+91 6002993949
submission@iarconsortium.org
Open Access
ISSN (Print) : 2709-3247
ISSN (Online) : 2709-3255
Introduction: The use of Central Venous Catheters (CVC) is a common practice among ill pediatric patients with most common complication being catheter-related blood stream infections. Objectives: The primary objective is to study the CVC settings in Rafic Hariri University Hospital (RHUH) including assessment of the types of CVCs used, indications and determining the complications, especially infection. Secondary objectives are to assess the factors predisposing to infections, evaluate care guidelines applied in comparison to the international guidelines and come up with proposal of improvement plan. Subjects and Methods: This is a retrospective study, at RHUH. Charts reviewed of all patients <18 years admitted to the hospital from 1-1-2016 till 31-12-2017 and had CVC insertion. The data collected included the age of patients, CVC type and complications. Data was treated using SPSS version 22. Results: One hundred three pediatric patients were included. CVCs were mainly inserted for prolonged Intravenous (IV) therapy. The most prevalent type of CVC was Umbilical Venous Catheter (UVC). The most common complication was infection 68.75%. The predictors of CVC-related infection were increased age, longer CVC duration and chemotherapy. However, the only indication that persisted as an independent predictor of infection was chemotherapy 16 times higher risk). A statistically significant correlation was set at P-value less than 0.05. Conclusion: CVCs, mainly UVC, are mainly inserted in newborns due to prolonged IV therapy with infection as main complication. Residents, Neonatal Intensive Care Unit (NICU), prolonged insertion, malignancy and older age of the population proved significant effect on increasing risk of catheter related blood stream infections.
General Overviews
The insertion of central venous catheters is an important requirement for several short and long-term treatments. The use of CVCs is a common practice among patients with critical illness [1], due to their wide application which has extended beyond the original use for IV medication administration. CVCs placement can thus be used for therapeutic interventions in inpatient or outpatient settings, as well as serving diagnostic purposes. CVCs placement remains one of the most frequently performed clinical procedures, with clinical data reporting 5 million CVCs insertion yearly in the united states alone [2]. The indications for CVCs insertion are many including infusion of medication (or chemotherapy) or hemodynamic monitoring, among others. CVCs should be restricted to the adequate indication of their use, particularly considering its inherent risks. As such, CVCs should not be placed simply because of the convenience of reduced cost. This is mainly due to the fact that CVCs insertion carries notable risks, including mechanical, infectious and thrombotic ones. In general, it seems that the most common mechanical complications remain arterial puncture, hematoma and pneumothorax [1]. In pediatric patients, the most common complication of central venous access devices was shown to be catheter-related blood stream infections [3], with thrombosis also cited as a common complication of CVC insertion in children [4]. The infectious complications of CVCs insertion can be predicted by several factors such as age [5], CVC duration [6,7], CVC indication [8], type of CVC [7,9] and exposure to intensive care units [7]. The risks imposed by CVCs insertion have spurred many preventative efforts and strategies. The latter are necessary when looking to reduce the complications related to this procedure, such as bleeding, pneumothorax, infection, thrombosis etc. As such, the clinical use of CVCs, their indication, type, epidemiology and complications will be explored in the present review.
Literature Review
Indications of CVCs Insertion: In clinical practice, patients often present with emergent or non-emergent conditions requiring medical treatment. In order to provide the latter, it is frequently necessary to obtain venous access which serves many purposes; some are diagnostic while the others are therapeutic. Venous Access: Peripheral venous access generally serves for short-term administration of medications. The procedure of CVCs insertion becomes necessary when treatment requires continuous administration. Also, the use of CVCs is particularly indicated when peripheral line insertion becomes difficult [10]. This is due to the fact that peripheral access can become limited and painful which carries notable stressors that could affect a pediatric patient’s medical condition and mental health [11]. The importance of preventing the pain and discomfort due to needle-related procedures has been recognized in clinical practice, leading to various efforts to reduce it including distraction, hypnosis, or breathing. These have been applied with various degrees of benefit in the reduction of self-reported pain after needle procedures [12].
Parenteral Nutrition
Adequate nutrition is a critical aspect of medical care for inpatients. When enteral feeding is not possible, administration of fluids and nutrients through the veins becomes necessary. This includes patients with bowel obstruction, intestinal failure or chronic idiopathic intestinal pseudo-obstruction syndrome. Other cases include children requiring treatment for dehydration and supplementation for deficiencies (enzymes, amino acids, etc). Children with metabolic disorders, the use of central vein access might be necessary to optimally administer a larger blood flow. Opting for central access as opposed to peripheral access thus limits the irritation of vessels, particularly small vessels which subsequently limits the possibility of injury due to parenteral nutrition [10,11].
Chemotherapy
Cancer is a notoriously lethal malignancy that does not spare pediatric populations. In general, the treatment of cancer requires the administration of chemotherapeutic agents. For this, central venous access is needed which makes CVCs a regular necessity. The reason for CVC use as opposed to peripherally placed catheters is the fact that chemotherapeutic agents can irritate and injure veins of a small caliber. Moreover, seeing as chemotherapy can damage soft tissue should it extravasate, peripheral catheters are avoided in such patients. Therefore, CVCs are required for the prevention of vascular endothelium damage and the safer administration of chemotherapy [10].
Hemodialysis
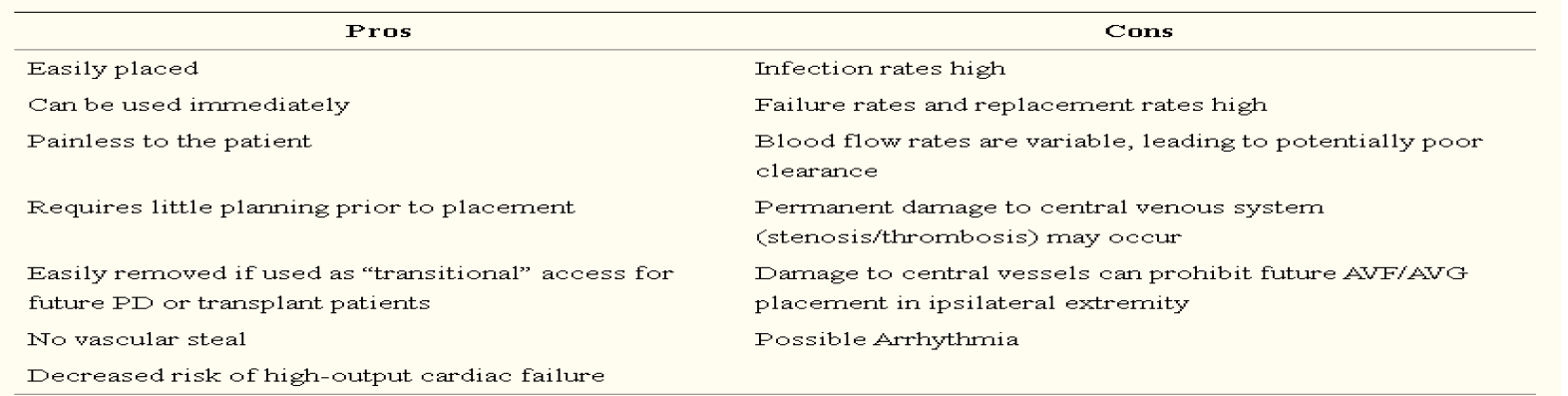
In children requiring hemodialysis, CVCs remain the most commonly used form and the first choice of vascular access. This includes children who are in need of urgent hemodialysis (stage V chronic kidney disease), as well as children set to receive a kidney transplant or peritoneal dialysis [13,14] (Table 1).
Table 1: Advantages (Pros) and Disadvantages (Cons) of CVCs for Hemodialysis in Children [13]
Blood Exchange/Apheresis
In some medical conditions, pediatric patients require blood exchange. This intervention requires central venous access in order to exchange blood components such as plasma, red blood cells, etc [10]. Therapeutic apheresis is also another indication for CVCs in children, particularly in those suffering from conditions such as Wilson’s disease, where it’s used for the reduction of copper that accumulates in the blood as a result of the autosomal recessive disorder characterizing the disease [15]. The use of total plasma exchange thus affords patients with a much-needed improvement in survival [15]. Other conditions include hereditary hemochromatosis, myasthenia gravis and sickle cell disease. For all these conditions, in addition to children with severe hemophilia, the use of CVCs becomes necessary on the long-term, even in an outpatient setting [10].
Types of CVCs
CVCs are indicated for a variety of medical conditions and diagnostic needs. As such, the type of catheter used can vary according to the duration of use, the frequency of catheter needed and which venous access sites are available for catheter insertion. CVCs can be used for short term up to two weeks, on a medium term for weeks to several months, or on the long term (for years) [16]. Central venous access falls mainly under 3 categories, namely non-tunneled, tunneled and totally implanted (Figure 1). In neonatal period, however, a 4th type exists: umbilical venous catheter.
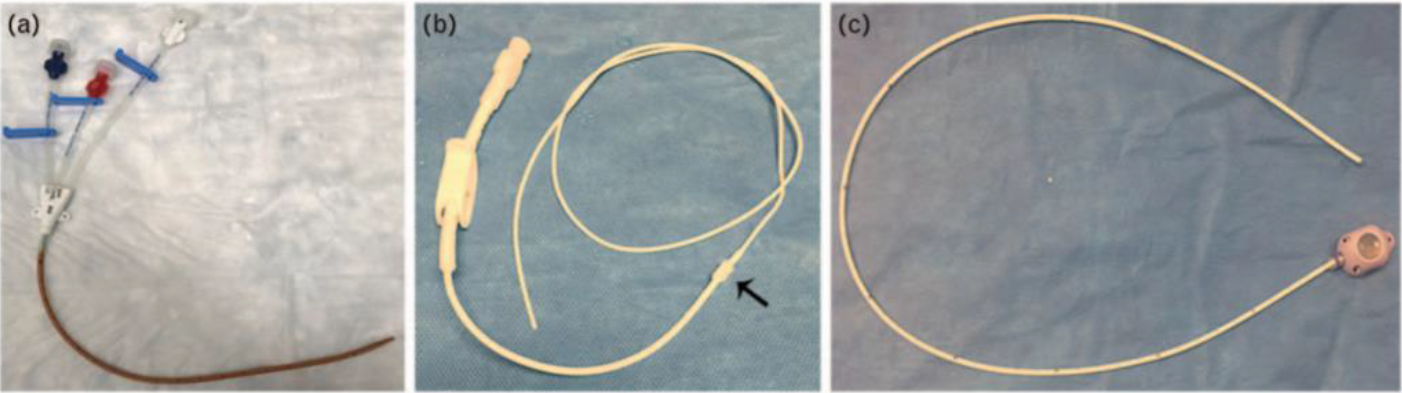
Figure 1: Commonly Used Central Venous Catheters. (a) Non-Tunneled, Triple Lumen Central Venous Catheter. (b) Broviac Catheter, a Brand of Tunneled Central Venous Catheters (c) Totally Implantable Venous Access Device (a.k.a. port) [16]
Non-Tunneled Central Catheters
In general, urgent and emergency cases require the use of percutaneous non-tunneled central catheters. They are also used in short-term CVC use (<2 weeks) or medium term (weeks-months) as shown in Figure 2. It should be noted that CVCs inserted in an emergency setting should be considered for replacement in 48 hours after the procedure due to increased risk of infection and improper settings of placement [16]. In general, this type of CVCs is advantageous in its cost-effectiveness and ease of removal by non-surgical means [2]. In order to achieve venous access, puncture is done through a needle directly in the jugular, femoral, or subclavian veins for short-term access. Peripherally Inserted Central Catheters (PICCs) however can be achieved with venous access ensured by venipuncture in the distal cephalic, basilic, or median cubital veins and are considered medium term catheters [2]. Establishing PICC lines has gained clinical use in recent years therefore decreasing the necessity of tunneled CVCs. However, both tunneled and implantable CVCs remain needed in certain clinical settings, particularly those where PICC lines could not be established or a durable long-term central venous access is needed [2] (Figure 2).
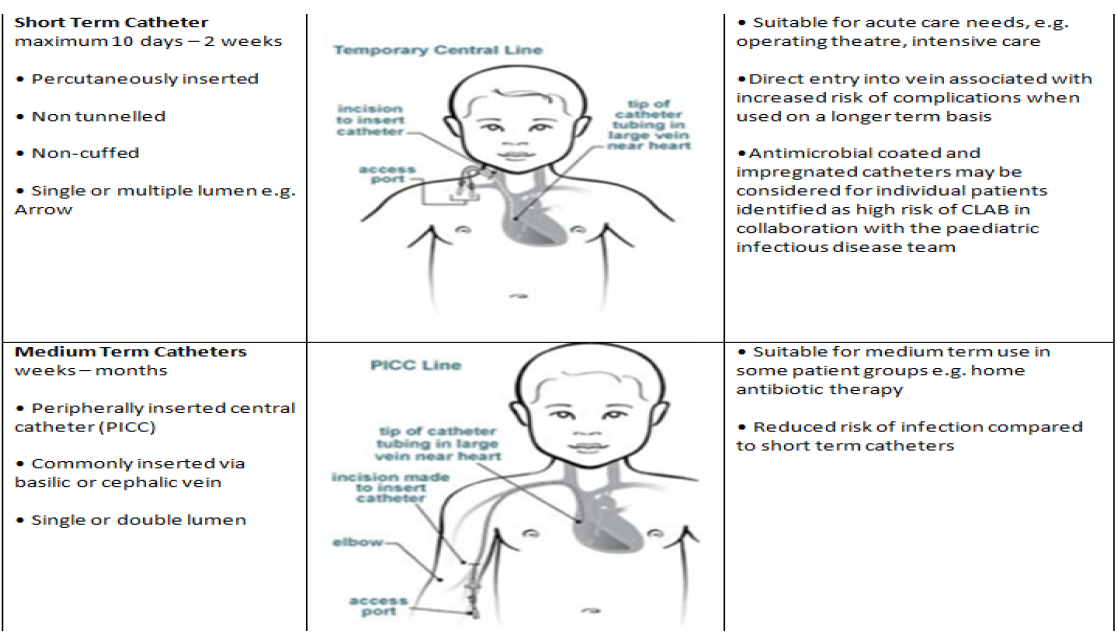
Figure 2: Examples and Characteristics of Non-Tunneled Central Catheters [2]
Tunneled Catheters
As shown in Figure 3, similar to non-tunneled catheters, tunneled catheters can be accessed by venipuncture of the subclavian, internal jugular, or femoral veins. Also, they serve for medium or long term use. For ease, a tunneled exit site is usually referred to “on the chest” or, in rare cases, “on scapula”. The tunneled exit serves as landmark for site of catheter removal. The location of the exit site varies according to child age, gross motor development and previous CVC insertion. The latter is an important consideration in order to account for previous exposure to catheterization and tugging of line that ensues from it [2]. In terms of infection rates, tunneled catheters provide an advantage to non-tunneled catheters [16]. This is due to the fact that the insertion site of tunneled catheters remains separate from the exit site and the cuff. As such, long-term catheter use generally tends to include the choice of tunneled catheters, particularly considering its convenience for both the patient and the family in terms of ease of care, lower risk of dislodgment and possibility of non-surgical repair of a ruptured line [2].
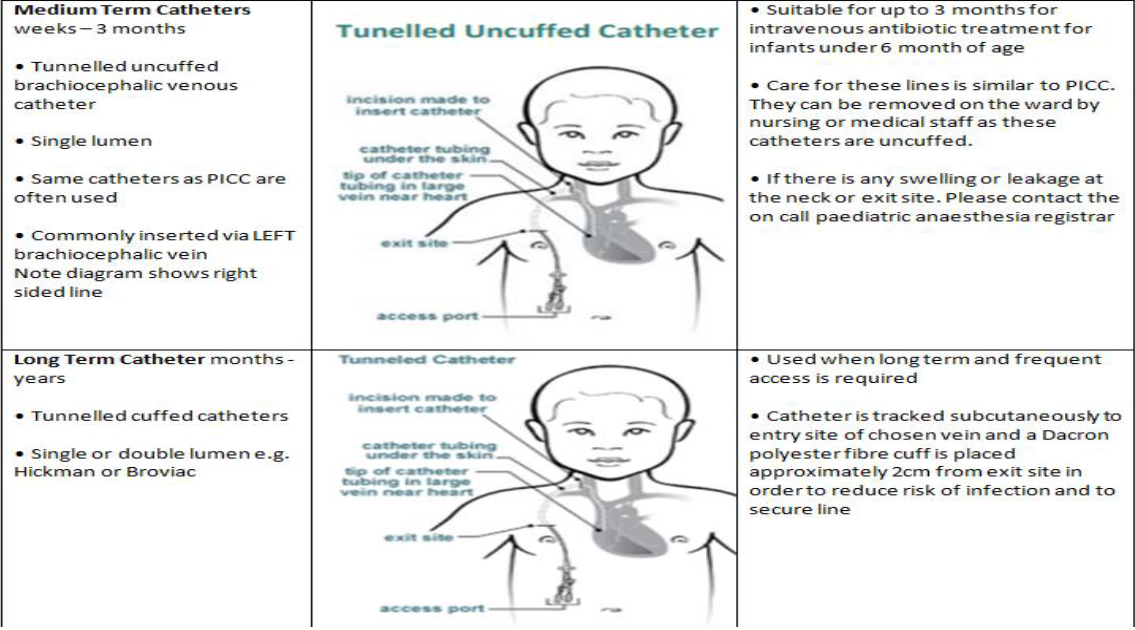
Figure 3: Examples and Characteristics of Tunneled Catheters [2]
Totally Implanted Catheters
In the case of totally implanted catheters, or ports, a percutaneous puncture of the vein is undertaken while a pocket is also created through an incision for the subcutaneous port to be held in. A non-coring needle generally serves for the access of a port. In comparison with non-tunneled and tunneled catheters, totally implanted catheters can be advantageous due to their higher durability, which allows their use for months or even years as shown in Figure 4.
Moreover, minimal body image changes are induced by totally implanted catheters which remain at a low risk of dislodgment or breakage. As for maintenance, the need for access for flushes is not very frequently observed, which increases their convenience [2,17,18]. Totally implanted catheters are generally placed on the anterior chest wall, but placement can vary according to disease, patient needs and sex with insertion into the trapezius muscle also reported [17]. Other possible insertion sites include the forearm, which was generally successful and was not associated with major complications [19].
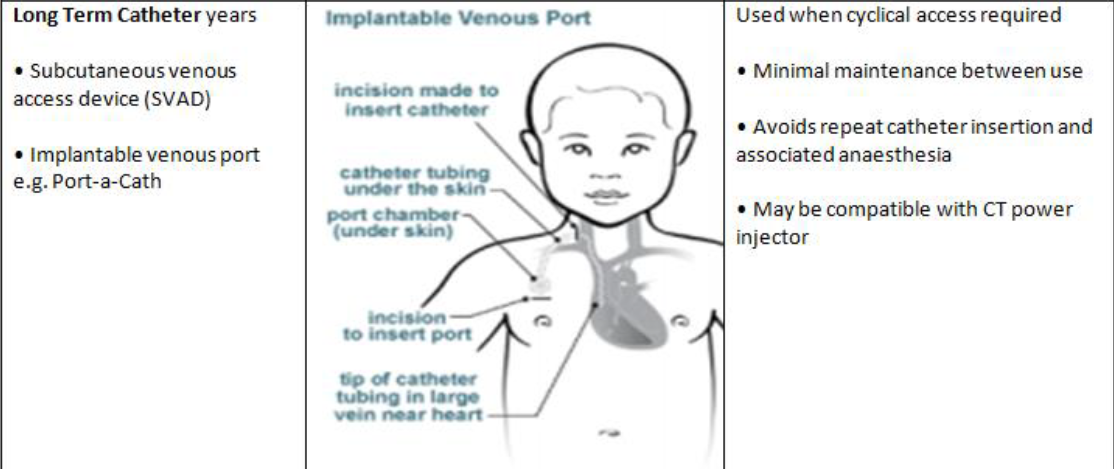
Figure 4: Example and Characteristic of Totally Implanted Catheters [2]
Umbilical Venous Catheter (UVC)
In neonates born prematurely, umbilical venous catheters are commonly used in order to account for the small caliber of their peripheral veins. This is done in order to deliver parenteral nutrition with a lower rate of infection and better weight gain when compared to delivery through peripheral lines [20]. However, correct placement of an umbilical venous catheter is critical in order to prevent malpositioning. The latter can induce severe hepatic injury, which in turn can be reflected in worse clinical outcomes on both the short- and the long-term. Furthermore, umbilical venous catheters still carry a significantly higher risk of infection, which leads to their replacement with other central access modalities if possible within one week of insertion [10].
Settings of CVCs Insertion
The placement of a CVCs can be done in several places, such as the Neonatal Intensive Care Unit (NICU), the Operating Room (OR), the Pediatric Intensive Care Unit (PICU), the delivery room or the Emergency Room (ER), depending on the circumstances of patient presentation. Considering this variability, different medical specialists should be responsible for the CVCs insertion, which includes medical residents, anesthesiologists, cardiothoracic surgeons, pediatric surgeons, neonatal intensive care fellow, or nurses [21]. Seeing as CVCs can lead to notable complications, ensuring the competence of medical professionals tasked with the placement of these catheters is critical. However, there remains a lack of standardized approach for the assessment of the competences of personnel which are sometimes required to place CVCs [22].
Complications Post CVC
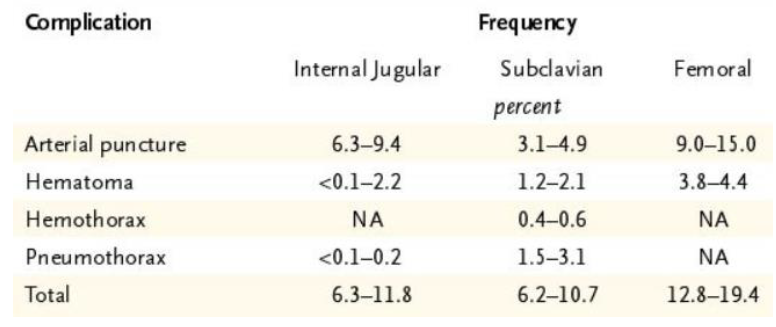
Mechanical Complications: Multiple studies have attempted to characterize the frequency of different mechanical complications arising from CVCs which are shown in Table 2. In general, it seems that the most common mechanical complications remain arterial puncture, hematoma and pneumothorax. Regardless, the rates of each mechanical complication vary according to the route of catheterization [1]. Overall, comparable rates of mechanical complications can be seen with internal jugular and subclavian venous catheterization, but they are more preferable than femoral venous insertions unless there is a contraindication to their use [1,23].
Table 2: Frequency of Mechanical Complications According to Route of Catheterization [1]
Infectious Complications
CVCs are foreign objects that are inserted into the body. They have been shown to be significantly associated with infections, particularly bloodstream infections, through multiple ways. Infection can occur on the external surface of the catheter, even at the exit site, or could occur on the internal surface (intraluminal) should the catheter hub be contaminated, or by hematogenous routes [1]. In pediatric oncology patients, the most common complication of central venous access devices was shown to be catheter-related blood stream infections [3]. Studies in children have demonstrated that CVCs carry a higher risk of infections when compared to other venous access methods. Moreover, infections led to the need to replace the catheter in approximately half of the cases [24]. Considering the effect of central-line associated infections on pediatric mortality, morbidity, complications and hospitalization, the prevention of these infections is critical in clinical practice [25].
Thrombotic Complications
Thrombosis is a complication often encountered in patients with CVCs, particularly since critical patients often suffer from conditions rendering them in a thrombophilic state [26]. Thrombosis is a common complication of CVC insertion in children [4]. Deep Vein Thrombosis (DVT) is also a relatively common complication of CVC. The risk of DVT was found to be significantly affected by several factors, among which was the presence of more than one line, as well as longer ICU stay. In other words, the longer the duration of CVCs use, the higher their risk of deep vein thrombosis. Similar associations were noted for intubation times and length of stay in the cardiac intensive care unit [27].
Bleeding Complications
The incidence of major bleeding from CVC is rare, even in patients with coagulopathy. Minor bleeding is also uncommon. Successful catheterization on the initial attempt is associated with fewer hemorrhagic complications [28,29]. Coagulopathy also was shown to not be an independent risk factor for bleeding complication at insertion of CVC [30].
Risk Factors for Catheter-Related Infection
Age: According to one major observational study performed over 20 years, several risk factors for catheter-related bloodstream infections were identified with a significant impact with infants in the NICU being at the highest risk [29]. This would suggest that younger age would suffer from a higher chance of developing bacteremia and infection. However, definitive data are still lacking and further studies addressing this topic are in need.
CVC Duration
Data indicates that umbilical vein catheters can act as vectors for the transmission of the skin bacteria into the bloodstream [31]. This is done through microfilm formation and was observed regardless of the use of antibiotics and was not affected by the duration of catheterization [31]. Strategies have been suggested to reduce the risk of infection in infants. Among them was the early (within 10 days) removal of umbilical vein catheters as opposed to leaving them for 28 days after birth. Regardless, the study failed to demonstrate a statistically significant advantage with the removal of umbilical vein catheters within 10 days of placement in terms of catheter related bloodstream infections [32]. Children who had a bloodstream infection due to catheter insertion had significantly longer pediatric ICU stays when compared to those who were not infected [7]. However, current clinical evidence remains limited, with only one study available on the subject to date. Indication: The indication for which CVCs is done could be predictive of bloodstream infections [8]. Consistently, having a malignancy, immunologic or hematologic disease was shown to significantly and independently predict central line associated bloodstream infections in children admitted to the pediatric intensive care unit [7].
Type of CVC
Concurrent use of more than one central venous catheter can lead to a higher risk of infections [9]. Central line associated bloodstream infections were more frequently reported in patients with two CVCs who were more ill compared to those with only one CVC [9]. However, evidence regarding the role of polysite or concurrent CVCs in children remains limited. On the other hand, studies have explored the implication of umbilical vein catheters in the incidence of infections in newborns with varying incidence of complications when compared to picc lines.
Location and Personnel
Child exposure to particular settings could increase their risk of developing catheter-related infections [5]. However, this association was not observed with non-infectious complications [5]. It should be mentioned that few to no studies explore the effect of who inserts a CVC on the incidence of infections. CVCs are commonly used in clinical practice across a broad range of indications. Significant factors are associated with these devices, which emphasizes the need for the establishment of risk factors and the formulation of risk mitigation and preventive strategies. Multiple characteristics such as age, admission to intensive care, increased catheterization duration, indication for CVC and the type of CVC, among others, seem to play a role in determining the risk of catheter-related infections. However, clinical evidence remains limited in certain cases, which limits the ability of clinicians to adequately address and limit catheter-related complications.
Objectives
The primary objective of our thesis was to study the central venous line settings (type, inserting personnel, location of insertion,) in one of the central hospitals in Beirut-Lebanon. Secondary objectives of the study were to: determine the most common complications of central line used, especially infection and assess the factors predicting the infection; evaluate the guidelines applied with comparison to the international guidelines; and provide suggestions (proposal plan) that can be made for improving the results.
Study Design and Population
This is a retrospective study, conducted at Rafic Hariri University Hospital (RHUH) including pediatric patients who underwent a CVC insertion during their hospitalization between January 1st 2016 and December 31st 2017. All patients who met the inclusion criteria have been included in the study. The total number of patients is 103 patients.
Inclusion Criteria
Were included in our study:
Patients with central venous catheter inserted during hospitalization in RHUH hospital in 2016 and 2017
Patients aged between 0 and 21 years
Patients of both genders (male and female)
Exclusion Criteria
Were excluded from our study:
Patients who had a fever before insertion of central venous catheter
Patients who developed a fever after one day of insertion CVC
Patients who have congenital abnormalities that increase risk of pneumothorax
Patients who have coagulation disorder
Data Collection
The data was collected from the RHUH archive department and included the following data: age; gestational age in neonates (term vs. preterm); CVC data (indication for the CVC insertion; type of CVC; location of CVC insertion (NICU, or PICU, delivery room, ER); performer of CVC insertion; cause of CVC removal; duration); and complication post CVC (infection; occlusion thrombosis; and bleeding).
CVC Insertion Protocol Used at RHUH
A protocol used at RHUH which is followed by nurses and doctors during the CVC insertion in all the patients included in the study. The protocol started by defining the CVCs as catheters inserted directly into a central vessel to provide adequate venous access and or measurement of central venous pressure (internal jugular, subclavian, femoral, humeral veins or umbilical). Careful handling of the central venous catheter should be done aided by aseptic techniques to avoid the following complications:
Mechanical Complications: Arterial puncture, hematoma and pneumothorax are the most common during the insertion of CVC
Infections Complications: Local infection or septicemia
Thrombotic Complications: The protocol included the nursing role during the CVC insertion, the CVC supervision, the CVC care and the CVC removal. A CVC Competency Validation Checklist should be filled by the nurses taking in charge the patient
Ethical Considerations
The study protocol was approved by the Institutional Review Board at RHUH (Appendix 4). The protocol was also reviewed and granted a written study approval from the research committee in the Lebanese university. This study was conducted in accordance with the US Code of Federal Regulation 45- CFR -46.107, 21-CFR-56.107, Good Clinical Practice International Conference on Harmonization Section 3 and the principles laid down by the 18th World Medical Assembly (Helsinki, 1964) and all applicable amendments. All participants had a designated code. Records will be stored and none can access the sheets except the researchers.
Statistical Analysis
Data was analyzed using the SPSS version 22. A descriptive analysis was enrolled and the variables were presented as per their type. The categorical variables were presented as frequency and proportions. The continuous variables were presented as the frequency, mean, median and standard deviation. The dependent variable is the “Infection”. The statistical correlation was tested between the CVC infection and the secondary variables. The tests used in the bivariate settings are the chi-square test and the Fisher exact test, in order to test the statistical correlation between the CVC infection and the nominal variables (preterm, type of CVC, location of CVC etc. …). In addition, the Mann-Whitney test was used in order to test the statistical correlation between the CVC infection and the continuous variables (age and duration of CVC) which are not normally distributed. Finally, a binary logistic analysis was performed in order to predict the factors affecting the CVC infection. A statistically significant correlation was set at 5% (p-value less than 0.05).
Demographic Characteristics
Our population included patients aged between 1 day and 5400 days (15 years). The mean age of the population was 447.01±1191.09 days 1.24 year and the median age was 1 day (Figure 5).
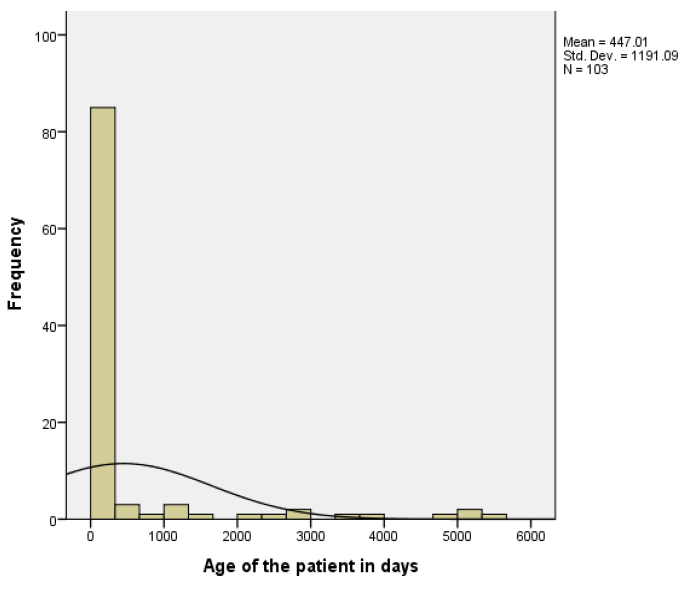
Figure 5: Age of the Patients
It was tracked in days because the data included patients from 1 day to 15 years. To note that 68% of the patients had an age of 1 day. Out of 70 neonates, 51.5% were preterm and 48.5% had a full-term gestational age (Figure 6).
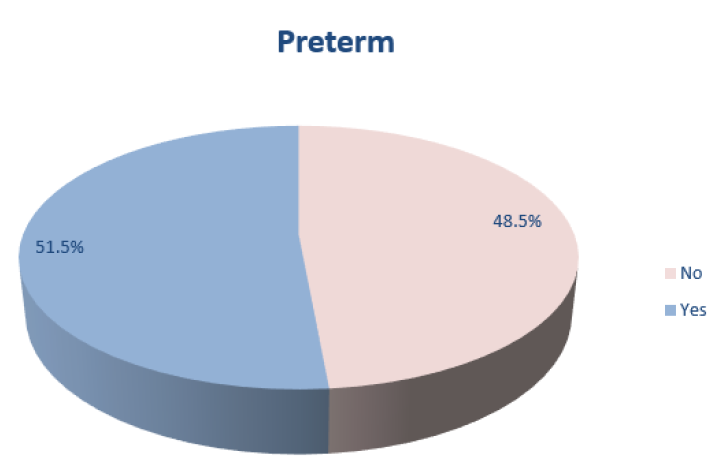
Figure 6: Percentage of CVCs Insertion in Neonates According to Gestational Age (Term Vs. Preterm)
Central Venous Line Characteristics: CVCs Indication
The prevalent indications of the central venous line insertion in the 103 patients include: prolonged IV therapy 41.7%, administration of anxious medication 30.1%, parenteral nutrition 24.3%, chemotherapy 13.6% and difficulty of peripheral line insertion 13.6% (Table 3).
Table 3: Indications of central venous line
| Indication of insertion | Frequency | % |
| Prolonged IV Therapy | 43 | 41.7 |
| Administration of Anxious Medication | 31 | 30.1 |
| Parenteral Nutrition | 25 | 24.3 |
| Chemotherapy | 14 | 13.6 |
| Difficulty of Peripheral Line Insertion | 14 | 13.6 |
| Hemodynamic Monitoring | 6 | 5.8 |
| Hemodialysis | 4 | 3.9 |
| Blood Exchange | 1 | 1.0 |
CVCs Type
The three most prevalent types of the inserted central lines were UVC 68%, Polysite 13.6% and the Broviac 7.8% (Table 4).
Table 4: Type of the Inserted Central Line
| Type of the central line | Frequency | % |
| Umbilical Line (UVC) | 70 | 68.0 |
| Implanted (Polysite) | 14 | 13.6 |
| Tunneled (Broviac ) | 8 | 7.8 |
| Non-Tunneled (Picc Line) | 6 | 5.8 |
| Non-Tunneled (Short-Term) | 5 | 4.9 |
| Total | 103 | 100.0 |
CVCs Place of Insertion
Out of 103 patients, 69.9% underwent a central line insertion at the NICU, 24.3% underwent a central line insertion at the OR and 5.8% in other departments (PICU, delivery room, ER) (Figure 5).
Table 5: Performer of the Central Line Insertion
| Performed by | Frequency | % |
| Resident | 73 | 70.9 |
| Pediatric Surgeon | 18 | 17.5 |
| Cardiothoracic Surgeon | 6 | 5.8 |
| Anesthesiologist | 3 | 2.9 |
| Fellow NICU | 3 | 2.9 |
| Total | 103 | 100.0 |
Central Line Insertion Personnel
The central line had been inserted by the resident 70.9%, pediatric surgeon 17.5%, the cardiothoracic surgeon 5.8%, anesthesiologist 2.9% and NICU fellow 2.9% (Table 6).
Table 6: Duration of the Central Line by CVC Type
| Parameter | N | Mean (days) | Std. Deviation (days) | Minimum (days) | Maximum (days) |
| Umbilical line (UVC) | 70 | 5.81 | 3.37 | 1 | 15 |
| Polysite (Implanted) | 8 | 15.00 | 7.29 | 6 | 28 |
| Tunneled (Broviac ) | 2 | 17.00 | 8.48 | 11 | 23 |
| Non-Tunneled (Picc Line) | 2 | 12.50 | 13.43 | 3 | 22 |
| Non-Tunneled (Short-Term) | 5 | 12.40 | 9.79 | 3 | 23 |
| Total | 103 | 29.36 | 84.26 | 1 | 720 |
Duration of CVC by Type
The mean duration of the central line is 29.36±84.26 days with a minimum of 1 day and a maximum of 720 days (Table 7).
Table 7: Correlation Between the CVC Infection and The Age
| Age (in Days) | N | Mean | Std. Deviation | Minimum | Maximum | p-value | |
| Infection | No | 81 | 342.23 | 1129.92 | 1 | 5040 | 0.013 |
| Yes | 22 | 832.77 | 1352.35 | 1 | 5400 | ||
Mann Whitney Test Used for These Parameters
Complications Post CVC Insertion
Out of 103 patients, 32 patients 31% underwent complications post central line insertion. The three common complications are: Infection 68.75%, occlusion/thrombosis 25% and bleeding 6.25% (Figure 7).
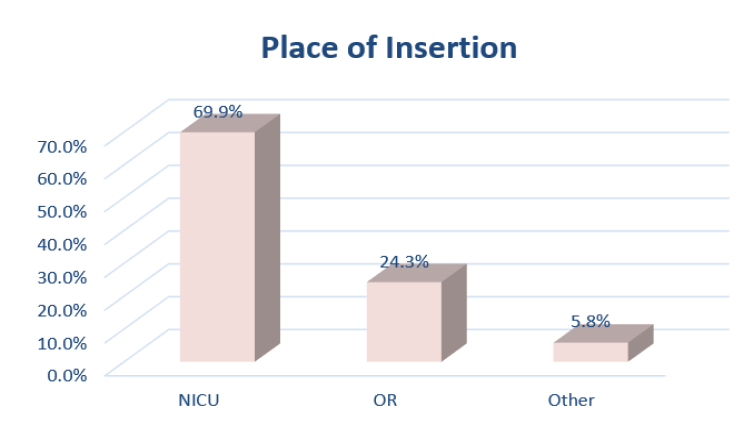
Figure 7: Place of Central Line Insertion
Factors Affecting the CVC Infection
CVC infection vs. Age: A statistically significant correlation exists between the CVC infection and the patients’ age (p-value = 0.013). The results show that the mean age of patients who underwent a central line infection (mean = 832.7±1352.35 days, 2.3 years) is higher than the mean age of patients who did not underwent a central line infection (mean = 342.2±1129.92 days, <1 year) (Table 8).
Table 8: Correlation Between the CVC Infection and the CVC Duration
| Central line duration (in days) | N | Mean | Std. Deviation | Minimum | Maximum | p-value | |
| Infection | No | 81 | 18.90 | 81.41 | 1 | 720 | 0.001 |
| Yes | 22 | 67.86 | 85.21 | 2 | 273 | ||
Mann Whitney Test Used for These Parameters
CVC Infection According to Duration of Insertion
A statistically significant correlation exists between the CVC infection and the CVC duration (p-value = 0.001). The results show that the mean central line duration of patients who underwent a central line infection (mean = 67.8±85.21 days) is higher than the mean CVC duration in patients who had no central line infection (mean = 18.9±81.41 days) (Table 9).
Table 9: Correlation Between the CVC Infection and the Preterm Status
| Parameter | Infection | OR | 95% Confidence Interval | p-value | |||
| No | Yes | Lower | Upper | ||||
| Preterm | No | 25 | 9 | 0.582 | 0.224 | 1.514 | 0.264 |
| 74% | 26% | ||||||
| Yes | 30 | 6 | |||||
| 83% | 17% | ||||||
Chi-Square Test Used for These Parameters
CVCs Infection According to Term Delivery in Neonates
No statistically significant correlation exists between the CVC infection and the preterm status (p-value>0.05) (Table 10).
Table 10: Correlation Between the CVC Infection and the CVC Insertion Indications
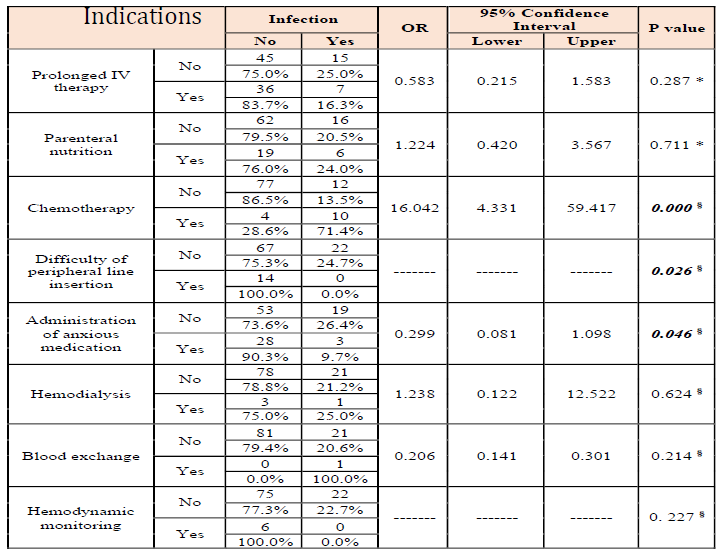
* Chi-Square Test and Fisher Exact Test used for these parameters
CVC infection According to Indication
A statistically significant correlation exists between the CVC infection and the chemotherapy indication (p-value<0.0001) (Table 11). The results show that the 71.4% of patients, who underwent a central line insertion for chemotherapy, had a CVC infection. In addition, a patient who underwent a central line insertion for chemotherapy indication has a risk of 16 times (4.331-59.417) to be infected. Furthermore, two indications for CVC insertion: difficulty of peripheral line insertion (p-value = 0.026) and administration of anxious medication (p-value = 0.046) had a significant risk for infection.
Table 11: Correlation Between the CVC Infection and the CVC Type
| Parameter | Infection | OR | 95% Confidence Interval | p-value | |||
| No | Yes | Lower | Upper | ||||
| Umbilical Line (UVC) | No | 22 | 11 | 0.373 | 0.142 | 0.982 | 0.042 * |
| 66.7% | 33.3% | ||||||
| Yes | 59 | 11 | |||||
| 84.3% | 15.7% | ||||||
| Tunneled (Broviac ) | No | 73 | 22 | ------- | ------- | ------- | 0.135 § |
| 76.8% | 23.2% | ||||||
| Yes | 8 | 0 | |||||
| 100.0% | 0.0% | ||||||
| Polysite (Implanted) | No | 77 | 12 | 16.042 | 4.331 | 59.417 | 0.000 § |
| 86.5% | 13.5% | ||||||
| Yes | 4 | 10 | |||||
| 28.6% | 71.4% | ||||||
| Non-Tunneled (Picc Line) | No | 75 | 22 | ------- | ------- | ------- | 0.227 § |
| 77.3% | 22.7% | ||||||
| Yes | 6 | 0 | |||||
| 100.0% | 0.0% | ||||||
| Non-Tunneled (Short-Term) | No | 77 | 21 | 0.917 | 0.097 | 8.643 | 0.711 § |
| 78.6% | 21.4% | ||||||
| Yes | 4 | 1 | |||||
| 80.0% | 20.0% | ||||||
* Chi-Square Test § Fisher Exact Test used for These Parameters
CVC Infection According to Type
The infection status was statistically significant with two types of CVC: the UVC (p-value = 0.042) and Polysite (p-value<0.0001) (Table 12). The results show that 15.7% of patients, who underwent an insertion of UVC, had a CVC infection. In addition, 71.4% of patients who underwent an insertion of Polysite had a CVC infection.
Table 12: Correlation Between the CVC infection and the CVC Place of Insertion
| Parameter | Infection | OR | 95% Confidence Interval | p-value | |||
| No | Yes | Lower | Upper | ||||
| NICU | No | 20 | 11 | 0.328 | 0.123 | 0.871 | 0.022 * |
| 64.5% | 35.5% | ||||||
| Yes | 61 | 11 | |||||
| 84.7% | 15.3% | ||||||
| PICU | No | 78 | 22 | ------- | ------- | ------- | 0.482 § |
| 78.0% | 22.0% | ||||||
| Yes | 3 | 0 | |||||
| 100.0% | 0.0% | ||||||
| Delivery Room | No | 79 | 22 | ------- | ------- | ------- | 0.617 § |
| 78.2% | 21.8% | ||||||
| Yes | 2 | 0 | |||||
| 100.0% | 0.0% | ||||||
| ER | No | 81 | 21 | ------- | ------- | ------- | 0.214 § |
| 79.4% | 20.6% | ||||||
| Yes | 0 | 1 | |||||
| 0.0% | 100.0% | ||||||
| OR | No | 66 | 12 | 3.667 | 1.336 | 10.060 | 0.009 * |
| 84.6% | 15.4% | ||||||
| Yes | 15 | 10 | |||||
| 60.0% | 40.0% | ||||||
* Chi-Square Test § Fisher Exact Test used for These Parameters
CVC Infection According to Insertion Place
The infection status is statistically significant with two departments where the CVC was inserted: the NICU (p-value = 0.022) and the OR (p-value = 0.009) (Table 13). The results show that 15.3% of patients, who underwent a central line insertion at the NICU, had a central line infection. In addition, 40% of patients who underwent a central line insertion at the operating theater had a central line infection.
Table 13: Correlation Between the CVC Infection and the CVC Insertion Performer
| Parameter | Infection | OR | 95% Confidence Interval | p-value | |||
| No | Yes | Lower | Upper | ||||
| Resident | No | 19 | 11 | 0.306 | 0.115 | 0.817 | 0.015 * |
| 63.3% | 36.7% | ||||||
| Yes | 62 | 11 | |||||
| 84.9% | 15.1% | ||||||
| Anesthesiologist | No | 79 | 21 | 1.881 | 0.163 | 21.758 | 0.518 § |
| 79.0% | 21.0% | ||||||
| Yes | 2 | 1 | |||||
| 66.7% | 33.3% | ||||||
| Cardiothoracic surgeon | No | 79 | 18 | 8.778 | 1.491 | 51.682 | 0.018 § |
| 81.4% | 18.6% | ||||||
| Yes | 2 | 4 | |||||
| 33.3% | 66.7% | ||||||
| Pediatric Surgeon | No | 69 | 16 | 2.156 | 0.703 | 6.614 | 0.172 * |
| 81.2% | 18.8% | ||||||
| Yes | 12 | 6 | |||||
| 66.7% | 33.3% | ||||||
| Fellow NICU | No | 78 | 22 | ------- | ------- | ------- | 0.482 § |
| 78.0% | 22.0% | ||||||
| Yes | 3 | 0 | |||||
| 100.0% | 0.0% | ||||||
* Chi-Square Test § Fisher Exact Test used for these parameters
CVC Infection According to Performer
The infection status is statistically significant with two CVC insertion performers: the resident (p-value = 0.015) and the cardiothoracic surgeon (p-value = 0.018) (Table 14). The results show that 15.1% of patients, who underwent a central line insertion via a resident, had a central line infection. In addition, 66.7% of patients who underwent a central line insertion via a cardiothoracic surgeon had a central line infection.
Table 14: Binary Logistic Analysis for the Factors Predicting the Infection
| Parameter | B | S.E. | Wald | p-value | OR | 95% Confidence Interval | |
| Lower | Upper | ||||||
| Indication of Chemotherapy | 2.775 | 0.668 | 17.256 | 0.000 | 16.042 | 1.571 | 4.524 |
| Constant | -1.859 | 0.310 | 35.875 | 0.000 | 0.156 | -2.615 | -1.346 |
Binary Logistic Analysis for the Factors Predicting the Infection
A binary logistic model was used in order to predict the factors affecting the infection. All the variables which were statistically correlated in the bivariate settings were included in the model. The results show that the “Indication of Chemotherapy” is the only factor affecting the central line infection (p-value<0.0001) with a risk OR = 16.
RHUH Characteristics and NICU as Most Common Place of CVC Insertion
One hundred and three pediatric patients with CVC insertion were retrospectively included in the study between 2016 and 2017. It’s worth mentioning that RHUH is considered as a major medical center in Beirut with a total capacity of 430 beds, 150 of which are reserved for COVID-19 ward. However, the pediatric department, mainly the hematology-oncology unit, has been suffering severely in the past few years (30 newly diagnosed cases with malignancy per year before 2015 compared to 15 cases per year after 2015). This affects the total number of cases in our study (only 103) with the majority being neonates since the number of deliveries retained its high rate with the presence of high risk pregnancies and deliveries. The factors affecting CVC-related infection will be presently discussed. According to demographic data obtained, we found that the majority of our population was newborns (Figure 6), most of them were preterm (Figure 7), which could be attributed to the importance of Obstetrics and Gynecology (OBGYN) department and the high number of deliveries per year in the studied institution. This may also be caused by the importance of our NICU that made RHUH referral hospital for high risk pregnancies and premature deliveries. This would also imply that CVCs are more frequently used around younger populations mainly newborns. It’s worth mentioning also that pre-terms had a slightly higher incidence of CVCs insertion which could be justified by the higher percentage of complications and low birth weights necessitating CVC access more urgently similar to what was shown in previous studies [33]. Furthermore, this could explain the highest percentage of UVC and polysites (Table 3) as the most prevalent types of CVCs inserted. Since most of newborns receive UVC as first-line CVC due to ease of access and short term indication to be followed by polysite if indicated, UVC was highly more frequent. Due to what was said, NICU being the most frequent place for CVCs insertion makes sense (Figure 8). These results coincide with previous studies showing newborns as the most frequent population in CVC insertion [34].
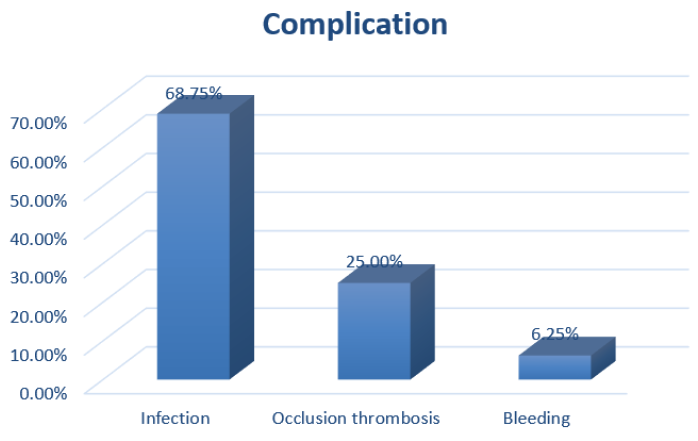
Figure 8: Complications After Central Line Insertion
Indications of CVC Insertion
As shown in Table 2, the most common indications for CVC insertion were prolonged IV therapy and Total Parenteral Nutrition (TPN) with administration of medications. These results are comparable to what was listed before, however hemodynamic monitoring through CVC insertion was not of much importance, could be due to our young population [35]. This result is interesting showing a possibility to reduce the incidence of CVC insertion through focusing on reducing IV therapy as soon as possible and focusing on other therapeutic means (non-parenteral). A worth mentioning result is that malignancy was a relatively frequent indication of CVCs insertion (polysite) for chemotherapy 13.6% as shown in Table 2 and 3, despite knowing that cancer is rare in pediatrics with a risk of any child developing cancer between birth and 20 years of age is about 1 in 300 [36]. However, among cancer patients, almost all of them need CVC.
CVC Insertion Personnel
What was interesting to obtain in Table 4, is that the resident was the most frequent performer of all CVCs insertions 70.9% despite the fact that newborns were the most studied population and the NICU fellow had a very low frequency of insertion of 2.9% only. This can be explained by the fact that RHUH is an Academic hospital affiliated with the Lebanese University (LU) and having high level of residents and fellows. One study reported that CVCs insertion by direct vein puncture was predominately done by medical residents. In the study, it was also reported that less than 15% of catheterizations were done by intensive care doctors [21].
CVC Related Risk Factors for Infections
Age: Our findings showed that increased age was a significant predictor of higher rates of CVC-related infections (p-value = 0.013) as shown in Table 6. This may be attributed to the fact that malignancy patients who received chemotherapy were of the older age groups and they had high incidence of CVC-related infections. This is inconsistent with study showing that PICC-related complications requiring the removal of the catheter increase in children less than 1-year old and decrease after 13 years of age [5]. When delving deeper into the infectious complications, it was shown that an age of 7 to 13 years old was significantly associated with less infectious complications. On the other hand, some studies report that age, gender and other demographic characteristics seemed to play no significant role in the prediction of central line associated bloodstream infections in pediatric populations [8,30]. Some other data showed that central venous catheter-related infections are common complications among children and neonates alike [25]. Its worth mentioning, however, that our population involved mainly newborns with no equal distribution according to age which might have influenced obtained results. Thus, further studies addressing this subject are needed for conclusive results.
CVC Duration
As CVC duration increases, the risk of developing a CVC-related infection increases. This was demonstrated in our study, where patients with CVC infections had a significantly longer duration of catheterization compared to those who did not (mean 67.8 days vs. 18.9 days, p = 0.001) as shown in Table 7. This was reflected in the literature, where the duration of catheterization played a complex role in the incidence of complications. In fact, it seems that catheter use for less than one week was protective against CVC-related infectious complications among children admitted to the pediatric intensive care unit [6]. Similarly, it was shown that CVC duration exceeding 7 days could independently predict central line associated bloodstream infections in the pediatric intensive care unit, with up to a 40-fold higher risk when catheters remained for 60 to 89 days [7]. CVCs have been shown to be significantly associated with infections due to their foreign aspect, particularly bloodstream infections, through multiple ways. Infection can occur on the external surface of the catheter in the event of infection of the exit site, or could occur on the internal surface (intraluminal) of the catheter should the catheter hub be contaminated, or by hematogenous routes [1]. Clinical evidence of the optimal time to remove or replace PICCs remains limited, with studies showing that the daily risk of central line associated bloodstream infections does not follow a linear relationship and can increase over time [37].
Chemotherapy
While CVCs were mainly inserted for prolonged IV therapy (41.7%) as shown in Table 2, the only factor that persisted in the multivariate model as an independent predictor of CVC-related infection was chemotherapy indication for CVC (Table 13). Our findings actually revealed that patients with a chemotherapy indication were 16 times more likely to have a CVC-related infection. In the literature, it was recognized that some conditions could predispose towards infections, particularly CVC-related infections. In one study, receiving chemotherapy 7 days prior to the insertion of a totally implantable venous access port significantly increased the risk of central line associated bloodstream infections [8]. Consistently, having a malignancy was shown to significantly and independently predict central line associated bloodstream infections in children. In fact, patients with such diseases had one-and-a-half-fold increase in the risk of central line associated bloodstream infections [7]. This could be due to the physiological state or the treatment received by patients suffering from such conditions, which could render them immunocompromised with an immature immune system. As aforementioned, the 16-fold increase might be exaggerated number because of unequal distribution of the sample.
CVC Type
The three most prevalent types of the inserted central lines in this study were the UVC 68%, Polysite 13.6% and the Broviac 7.8%. Bivariate analysis showed that patients with an umbilical vein catheter or multiple sites of CVCs were significantly more likely to have a CVC-related infection as in our study (p-value = 0.042; p-value<0.0001, respectively). Concurrent use of more than one central venous catheter can lead to a higher risk of infections which might be caused by increased illness severity in such patients [9]. One study showed that having multiple CVCs and having a Broviac CVC significantly increases the risk of central line associated bloodstream infections in the pediatric intensive care unit [7]. While this is generally consistent with our findings, a Broviac CVC was not associated with CVC-related infections in our study. On the other hand, data indicates that umbilical vein catheters can act as vectors for the transmission of the skin bacteria into the bloodstream [38]. This is done through microfilm formation and was observed regardless of the use of antibiotics and was not affected by the duration of catheterization [38]. This could account for the significant association between umbilical vein catheters and CVC-related infection observed in our study. Also, in contrast to what was previously reported that polysites have a protective effect against catheter-related blood stream infections, our study showed a significant increase in the risk of infection which may be attributed to the OR as discussed later on [34].
Location and Personnel
In this study, approximately 70% of patients underwent a central line insertion at the NICU which was inserted by the resident (Figure 8 and Table 4). Statistically, patients whose CVC was inserted in the NICU and OR had significantly higher rates of catheter-related infections (p-value = 0.022, p-value = 0.009 respectively) as shown in Table 11. This implies that the measures for keeping NICU and OR clean and sterile must be altered to target any possible pathogens. In contrast to what was previously reported, OR are no longer the most common location of CVC insertion which implies reduced burden and need of resources on hospitals and families [34]. Infections also seemed more likely to occur if the CVC was inserted by the resident (p-value = 0.015). This could suggest a deficit in expertise of CVC insertion among residents with the proper sterilization techniques and emphasize an important aspect to shed light upon in order to decrease CVC-related infections by properly educating and supervising residents’ work. Literature showed that child exposure to particular settings could increase their risk of developing catheter-related infections. This was reflected in one study, where the risk of infectious complications was significantly increased in children receiving a PICC and exposed to the neonatal intensive care unit [5]. More importantly, this association was not observed with non-infectious complications [5]. However, few to no studies explore the effect of who inserts a CVC on the incidence of infections.
Impact of the Study
This study provides important insights into the clinical aspects of CVCs among pediatric patients in Lebanon. It is the first official study about the central venous line indications, most common used type and most common complications related to it, policy followed during insertion and how to take care of it in one of the central hospitals in Lebanon. The results of this study can be used later on to evaluate the results of other studies that will be done in the same field. Moreover, the results can reflect necessary steps in order to reduce the risk of CVCs-related infections in children. Some of these steps may include proper education and supervision to resident’s work during UVC and PICC line insertion, auditing the nurses approach for providing optimum care of CVCs as documented in guidelines, avoiding keeping CVCs inserted beyond the recommended due date for removal. This can greatly improve clinical outcomes in a patient population that suffers from a high morbidity and mortality.
Limitations
The present study had multiple limitations. First, the small sample size could limit the statistical power of findings in addition to wide variation in age. Second, the distribution of included patients across age groups was not uniform, with the majority of patients were under the age of 1. Third, the study was conducted in a single center in Lebanon, which limits the generalizability of the results. Fourth, this is a retrospective study and the accuracy of the data greatly depends on the accuracy of the medical records from which it was extracted. Lastly, no sub-analysis was done according to CVCs indication and underlying diseases, which could have an influence on CVCs-related infections.
Study Perspectives
This study provides important insights into pediatric use of CVCs and infection as major complication in Lebanon. This may lead to increased antibiotic use especially with the rise of antibiotic resistance. Thus, further studies are needed in order to extensively explore the use of CVCs, existing policies, as well as the clinical profile of CVC use in different hospitals. Moreover, future studies should examine the predictors of CVC-related infections, as well as other CVC-related complications such as mechanical complications and thrombosis. Through this, the clinical outcomes of children receiving CVCs can be greatly improved in Lebanon.
The present study sheds important insights on CVC-related complications, as well as the possible predictors of CVC-related infection in pediatric patients in Lebanon. Further studies remain needed in order to explore these associations on a wider scale and formulate national preventative strategies in order to limit the burden of CVCs in pediatric populations.
McGee, D.C. and M.K. Gould. “Preventing complications of central venous catheterization.” New England Journal of Medicine, vol. 348, no. 12, 2003, pp. 1123–1133.
Duesing, L.A. et al. “Central venous access in the pediatric population with emphasis on complications and prevention strategies.” Nutrition in Clinical Practice, vol. 31, no. 4, 2016, pp. 490–501, https://doi.org/10.1177/0884533616640454.
Beck, O. et al. “Central venous access devices (CVAD) in pediatric oncology patients A single-center retrospective study over more than 9 years.” Frontiers in Pediatrics, vol. 7, 2019, article 260, https://doi.org/10.3389/fped.2019.00260.
Vidal, E. et al. “Central venous catheter-related thrombosis and thromboprophylaxis in children: A systematic review and meta-analysis.” Journal of Thrombosis and Haemostasis, vol. 12, no. 7, 2014, pp. 1096–1109, https://doi.org/10.1111/jth.12598.
Jumani, K. et al. “Risk factors for peripherally inserted central venous catheter complications in children.” JAMA Pediatrics, vol. 167, no. 5, 2013, pp. 429–435, https://doi.org/10.1001/jamapediatrics.2013.775.
Rosado, V. et al. “Incidence of infectious complications associated with central venous catheters in pediatric population.” American Journal of Infection Control, vol. 41, no. 9, 2013, pp. e81–e84, https://doi.org/10.1016/j.ajic.2012.10.024.
Woods-Hill, C.Z. et al. “Novel risk factors for central-line–associated bloodstream infections in critically ill children.” Infection Control & Hospital Epidemiology, vol. 41, no. 1, 2020, pp. 67–72, https://doi.org/10.1017/ice.2019.302.
Viana Taveira, M.R. et al. “Risk factors for central line–associated bloodstream infection in pediatric oncology patients with a totally implantable venous access port: A cohort study.” Pediatric Blood & Cancer, vol. 64, no. 2, 2017, pp. 336–342, https://doi.org/10.1002/pbc.26225.
Dube, W.C. et al. “Comparison of rates of central line–associated bloodstream infections in patients with one vs. two central venous catheters.” JAMA Network Open, vol. 3, no. 3, 2020, article e200396, https://doi.org/10.1001/jamanetworkopen.2020.0396.
Ares, G. and C.J. Hunter. “Central venous access in children: indications, devices and risks.” Current Opinion in Pediatrics, vol. 29, no. 3, 2017, pp. 340–346, https://doi.org/10.1097/MOP.0000000000000485.
Barczykowska, E. et al. “The use of central venous lines in the treatment of chronically ill children.” Advances in Clinical and Experimental Medicine, vol. 23, no. 6, 2014, pp. 1001–1009, https://doi.org/10.17219/acem/37359.
Birnie, K.A. et al. “Psychological interventions for needle-related procedural pain and distress in children and adolescents.” Cochrane Database of Systematic Reviews, vol. 10, no. 10, 2018, article CD005179, https://doi.org/10.1002/14651858.CD005179.pub4.
Chand, D.H. et al. “Hemodialysis vascular access options in pediatrics: Considerations for patients and practitioners.” Pediatric Nephrology, vol. 24, no. 6, 2009, pp. 1121–1128, https://doi.org/10.1007/s00467-008-0812-3.
Ramage, I.J. et al. “Vascular access survival in children and young adults receiving long-term hemodialysis.” American Journal of Kidney Diseases, vol. 45, no. 4, 2005, pp. 708–714, https://doi.org/10.1053/j.ajkd.2004.12.010.
Pham, H.P. et al. “Report of the ASFA apheresis registry study on wilson’s disease.” Journal of Clinical Apheresis, vol. 31, no. 1, 2016, pp. 11–15, https://doi.org/10.1002/jca.21396.
O’Grady, N.P. et al. “Guidelines for the prevention of intravascular catheter-related infections.” Clinical Infectious Diseases, vol. 52, no. 9, 2011, pp. e162–e193, https://doi.org/10.1093/cid/cir257.
Hill, S. “Totally implanted ports: The trapezius approach in practice.” British Journal of Nursing, vol. 24, no. 19, 2015, pp. S22–S26, https://doi.org/10.12968/bjon.2015.24.Sup19.S22.
Ullman, A.J. et al. “Complications of central venous access devices: A systematic review.” Pediatrics, vol. 136, no. 5, 2015, pp. e1331–e1344, https://doi.org/10.1542/peds.2015-1507.
Wildgruber, M. et al. “Short-term and long-term outcome of radiological-guided insertion of central venous access port devices implanted at the forearm.” European Radiology, vol. 25, no. 3, 2015, pp. 606–616, https://doi.org/10.1007/s00330-014-3417-1.
Shalabi, M. et al. “Risk of infection using peripherally inserted central and umbilical catheters in preterm neonates.” Pediatrics, vol. 136, no. 6, 2015, pp. 1073–1079, https://doi.org/10.1542/peds.2015-2710.
Gomes, A.V. de O. and M.A. de L. Nascimento. “Central venous catheterization in pediatric and neonatal intensive care units.” Revista da Escola de Enfermagem da USP, vol. 47, no. 4, 2013, pp. 794–800.
Boyer, D.L. et al. “Assessing competence in central venous catheter placement by pediatric critical care fellows: A national survey study.” Critical Care Medicine, vol. 47, no. 8, 2019, pp. e654–e661, https://doi.org/10.1097/CCM.0000000000003821.
Merrer, J. et al. “Complications of femoral and subclavian venous catheterization in critically ill patients: A randomized controlled trial.” JAMA, vol. 286, no. 6, 2001, pp. 700–707, https://doi.org/10.1001/jama.286.6.700.
Borzych-Duzalka, D. et al. “Vascular access choice, complications and outcomes in children on maintenance hemodialysis: Findings from the international pediatric hemodialysis network (IPHN) registry.” American Journal of Kidney Diseases, vol. 74, no. 2, 2019, pp. 193–202, https://doi.org/10.1053/j.ajkd.2019.02.014.
Chesshyre, E. et al. “The prevention, diagnosis and management of central venous line infections in children.” Journal of Infection, vol. 71, suppl. 1, 2015, pp. S59–S75, https://doi.org/10.1016/j.jinf.2015.04.029.
Jamshidi, R. “Central venous catheters: indications, techniques and complications.” Seminars in Pediatric Surgery, vol. 28, no. 1, 2019, pp. 26–32, https://doi.org/10.1053/j.sempedsurg.2019.01.005.
Steen, E.H. et al. “Central venous catheter-related deep vein thrombosis in the pediatric cardiac intensive care unit.” Journal of Surgical Research, vol. 241, 2019, pp. 149–159, https://doi.org/10.1016/j.jss.2019.03.052.
Vinson, D.R. et al. “Bleeding complications of central venous catheterization in septic patients with abnormal hemostasis.” American Journal of Emergency Medicine, vol. 32, no. 7, 2014, pp. 737–742, https://doi.org/10.1016/j.ajem.2014.03.004.
Van de Weerdt, E.K. et al. “Central venous catheter placement in coagulopathic patients: Risk factors and incidence of bleeding complications.” Transfusion, vol. 57, no. 10, 2017, pp. 2512–2525, https://doi.org/10.1111/trf.14248.
Kander, T.K. and U.S. Schött. “Bleeding complications after central line insertions and the relevance of pre-procedure coagulation tests and blood component therapy.” Critical Care, vol. 17, suppl. 2, 2013, p. P358, https://doi.org/10.1186/cc12296.
Sobczak, A. et al. “Umbilical catheters as vectors for generalized bacterial infection in premature infants regardless of antibiotic use.” Journal of Medical Microbiology, vol. 68, no. 9, 2019, pp. 1306–1313, https://doi.org/10.1099/jmm.0.001034.
Gordon, A. et al. “Early planned removal of umbilical venous catheters to prevent infection in newborn infants.” Cochrane Database of Systematic Reviews, vol. 10, no. 10, 2017, article CD012142, https://doi.org/10.1002/14651858.CD012142.pub2.
Yu, X. et al. “Risk factors related to peripherally inserted central venous catheter nonselective removal in neonates.” BioMed Research International, 2018, article 3769376, https://doi.org/10.1155/2018/3769376.
Carter, J.H. et al. “Risk factors for central venous catheter-associated bloodstream infection in pediatric patients: A cohort study.” Infection Control & Hospital Epidemiology, vol. 37, no. 8, 2016, pp. 939–945, https://doi.org/10.1017/ice.2016.83.
Pires, R.C. et al. “Central venous catheterization: An updated review of historical aspects, indications, techniques and complications.” Translational Surgery, vol. 2, 2017, pp. 66–70.
Hewitt, M. et al. Childhood Cancer Survivorship: Improving Care and Quality of Life. National Academies Press, 2003, https://doi.org/10.17226/10767.
Milstone, A.M. and A. Sengupta. “Do prolonged peripherally inserted central venous catheter dwell times increase the risk of bloodstream infection?” Infection Control & Hospital Epidemiology, vol. 31, no. 11, 2010, pp. 1184–1187, https://doi.org/10.1086/656589.
Sengupta, A. et al. “Catheter duration and risk of central line–associated bloodstream infection in neonates with PICCs.” Pediatrics, vol. 125, no. 4, 2010, pp. 648–653, https://doi.org/10.1542/peds.2009-2559.
