+91 6002993949
submission@iarconsortium.org
Open Access
ISSN (Print) : 2709-3247
ISSN (Online) : 2709-3255
Background: Hypospadias is a common congenital abnormality, affecting approximately 0.3-0.8% of male live births. While one-stage repair of hypospadias has gained popularity, it is not without limitations. The two-stage Bracka's method, on the other hand, offers a unique combination of versatility, reliability, and refinement, making it suitable for a wide range of proximal hypospadias deformities, whether for primary repair in a child or salvage surgery in an adult. Purpose: The purpose of this study is to evaluate the effectiveness of the two-stage Bracka’s procedure for repairing proximal hypospadias, with a focus on the use of oral mucosa graft. Methods: Between May 2011 and April 2012, 13 patients with proximal hypospadias underwent the two-stage Bracka’s procedure. The first stage involved correcting chordee, excising the urethral plate (in cases of fibrous unhealthy skin, such as re-operative cases), splitting the glans, and using an oral mucosa graft to cover the ventral defect. The second stage of the surgery included neourethra formation from the grafted ventral area, utilizing dartos fascia as an intermediate protective layer, and applying the Z-plasty technique for outer skin closure. Patient ages ranged from 15 months to 15 years, with a mean age of 5.5 years. The interval between the two stages was 4-6 months, and follow-up occurred 2-6 months after the second stage. Results: In the first stage, all 13 patients underwent the operation, while 10 patients proceeded to the second stage. One patient required a revision of the first stage due to residual chordee. Among the 10 patients involved in the second stage, three developed fistulas, but no residual chordee was observed. None of the patients developed meatal stenosis, and 70% achieved a vertical slit-like meatus in the glans. Conclusions: The use of an oral mucosa graft proved effective in preventing significant graft contracture, resulting in a more supple and predictable size for the neo-urethra in the second stage surgery. The incorporation of dartos fascia and the Z-plasty technique in the second stage contributed to increased success rates and decreased complications in proximal hypospadias repair.
Hypospadias is a congenital penile defect in which the urethra opens onto the ventral part of the penis, scrotum, or perineum, hypo = below + spad = to draw off (the urine) .It is the result of incomplete development of the urethra, which occurs in 0.3–0.8% of male newborns. In this deformity, the incompletely formed corpus spongiosum extends alongside the urethral plate and reaches the open glans wings [1]. Hypospadias may be an isolated defect or a phenotypical component of a more complex condition such as an intersex state [2]. Common associated anomalies include incomplete foreskin with ventral preputial skin defect [3], resulting in a typical “hooded” appearance that calls attention to the defect during newborn examination (in nearly all cases)[4], ventral penile curvature, and deficient corporus spongiosum [3-6]. In approximately 15% of distal cases there will also be ventral curvature of the penis during erection that may indicate relative shortening of the ventral shaft skin, corpus spongiosum, and/or corpus cavernosa, Over 50% of boys with proximal hypospadias have ventral penile curvature after the shaft skin is released. Traditionally this bending was referred to as “chordee” and thought to result from dysgenic dartos fascia, Buck’s fascia, and corpus spongiosum on the ventral shaft. Straightening involves excision of these tissues, including those now recognized as the urethral plate [7-8]. Other associated anomalies that could be found with hypospadias include paraurethral sinus, flattened glans, and urethral valves [9-11]. The urethral valves found at the distal prostatic urethra.
These valves are mucosal folds that look like thin membranes; they may cause varying degrees of obstruction when the child attempts to void [6]. 9% of the patients also have inguinal hernias and another 9% may have undescended testes [7]. The goal of hypospadias surgery is to restore the urethral meatus to its normal position on the glans, to correct penile curvature and create a urethra that allows urination with a controlled stream. These goals must be accomplished with attention to cosmesis. Results of hypospadias surgery can be analyzed by both subjective and objective criteria. Objective criteria include functional status as measured by uroflow. Subjective criteria are more difficult to define, but certainly include cosmesis, sexual function, psychosocial adjustment and body image [12-16]. The ideal time for surgery is between 3 and 18 months. The infants are amnesic of the procedure and 70 - 80 % of anomalies can be managed on an outpatient basis. In addition, it seems advantageous to complete the repair before the child is old enough to remember the anomaly or the events of the repair (i.e., before 2 years of age). It can usually be accomplished before the onset of separation anxiety, which peaks between 15 and 30 months of age. Modern anesthesia and intraoperative monitoring have made the risks of operating on infants over 60 weeks of gestational age essentially immeasurable, while improvements in instruments, sutures, urethral catheters, dressings, and optical magnification have negated the "size factor."[17-21].
Patient Selection: Between May 2011 and April 2012, a total of 13 patients with varying presentations of proximal hypospadias were included in this study. These patients were recruited from two hospitals in Baghdad, Iraq, and presented with different types of hypospadias, associated with varying degrees of chordee (penile curvature) and complications.
Surgical Technique - First Stage
Anesthesia and Positioning: All surgical procedures were carried out under general anesthesia with patients in the supine position
Preoperative Assessment: Precise assessment of the penis, urethral meatus, chordee, and glans configuration was performed to determine the extent and nature of the deformity
Surgical Steps: Surgical procedures were executed meticulously with the aid of magnification
The first stage surgery involved:
Marking the new meatus location
Making lateral incisions
Infiltration with adrenaline
Suturing of specific areas
Insertion of a Foley urethral catheter
Careful dissection and deepening of the glans
Release of chordee
Reconstruction of the urethra using an oral mucosa graft
Graft Harvesting and Configuration
The oral mucosa graft was harvested, configured, and securely attached using sutures. A tie-over dressing was applied to protect the graft. Postoperative monitoring was conducted to ensure graft viability and wound healing.
Second Stage
Interval: After an approximate interval of 4-6 months from the first stage, the second stage of the procedure was initiated
Anesthesia and Assessment: Similar to the first stage, patients were administered general anesthesia, and a comprehensive assessment was performed. This included re-evaluation of chordee and meatal dilatation as needed
Meatal Reconstruction: Meatal reconstruction was the first step in the second stage, followed by tubularization of the urethra
Skin Reconstruction: In non-circumcised patients, the skin envelope was mobilized to cover the suture line. In circumcised or re-operative cases, lateral undermining and the use of a dartos fascia flap were employed to effectively cover the suture line of the neo-urethra
Suture Closure and Drain Placement: Sutures were utilized for the final closure of the glans and penile shaft skin. A drain was introduced for postoperative drainage management
Stent Placement: An N-G tube was secured and used as a stent, which remained in place for several weeks. Calibration of the new urethra was performed for an additional 2 months
Postoperative Care
Postoperative care included the administration of antibiotics and pain management as necessary. Hospitalization typically lasted 2-3 days, after which patients were closely monitored in the outpatient clinic.
At the beginning of this work, we included 13 patients their ages ranging from 15 months to 15 years (the average was 5years and 6 months).
A number of 12 patients with severe chordee, while 1 was with mild, 2 cases (15%) in addition to the correction of the chordee was required meatatomy in the first stage due to pin- point urethral meatus, one of them was peno-scrotal and became mid-scrotal ().
During the follow up period of the 1st stages 12 case (92%) show near 100% graft take, 1 case (8%) show small hematoma end with minimal slough in the central area, whereas the hematoma drained and the small slough was debrided in the outpatient unit, then the graft show good take, this was making us increasing quilting stitches to fix the graft in the subsequent cases and had been far less troublesome. Two cases (15%) develop catheter obstruction, one of them required to replace it at the 2nd post-operative day.
In concern with the mucosal graft donor site, all the cases show good healing without complications.
Table 1: Show the Numbers and Percentages of Complications in Each Type of Hypospadias Following the 1st Stage

Table 2: Show the Numbers and Percentages of Complications in Each Type of Hypospadias after the 2nd Stage
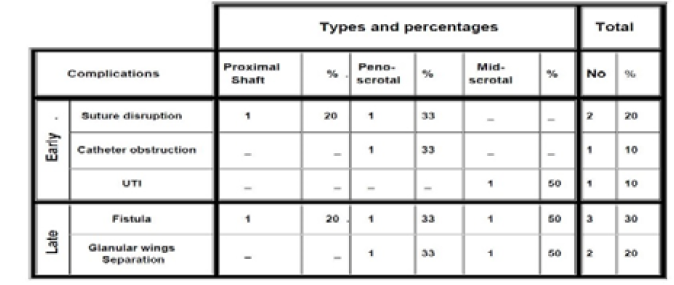
Table 3: Post-Operative Fistulae; Number, Percentage, Site, and Size in Each Type
Figure 1: 8.5 years old child, circumcised mid-scrotal hypospadias, a. shows the mild chordee, b. the abnormal (midscrotal) meatal site, c. 1.st stage; the marking of the fibrosed urethral plate excision, and glans cleftting, d. 1.st stage; the chordee excision and the wide area to be resurfaced by oral mucosa graft
Figure 2: Same child in figure 11: a. Showing the marking of harvesting oral mucosa graft, about 1 cm below the site of parotid duct, b. The size of the graft, c. Multiple quilting stitches, d. Tie-over dressing
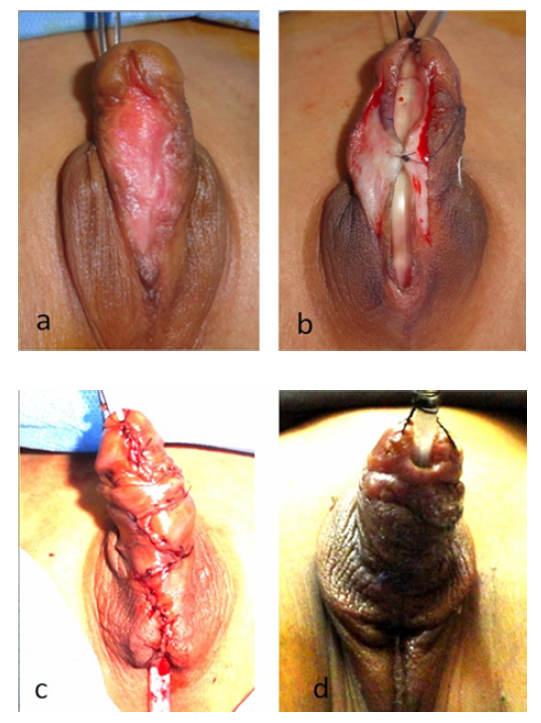
Figure 3: The 2nd Stage Steps; A. Show the Quality of the Graft after 5 Months, From The1.St Stage, B. The Formation of the Neo-Urethra by U-Shape Incision, C. The Outer Skin Closure by 4-Flap Z-Plasty, D. 3 Wks after Second Stage
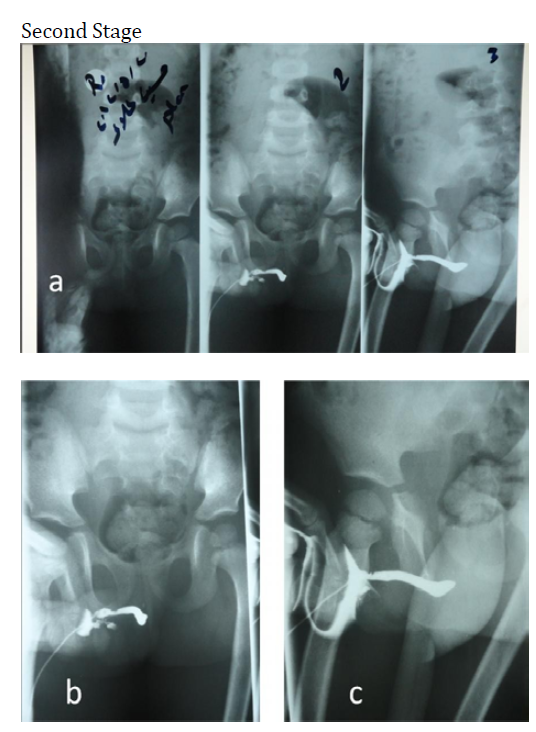
Figure 4: Retrograde urethrogram 2 months after the 2nd stage. The 3 steps of the urethrogram, b. The contrast injected through the catheter and pass in the neo-urethra, c. No stenosis at the site of the abnormal (previous) meatus, no diverticulum, and symmetrical caliber urethra
In addition, there were 12 cases (92%) show no residual chordee, while 1 case (8%) with mild to moderate residual chordee, this case already had extensive chordee and penoscrotal type.
The second stage had been carried out after 4 or 5 months in most of the cases, only two cases were managed after 6 months, and another one after 8 months (due to misunderstanding of his family).
One-stage repair of hypospadias is currently fashionable and is undoubtedly attractive in concept but the methods that are presently available all have inherent limitations and drawbacks [22]. Children operated with single-stage tubed flap repairs such as the Broadbent and Mustarde techniques during the 1960s and 1970s, were found to have had a more than 90% complication rate at adult review [24].
The two-stage Bracka method offers a unique combination of versatility, reliability and refinement, and can be used for almost any hypospadias deformity, be it primary repair in a child or salvage surgery in an adult [22].
From the vast armamentarium of hypospadias repairs that are still in use, Dr. Aivar Bracka suggests a simple protocol of just three closely related procedures with which we can now repair almost all hypospadias. The tubularised incised plate (TIP) repair and the 'Snodgraft' modification of the TIP principle are simple and effective one-stage solutions when partial circumference urethroplasty is required. Conversely, the Bracka's two-stage graft repair remains an ideal and versatile solution when a full circumference urethroplasty is required. It is particularly appropriate for severe primary hypospadias associated with a poor plate and marked chordee and also to replace a scarred, hairy or balanitis xerotica obliterans diseased urethra in re-operative salvage hypospadias [19]. All single stage repairs have a limited range of application and therefore to deal with the full spectrum of hypospadias one has to master a variety of quite unrelated procedures and all the decision making that goes with them. By contrast, the two- stage method deals with everything from minor coronal hypospadias, through to the most severe proximal cases, even if circumcised or has already been the victim of multiple failed repairs [22]. The deep splitting of the glans in the 1.st stage making the tubularisation of the grafted area easy and free from tension, never the less the graft can be observed in the follow up period after the 1.st stage for any residual chordee or shallow glans, a problem can be corrected by revision of the 1.st stage by another smaller graft [22].
One-stage tubes have an inherent tendency to stricture, both at the junction with the native urethra and also at the meatus which therefore often finishes up as a puckered orifice rather than a normal slit. Attempts to prevent contraction of the meatus by coring out erectile tissue or turning in triangular glans flaps will further compromise the appearance of the glans. Two-stage Bracka's repair avoids this problem, producing a natural slit-shaped terminal meatus and an overall sophistication of result which is hard to match with the one-stage techniques [22].
The use of an intermediate or interposition layer between the neourethra and the skin layer has greatly improved the results following hypospadias surgery and reduced complications [8].
The Dartos fascia contains a pair of axial vessels which form an arterial network within the fascia which forms the basis of the axial tunica Dartos flap, In an attempt to decrease the occurrence of urethro-cutaneous fistula, Dartos fascia axial flap has been utilized as a vascularized layer over the tabularized urethra [5].
During the fifties of the last century a modification of a popular procedure (Thiersch Duplay) introduced by Byars. A potential problem with this Byars repair is that the urethral suture line faces the overlying skin closure and is therefore at significant risk of fistula formation [22].
Cesil A. B in 1946 described a method to repair proximal hypospadias with the use of single Z-plasty to close the penile shaft skin to balance between the short skin of the penoscrotal junction and the redundancy of the lateral one [25].
In more proximal hypospadias where there is sever curvature, the integumental volume deficiency will be very pronounced, and closing the defect by advancement of the edges would undoubtedly be associated with excessive tension, to solve this problem a Z-plasty could be carried out.
Furthermore the incorporation of Z-plasty to close the penile shaft skin certainly will overcome the problem of longitudinal facing between urethral suture line and the overlying skin closure and is therefore the risk of fistula formation will decrease which is the main indication of our choice for Z-plasty.
Bracka A. published his study on 600 hypospadias, including all types; result in a fistula rate (5.7%), in wich about (11-12%) in the 1.st three years. (7%) stricture rate. (3.7 %) underwent revision of the first stage of their repair. (5.5%) underwent further cosmetic adjustments after completion of their repairs [22].
In our study which involve 5 cases (38%) proximal shaft , 5 cases (38%) peno- scrotal, whereas 3 cases( 23%) mid-scrotal type in the 1.st stage, and excluding one mid-scrotal , and two peno-scrotal cases from the 2.nd stage , with 2-6 months follow up period, there was 3 cases(30%) fistula all are in the earlier cases after second stage; this higher percentage perhaps due to the exclusive involvement of the proximal type, furthermore lower experience with this technique at the beginning of the study. This problem was canceled from the late 6 cases by increasing the depth of the glanular splitting in the first stage and change the site and direction of the corrugate drain from the proximal angle of the incision and longtudinal direction with the neourethral suture line to a site that pass between the two angles of the Z-plasty horizontaly.
Regarding other complications such as stricture, and meatal stenosis, in our study it is a 0%, this rate was due to the policy of our senior auther in delaying the stenting for 5-6 weeks and post-removal caliberation for another 2 months, but we need more follow up period to exclude possible future strictures.
There was 1 case (8% ) who require a revision for the 1.st stage due to mild residual chordee, which at 1.st was peno-scrotal with sever chordee. While in the follow up period of the 2.nd stage there was no residual chordee , also the technique of outer skin closure(Z-plastys) make a nice redistribution of the irregularly shaft and preputial skin , in addition to its favour of preventing facing between inner and outer suture lines. In Duckett's review of 18 patients undergoing to buccal mucosal grafting (16 tube) with 6-17 months follow up metal stenosis 28% which is 0% in our study. and fistula 6% in compare to 30% in our study .while in Woodard's review (Woodard's et al 1995) of 21 patients (proximal shaft: tubes and onlays) followed for 3-25 months whereas anastamosing stricture in 38%, and about 29% fistula rate which is approximately similar to our study[7], keeping in mind that we involve unselectively any proximal hypospadias whether operated or not.
Two cases (20%) in our study develop small distal glanular wings separation, and still they are satisfied and neglect its importance.
We agree with Aivar Bracka who state that, a further follow up is needed, as an ideal protocol should include an early evaluation within 3 months of surgery, followed by a review at 1 or 2 years, and again at 4 or 5 years [26].
The two-stage Bracka's method is an exceptionally versatile and reliable approach, suitable for addressing a wide range of proximal hypospadias deformities. This technique is valuable for both primary repairs in pediatric patients and salvage surgeries in adults. It particularly shines in cases of severe proximal hypospadias, chordee, and small phallus, as well as recurrent hypospadias with fibrous unhealthy skin. Utilizing buccal mucosa graft material offers an easily accessible and elastic substitute for urethral replacement, enhancing graft take with meticulous preparation. Deep division of the glans ensures a favorable outcome with a vertical slit-like meatus and minimal meatal stenosis. Incorporating an intermediate dartos fascia flap minimizes urethro-cutaneous fistula formation. Additionally, modifying the outer penile skin closure using Z-plasty reduces fistula rates and optimizes penile skin distribution. To further enhance results, urethral stenting for 5-6 weeks, followed by meatal dilatation for an additional 2 months, reduces the incidence of meatal stenosis and urethral strictures.
Yachya, D. Text Atlas of Penile Surgery. Informa Healthcare, 2007, pp. 4, 83–107.
Borer, J.G. and A.B. Retik. “Hypospadias.” Campbell-Walsh Urology. 9th ed., edited by A.J. Wein et al., Saunders Elsevier, 2007, pp. 3703–3744.
Canning, D., and A. Chang. “One-stage hypospadias repairs.” Textbook of Reconstructive Urologic Surgery, edited by D. Montague et al., Informa Healthcare, 2008, pp. 407–419.
Snodgrass, W.T. “Hypospadias and related conditions.” Clinical Problems in Pediatric Urology, edited by P. Godbole et al., Blackwell Publishing, 2006, pp. 40–54.
Chiu, T.W., and A. Burd, editors. Key Topics in Plastic and Reconstructive Surgery. Taylor and Francis, 2005, pp. 95–98.
Gerst, S.R., and H. Hrick. “Radiology of the urinary tract.” Smith’s General Urology. 17th ed., edited by E.A. Tanagho and J.W. McAninch, McGraw-Hill, 2008, p. 72f.
Duckett, J.W. “Hypospadias repair.” Operative Pediatric Urology. 2nd ed., edited by J.D. Frank et al., Churchill Livingstone, 2002, pp. 149–161.
Hadidi, A.T., editor. Hypospadias Surgery: Art & Science. Springer, 2009, pp. 1–2.
Robertson, C.N. “Embryology of genitalia.” Georgiade Plastic, Maxillofacial, and Reconstructive Surgery. 3rd ed., edited by G.S. Georgiade et al., Williams & Wilkins, 1996, pp. 839–844.
Mader, S.S. editor. Understanding Human Anatomy and Physiology. 5th ed., McGraw-Hill, 2004, pp. 380–381.
Laurence, S. and A. Baskin. “Hypospadias and urethral development.” The Journal of Urology, vol. 163, 2000, pp. 951–956.
Moore, K.L. et al., editors. Clinically Oriented Anatomy. 5th ed., Lippincott & Wilkins, 2006, pp. 357–467.
Glory, A.M. and B.R. McPherson, editors. Atlas of Anatomy. Thieme, 2008.
Johnny, A. et al., editors. “Surgical anatomy of the penis and erectile bodies.” Atlas of the Urologic Clinics, 2002, pp. 119–125.
Winterroth, F., editor. Use of Scanning Acoustic Microscopy to Examine and Evaluate Physical Characteristics of Mucosal Tissues. Deep Blue, 2011, pp. 23–61.
Tanagho, E.A. “Anatomy of the genitourinary tract.” Smith’s General Urology. 17th ed., edited by E.A. Tanagho and J.W. McAninch, McGraw-Hill, 2008, p. 15.
Mungadi, I.A. and V.I. Ugboko. Annals of African Medicine, vol. 8, no. 4, 2009, pp. 203–209.
(No article title provided; let me know if you want me to add it.)
Kirsch, A.J. “Hypospadias free grafts.” Operative Pediatric Urology. 2nd ed., edited by J.D. Frank et al., Churchill Livingstone, 2002, pp. 167–173.
Bracka, A. “The role of two-stage repair in modern hypospadiology.” Indian Journal of Urology, vol. 24, 2008, pp. 210–218.
Mouriquand, P. and P.Y. Mure. “Hypospadias.” Pediatric Surgery, edited by P. Puri and M. Hollwarth, Springer, 2006, pp. 529–543.
Schaeffer, C.S. and L.R. King. “Anomalies of male genitalia.” Georgiade Plastic, Maxillofacial, and Reconstructive Surgery. 3rd ed., edited by G.S. Georgiade et al., Williams & Wilkins, 1996, pp. 844–855.
Bracka, A. “A versatile two-stage hypospadias repair.” British Journal of Plastic Surgery, vol. 48, 1995, pp. 345–352.
Ramanathan, C. “Three years’ experience of hypospadias surgery: Bracka’s method.” Indian Journal of Plastic Surgery, vol. 39, 2006, pp. 130–135.
Bracka, A. “A long-term view of hypospadias.” British Journal of Plastic Surgery, vol. 42, 1989, pp. 251–255.
Hadidi, A.T. “Single-stage versus two-stage repair, Denis Browne technique.” Hypospadias Surgery: An Illustrated Guide, edited by A.T. Hadidi and A.F. Azmy, Springer, 2004, pp. 266–267.
Manzoni, G. et al. “Hypospadias surgery: When, what and by whom?” BJU International, vol. 94, no. 8, November 2004, pp. 1188–1195.
