
+91 6002993949
submission@iarconsortium.org
Open Access
ISSN (Print) : 2789-6099
ISSN (Online) : 2789-6102
Background: Cataract remains the leading cause of preventable blindness globally, disproportionately affecting rural and underserved populations. Despite accessible surgical interventions, persistent misconceptions and limited public awareness delay diagnosis and treatment. This study evaluated public knowledge, prevalent misconceptions and healthcare-seeking behaviors related to cataracts in Himachal Pradesh, India. Material and Methods: A descriptive cross-sectional survey was conducted among 400 adults in Himachal Pradesh from October to December 2024. Convenience and purposive sampling via electronic platforms facilitated participant recruitment. A structured, bilingual questionnaire collected socio-demographic information, cataract-specific knowledge and healthcare-seeking behavior. Data were analyzed using descriptive statistics and Chi-square tests (SPSS v26.0, significance p<0.05). Results: Participants were primarily aged 26-45 years (63.8%), evenly divided by gender (51.0% female), predominantly rural residents (57.3%) and educated to at least secondary (31.8%) or undergraduate levels (33.5%). While most (79.3%) understood cataracts as lens clouding, fewer recognized the lens as the affected part (65.3%) or identified vitamin C’s preventive role (64.8%). Knowledge classification indicated 37.3% had "Very Good," 40.3% "Good," 17.3% "Fair," and 5.3% "Poor" awareness, with notable deficits among rural and less-educated groups. Conclusion: Although general awareness about cataracts in Himachal Pradesh is adequate, targeted, culturally-sensitive education and improved rural eye-care services are crucial to addressing remaining knowledge gaps and reducing preventable blindness.
Cataract remains the leading cause of visual impairment and preventable blindness globally, profoundly affecting the quality of life, particularly among aging populations. Despite significant advancements in ophthalmological treatments, including straightforward surgical interventions, cataract continues to significantly burden healthcare systems, especially in low-resource settings [1,2]. A critical yet often overlooked factor contributing to the high prevalence of cataract-induced blindness is the general public's limited understanding of the condition itself. Misconceptions, cultural beliefs, misinformation about treatment methods and the absence of accessible, accurate information collectively result in delayed diagnosis, underutilization of available healthcare resources and ultimately, preventable blindness [3-5].
In India, cataract contributes overwhelmingly to the country's burden of visual impairment, with rural populations disproportionately affected due to poor healthcare infrastructure, low literacy rates and persistent socio-economic challenges. Himachal Pradesh, a predominantly mountainous state characterized by remote and rural settlements, faces unique hurdles concerning visual healthcare. Limited healthcare facilities, challenging geographical accessibility and traditional health beliefs often merge to create barriers that prevent timely diagnosis and management of cataract cases. Consequently, residents of Himachal Pradesh, especially elderly populations in remote villages, are highly vulnerable to progressive vision loss and reduced quality of life due to untreated cataracts [6,7].
Although cataract surgeries are safe, cost-effective and widely available through public health initiatives, surgery rates remain lower than optimal due to public misconceptions and misinformation. Community misperceptions range from misunderstanding the early signs of cataracts to associating surgical procedures with unnecessary risks or expenses. The gap between cataract prevalence and surgical intervention rates underscores a critical need to evaluate public knowledge, attitudes and behaviors surrounding cataracts comprehensively [8-10].
Given these gaps, this study seeks to critically examine public awareness, common misconceptions and barriers influencing healthcare-seeking behaviors regarding cataracts among populations in Himachal Pradesh. Through identifying specific knowledge deficits and socio-cultural determinants that hinder timely intervention, the study aims to inform evidence-based, culturally sensitive educational strategies and public health policies. Improving community-level understanding of cataracts and demystifying available treatments can significantly enhance early detection, encourage acceptance of surgical interventions and ultimately reduce the unnecessary burden of cataract-related visual impairment in this geographically challenging region.
Research Design
A descriptive, cross-sectional research design was adopted to evaluate public knowledge, perceptions and healthcare-seeking behaviors regarding cataracts in Himachal Pradesh. This study employed a structured questionnaire distributed electronically to gather quantitative data from adults across diverse socio-demographic backgrounds within the state.
Study Area and Population
The study was conducted across multiple districts of Himachal Pradesh, a northern Indian state known for its diverse topography and significant rural populations. The selected districts represented varied geographical contexts, including urban, rural and remote mountainous regions, ensuring a comprehensive assessment. Participants included adults aged 18 years or older who were permanent residents of Himachal Pradesh, with an emphasis on engaging residents from rural and underserved communities where cataract awareness and healthcare access are notably limited.
Study Duration
The data collection was conducted over a period of three months, from October to December 2024. This duration provided adequate time to achieve broad geographical and demographic coverage while maximizing respondent participation and survey completeness.
Sample Size and Sampling Technique
A total of 400 participants were enrolled in the study. The sample size was determined based on a 95% confidence interval, an assumed awareness prevalence of 50% and a 5% margin of error. To accommodate potential incomplete responses, a 10% buffer was incorporated into the final sample size. Convenience and purposive sampling techniques were employed for participant recruitment. Digital outreach methods such as social media (WhatsApp, Facebook community pages) facilitated the recruitment of diverse respondents efficiently across various socio-economic strata.
Inclusion and Exclusion Criteria
Inclusion Criteria
Exclusion Criteria
Data Collection Instrument
A structured, pre-validated questionnaire was designed specifically for this study, drawing inputs from ophthalmologists, public health specialists and community healthcare providers. The questionnaire comprised three primary sections:
Healthcare-Seeking Behavior: Questions in this section assessed the respondents’ experiences and attitudes toward cataract detection and treatment, barriers encountered in accessing care, preferred sources of information regarding eye health and attitudes toward cataract surgery
The questionnaire was provided bilingually (Hindi and English) to enhance accessibility and comprehension among respondents with varying literacy levels.
Scoring and Knowledge Classification
Participants' responses in the knowledge assessment section were scored and categorized into four distinct knowledge categories to identify specific gaps clearly:
This classification facilitated the identification of vulnerable groups requiring targeted educational interventions.
Data Collection Procedure
The survey was distributed electronically using Google Forms, shared extensively through various social media platforms, including WhatsApp groups and Facebook community pages. Clear instructions accompanied each survey link, emphasizing voluntary participation and the assurance of confidentiality. Prior to responding, informed consent was explicitly obtained from each participant, ensuring ethical adherence and respondent privacy.
Data Analysis
Collected data were systematically cleaned and organized using Microsoft Excel. Statistical analyses were conducted using SPSS version 26.0. Descriptive statistics were employed to summarize socio-demographic characteristics, knowledge levels and healthcare-seeking behaviors.
Ethical Considerations
Ethical principles guided the entire study process. Participants received detailed explanations of the study's purpose, confidentiality measures, voluntary participation and their right to withdraw at any stage without consequence. Data confidentiality was rigorously maintained and collected data were used exclusively for research purposes.
A total of 400 participants were surveyed across Himachal Pradesh, with a balanced gender distribution (51.0% females, 49.0% males). Most participants were from the age group of 26-35 years (34.3%), closely followed by the 36-45 years category (29.5%), highlighting active engagement from the working-age population. Educationally, a substantial number of participants held undergraduate degrees (33.5%) or completed secondary school education (31.8%), although a smaller segment had no formal education (5.3%). Occupationally, homemakers (28.3%) and office workers (21.8%) comprised the largest groups, along with a significant proportion of retired individuals (13.3%), who are generally at higher risk for cataracts. Notably, the majority resided in rural areas (57.3%), underscoring the importance of addressing cataract awareness and healthcare accessibility specifically within these communities (Figure 1).
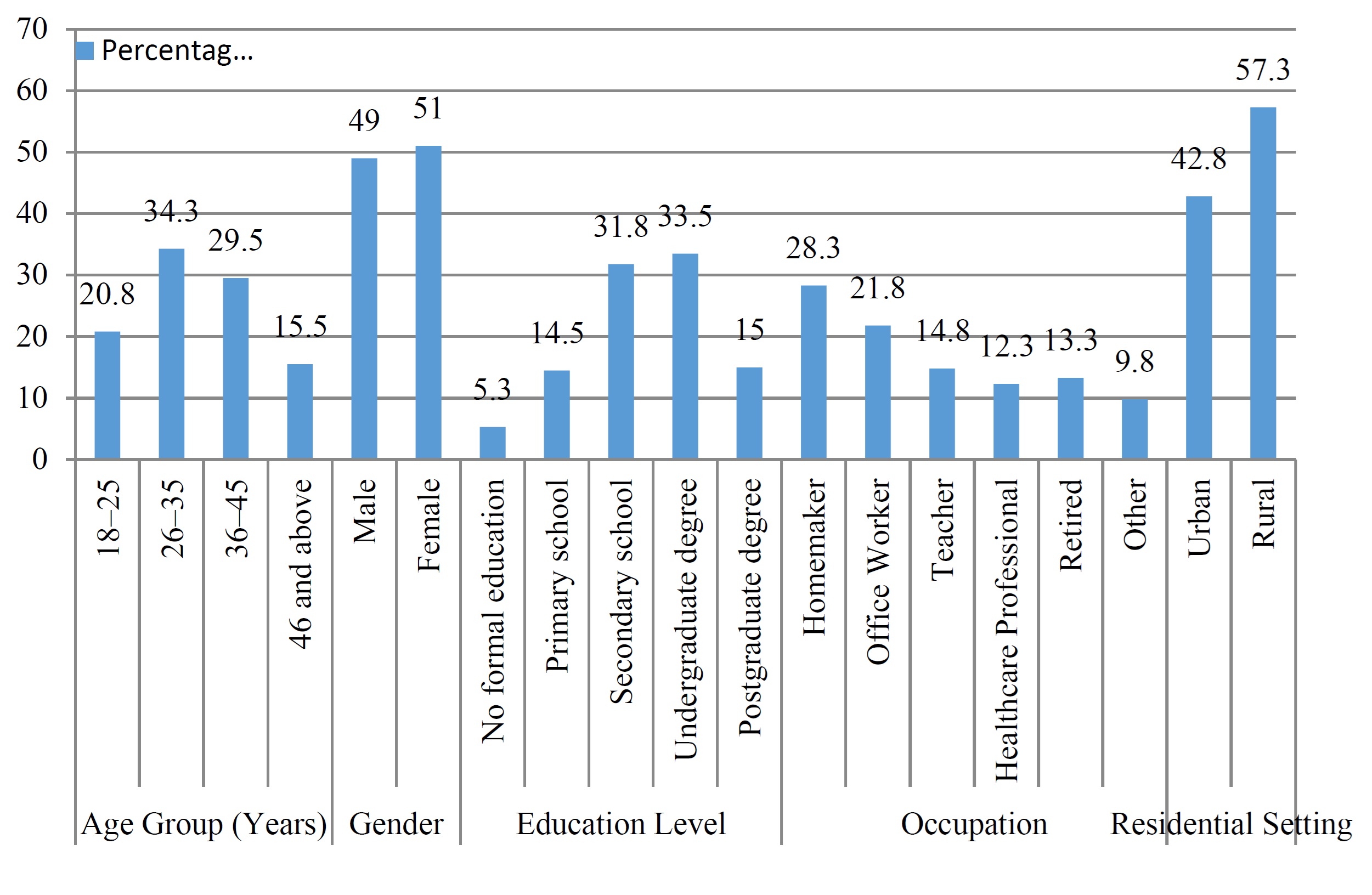
Figure 1: Socio-demographic characteristics of participants
The assessment of cataract-related knowledge indicated a moderate-to-good overall awareness among the participants. Most respondents correctly identified cataracts as clouding of the eye's lens (79.3%), acknowledged it as the leading global cause of vision loss (73.5%) and recognized surgery as the standard treatment method (72.3%). Despite this foundational understanding, several specific gaps emerged, such as limited recognition of the lens as the affected eye part (65.3%), uncertainty regarding nutritional risk factors like vitamin C deficiency (64.8%) and misconceptions about complete cataract prevention (68.5%). Awareness about symptoms requiring urgent care, such as sudden blindness in one eye (73.3%), was relatively good, yet the lower recognition of UV exposure as a risk factor (69.3%) highlights areas for targeted public health education (Table 1).
Table 1: Awareness and Knowledge of Cataracts Among the Public
No. | Question | Options | Correct Responses (n) | Percentage (%) |
1 | What is a cataract? | a) Ear blockage, b) Clouding of the eye's lens, c) Throat infection, d) Skin rash | 317 | 79.3 |
2 | What is the leading cause of vision loss worldwide? | a) Sinusitis, b) Hearing loss, c) Cataracts, d) Diabetes | 294 | 73.5 |
3 | What primarily causes cataracts? | a) Loud noises, b) Aging, c) Poor hygiene, d) Lack of sleep | 281 | 70.3 |
4 | Can cataracts be treated without surgery? | a) Yes, b) No, c) Only in early stages, d) Only with diet | 339 | 84.8 |
5 | Which nutrient helps reduce cataract risk? | a) Vitamin B12, b) Vitamin C, c) Vitamin K, d) Iron | 259 | 64.8 |
6 | What should someone do if they notice cloudy vision? | a) Ignore it, b) Visit an eye specialist, c) Use eye drops, d) Wait a month | 306 | 76.5 |
7 | What is a common symptom of cataracts? | a) Ear pain, b) Sore throat, c) Blurry vision, d) Fever | 272 | 68.0 |
8 | Which symptom requires urgent eye care? | a) Mild itching, b) Sudden blindness in one eye, c) Occasional redness, d) Tiredness | 293 | 73.3 |
9 | Can UV exposure increase cataract risk? | a) Yes, b) No, c) Only in children, d) Only at night | 277 | 69.3 |
10 | What is the most common treatment for cataracts? | a) Eye drops, b) Surgery, c) Glasses, d) Home remedies | 289 | 72.3 |
11 | What is a risk of untreated cataracts? | a) Complete vision loss, b) No risk, c) Hair loss, d) Joint pain | 266 | 66.5 |
12 | Can cataracts develop in young people? | a) Yes, b) No, c) Only after age 50, d) Only if inherited | 303 | 75.8 |
13 | How does smoking affect cataracts? | a) No effect, b) Increases risk, c) Improves vision, d) Causes ear pain | 282 | 70.5 |
14 | What part of the eye is affected by cataracts? | a) Cornea, b) Lens, c) Retina, d) Optic nerve | 261 | 65.3 |
15 | Can cataracts be prevented completely? | a) Yes, b) No, c) Only with surgery, d) Only in youth | 274 | 68.5 |
16 | What lifestyle habit reduces cataract risk? | a) Drinking soda, b) Excessive screen time, c) Wearing sunglasses, d) Ignoring mild blur | 316 | 79.0 |
17 | What is the best way to detect cataracts early? | a) Self-check, b) Regular eye exams, c) Waiting for symptoms, d) Asking family | 297 | 74.3 |
18 | Which of these is NOT a cataract symptom? | a) Cloudy vision, b) Double vision, c) Glare sensitivity, d) Ear infection | 258 | 64.5 |
19 | What is the first step if you suspect a cataract? | a) Rub eyes, b) Apply heat, c) See an eye doctor, d) Avoid bright light | 276 | 69.0 |
20 | What type of doctor treats cataracts? | a) Cardiologist, b) Neurologist, c) Ophthalmologist, d) General physician | 336 | 84.0 |
Knowledge score classification revealed an encouraging level of general cataract awareness among respondents, with the majority falling into the "Good" (40.3%) or "Very Good" (37.3%) categories. Nevertheless, a concerning proportion exhibited only "Fair" (17.3%) or "Poor" (5.3%) knowledge, reflecting critical gaps and misconceptions within segments of the population. These findings suggest an urgent need for focused educational initiatives and community-based interventions, particularly directed toward rural populations and less-educated groups, to address the identified knowledge gaps, misconceptions and barriers to healthcare access, ultimately reducing the preventable burden of cataract-induced vision loss in Himachal Pradesh (Table 2).
Table 2: Knowledge Score Classification
Knowledge Category | Score Range | Frequency (n) | Percentage (%) |
Very Good | ≥80% | 149 | 37.3 |
Good | 60%–79% | 161 | 40.3 |
Fair | 41%–59% | 69 | 17.3 |
Poor | <40% | 21 | 5.3 |
This research provides a comprehensive evaluation of public awareness, knowledge and perceptions regarding cataracts among residents of Himachal Pradesh, uncovering several critical insights essential for enhancing eye health in this geographically challenging region. While the study reveals generally positive baseline knowledge about cataracts, including recognition of the condition, common symptoms and standard treatment methods, notable gaps remain, highlighting persistent misconceptions that potentially contribute to delayed diagnoses and underutilization of available healthcare services.
The socio-demographic findings offer valuable context for understanding the awareness dynamics in Himachal Pradesh. Participation predominantly from the economically active age groups (ages 26-35 and 36-45 years) and a considerable percentage of retired respondents (13.3%) reflect that the survey captured populations most directly impacted by cataracts-either through personal risk or caregiving responsibilities. Furthermore, the gender-balanced sample enhances the representativeness of the findings, emphasizing that both men and women are engaged in discussions concerning eye health. Importantly, a higher proportion of rural respondents (57.3%) underlines specific vulnerabilities related to healthcare access and availability in rural and mountainous areas. These residents often face infrastructural and socioeconomic challenges, including limited access to specialized ophthalmological services, transportation difficulties, economic constraints and lower overall health literacy. As such, these findings call for tailored public health strategies, explicitly addressing rural barriers and delivering culturally sensitive education through community-based health programs.
Regarding specific knowledge about cataracts, the results indicate commendable foundational awareness, with most participants accurately identifying cataracts as clouding of the lens (79.3%), correctly recognizing cataracts as a leading global cause of vision impairment (73.5%) and appropriately acknowledging surgical treatment as the primary intervention (72.3%). Such fundamental knowledge implies a positive impact of existing health communication efforts. However, deeper analysis revealed critical deficits in nuanced understanding. For example, only 65.3% correctly identified the lens as the eye structure affected and just 64.8% recognized vitamin C as protective against cataract development. These gaps could significantly impact preventive behaviors, leading individuals to underestimate controllable risk factors or delay seeking early intervention, subsequently exacerbating cataract progression.
Moreover, the relatively lower understanding of certain critical risk factors-such as UV exposure (69.3%) and lifestyle-related prevention measures-highlights essential gaps in current public health messaging. These misperceptions or lack of detailed knowledge might prevent individuals from adopting protective behaviors such as wearing sunglasses or improving dietary habits, potentially increasing the prevalence and severity of cataracts in the region. The findings align with broader literature indicating that detailed understanding of specific risk factors and preventive measures significantly influences healthcare-seeking behaviors and the timely uptake of cataract surgery.
The analysis of symptom recognition and appropriate healthcare responses also provides essential insights. While participants generally recognized common cataract symptoms, such as blurred or cloudy vision (68.0%), understanding of symptoms demanding immediate medical attention, such as sudden blindness in one eye (73.3%), was higher but still suboptimal. This suggests potential delays in seeking critical ophthalmic care, underscoring the importance of targeted educational campaigns that clearly communicate symptom severity and urgency. Furthermore, participants showed moderate uncertainty regarding the preventability of cataracts, indicating confusion and misunderstanding about realistic expectations of prevention measures and underscoring a need for clearer, more precise public health communication on cataract prevention and early intervention benefits.
Knowledge classification further illuminated significant disparities within the population. Though the majority exhibited either "Very Good" or "Good" knowledge (totaling 77.6%), a substantial proportion fell into the "Fair" (17.3%) or "Poor" (5.3%) knowledge categories. Such disparities likely correlate strongly with lower educational levels, rural residency and socioeconomic constraints. Individuals in these groups are most vulnerable to developing advanced cataracts due to delayed diagnosis and treatment, highlighting the critical need for focused, culturally appropriate education and outreach initiatives. Interventions should explicitly target low-literacy populations, using easily understandable materials, visual aids and community health workers trained to communicate effectively with rural populations.
The persistent gaps identified in this study echo findings from broader national and international contexts, indicating widespread misconceptions about cataracts, surgery-related apprehensions and significant underutilization of available ophthalmological services. In Himachal Pradesh, traditional beliefs, fear of surgical complications, perceived high cost and limited access to specialist care compound these issues. Thus, public health strategies must specifically target these socio-cultural barriers, clearly addressing myths, demonstrating the safety and effectiveness of modern cataract surgery and illustrating successful patient outcomes to build trust and improve surgical uptake [11,12].
A multifaceted, integrated public health approach is critical for effectively addressing these identified challenges. Enhanced educational campaigns delivered via community meetings, local media and digital platforms could significantly elevate detailed cataract knowledge. Additionally, integrating regular vision screenings into primary health services, particularly in remote and rural settings, would facilitate early detection and timely referrals. Leveraging existing community healthcare networks, including ASHA workers and rural health centers, could also improve outreach efficacy. Such integrated strategies would collectively enhance awareness, reduce misconceptions and increase acceptance and utilization of available ophthalmic services [13-15].
This study underscores substantial foundational knowledge among Himachal Pradesh residents concerning cataracts but identifies critical knowledge gaps that need targeted interventions. Addressing these gaps through culturally sensitive education, strengthening rural health infrastructure and dispelling prevalent misconceptions will significantly enhance early diagnosis and treatment uptake, thereby reducing preventable cataract-related blindness. Future studies should evaluate the long-term effectiveness of these targeted educational initiatives and further explore socio-cultural determinants affecting cataract awareness and healthcare behaviors in this region.
This study highlights that while residents of Himachal Pradesh possess a generally good foundational understanding of cataracts, critical knowledge gaps and misconceptions persist, particularly regarding specific risk factors, preventive measures and the urgency of seeking medical care. These deficiencies are more pronounced among rural and educationally disadvantaged populations, significantly contributing to delayed interventions and increased cataract-related visual impairment. Addressing these gaps through targeted, culturally sensitive educational initiatives, community outreach and strengthened rural healthcare infrastructure is essential to enhancing early diagnosis, improving acceptance of surgical treatments and ultimately reducing the preventable burden of cataract-induced blindness across the region.
