantation (eg rejection, length of hospital stay and mortality), in addition to reduced quality of life and lack of functional independence [3-4].
Loss of muscle mass and function, or sarcopenia, is one of the commonest features of cirrhosis and contributes significantly to morbidity and mortality in this population. The prevalence of sarcopenia and frailty in cirrhosis ranges from 40–70% depending on the population evaluated, the methods of assessment, and the operational definitions used [5-6].
Reversal of sarcopenia in an observational cohort has been associated with improved survival, and thus it is logical to anticipate a mortality benefit if we can treat sarcopenia in cirrhosis. However, there are currently no interventions supported by randomized controlled data to increase muscle mass in this population. Himachal Pradesh is situated in the North-West of India and is mainly a hill state. Rajendra Prasad Government Medical College Hospital in district Kangra is the only major referral hospital in this part of the state catering to approximately 60% of the population of the state mainly of rural background. Most of the available literature on Cirrhosis of liver is from studies based on urban population and studies in developed countries.
Moreover, the inference from studies on western population or urban population may not be uniformly applicable to the rural setup in which our medical college is situated as also the modalities regarding disease prevention based on urban population or western population cannot be applied to rural population. Keeping these things under consideration, the present study was designed with the aim to assess the clinical profile of sarcopenia in patients of cirrhosis of liver presenting to the Department of Medicine, Dr. R.P.G Medical College Kangra at Tanda.
In this descriptive hospital-based study, 50 patients with evidence of liver cirrhosis diagnosed on history, imaging and investigations were included for a period of 12 months (Jan 2020-Dec 2020) at in Dr. Rajendra Prasad Government Medical College, Kangra at Tanda. Non-cirrhotic patients, and those who did not consent to participate in the study, were excluded.
Methodology
All consecutive patients of cirrhosis of liver willing to participate were subjected to focused history and examination. Demographic profile and detailed history were elicited. Detailed systemic examination was conducted. Patients were carefully examined to determine the etiology of the disease, complications at the time of presentation and disease prognosis. Data were recorded on a questionnaire specifically designed for this purpose. Variables were recorded, analyzed.
Each patient underwent the following laboratory analyses: full blood count; liver function tests, serum protein, serum albumin, SGPT, SGOT, direct, indirect and total bilirubin; renal function tests; blood sugar; serum electrolytes; and coagulation profile. Patients underwent laboratory test for testosterone levels.
Cross-sectional muscle area at the level of third (L3) lumbar vertebrae was measured. L3 skeletal muscle index was calculated by total L3 muscle cross sectional area divided by square of height. Sarcopenia was defined as value of ≤36.5 cm2/m2 in males and ≤30.2 cm2/m2 in females.
Statistical Analysis
Data were recorded into Microsoft® Excel workbook 2007 and exported into SPSS v21.0 (IBM, USA) for statistical analysis. Categorical data were presented as frequency and percentages. Normative quantitative data were compare using one-way ANOVA between 3 groups. p<0.05 was considered significant.
General Characteristics
In our study, we observed that 7 patients (14%) were in the age group of less than 40 years, 18 patients (36%) were in the age group of 40-50 years, 18 patients (36%) were in the age group of 51-60 years and 7 patients (14%) were more than 60. The mean age was 50.4±10.1 years. The most common symptom was abdominal distension (50%) followed by upper GI bleed (30%), altered sensorium (20%), and jaundice (10%). Majority of the patients (58%) in our study were in CTP class C, followed by 16 patients (32%) in CTP class B, and 5 patients (10%) in CTP class A (Table 1).
Table 1: General Characteristics
Parameters | Frequency | Percentage |
Age Group (Years) | ||
<40 | 7 | 14.0 |
40-50 | 18 | 36.0 |
51-60 | 18 | 36.0 |
>60 | 7 | 14.0 |
Symptoms | ||
Upper GI bleed | 15 | 30.0 |
Abdominal distension | 25 | 50.0 |
Altered sensorium | 10 | 20.0 |
Jaundice | 5 | 10.0 |
CTP class |
|
|
A | 5 | 10.0 |
B | 16 | 32.0 |
C | 29 | 58.0 |
Skeletal Mass Index
In this study, 66% of the patients had low skeletal mass index (Figure 1). Relation between CTP score and skeletal mass index.
In our study, SMI was not associated with CTP class as shown in Table 2.
Table 2: Relation between CTP Class vs Testosterone
CTP class | Testosterone | p-value |
A | 37.2±5.1 | 0.463 |
B | 38.1±5.8 | |
C | 39.2±5.5 |
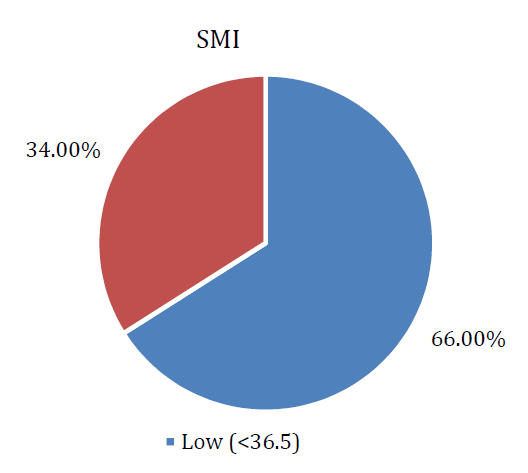
Figure 1: Skeletal Mass Index
In our study, we observed that 7 patients (14%) were in the age group of less than 40 years, 18 patients (36%) were in the age group of 40-50 years,18 patients (36%) were in the age group of 51-60 years and 7 patients (14%) were more than 60 years. In a study by Kundal et al, maximum patients were in the age group of 45-51 years (n=47;31.33%) [7]. In a multicentric study by Mukherjee et al, median age of the patients with liver disease was 43 years [8].
Majority of the patients (58%) in our study were in CTP class C, followed by 16 patients (32%) in CTP class B, and 5 patients (10%) in CTP class A. In a study of 91 patients, Pal et al found 51% of patients belonged to Child-Pugh Class B followed by Class C in 35% and only 14% in class A [9]. Soni et al reported that majority patients (77.8%) belonged to CTP Class C [10].
In our study, 33 patients (66%) had lower skeletal mass index. Kumar et al reported sarcopenia in 47.8% of patients [11]. Benzamin et al reported that sarcopenia was found in 12.8% of ALD patients (n = 148) [12]. Naseer et al in a systemic review reported that 30%-70% of the liver cirrhosis have sarcopenia [13].
In conclusion, cirrhotic population have a higher incidence of low skeletal mass in this region. Management should be tailored to the patient’s specific requirements and focus on high protein intake, regular mealtimes (including night-time snack), combination exercises, psychological support and optimisation of the underlying liver disease (ie ammonia-lowering therapy).
Carey, E.J. et al. “A North American expert opinion statement on sarcopenia in liver transplantation.” Hepatology, vol. 70, 2019, pp. 1816–1829.
Dasarathy, S. and Merli, M. “Sarcopenia from mechanism to diagnosis and treatment in liver disease.” Journal of Hepatology, vol. 65, 2016, pp. 1232–1244.
Ooi, P.H. et al. “Sarcopenia in chronic liver disease: impact on outcomes.” Liver Transplantation, vol. 25, 2019, pp. 1422–1438.
Montano-Loza, A.J. et al. “Inclusion of sarcopenia within MELD (MELD-sarcopenia) and the prediction of mortality in patients with cirrhosis.” Clinical and Translational Gastroenterology, vol. 6, 2015, article e102.
Kim, H.Y. and Jang, J.W. “Sarcopenia in the prognosis of cirrhosis: going beyond the MELD score.” World Journal of Gastroenterology, vol. 21, no. 25, 2015, pp. 7637–7647.
Montano-Loza, A.J. et al. “Inclusion of sarcopenia within MELD (MELD-sarcopenia) and the prediction of mortality in patients with cirrhosis.” Clinical and Translational Gastroenterology, vol. 6, no. 7, 2015, article e102.
Kundal, V. et al. “Chronic liver disease: etiological spectrum in adults.” JK Science, vol. 19, no. 3, 2017, pp. 145–149.
Mukherjee, P.S. et al. “Etiology and mode of presentation of chronic liver diseases in India: a multicentric study.” PLOS One, vol. 12, no. 10, 2017, article e0187033.
Pal, J. et al. “Clinical profile of chronic liver diseases in a tertiary care center in Kolkata.” Journal of the Association of Physicians of India, vol. 51, 2003, pp. 1173–1174.
Soni, A. et al. “Spectrum of hepatic encephalopathy admitted in a tertiary care center.” Indian Journal of Medical Sciences, vol. 72, no. 3, 2020, pp. 206–210.
Kumar, V. et al. “Sarcopenia in cirrhosis: fallout on liver transplantation.” Journal of Clinical and Experimental Hepatology, vol. 10, no. 5, 2020, pp. 467–476.
Benjamin, J. et al. “Characterization of body composition and definition of sarcopenia in patients with alcoholic cirrhosis: a computed tomography-based study.” Liver International, vol. 37, no. 11, 2017, pp. 1668–1674.
Naseer, M. et al. “Interventions to improve sarcopenia in cirrhosis: a systematic review.” World Journal of Clinical Cases, vol. 7, no. 2, 2019, pp. 156–170.
