
+91 6002993949
submission@iarconsortium.org
Open Access
ISSN (Print) : 2789-6099
ISSN (Online) : 2789-6102
Background: Congenital Blepharoptosis, a common form of ptosis, poses a substantial challenge in achieving consistent postoperative eyelid positioning. The complexity of this condition is evident in the extensive array of techniques available for its treatment, with over 100 reported approaches. Ptosis surgery primarily aims to achieve symmetrical upper eyelid elevation, addressing both functional improvement and aesthetic considerations. Objectives: This study sought to assess the effectiveness of non-absorbable monofilament nylon as a suspensory material in frontalis suspension surgery, utilizing a double rhomboid design. Patients and Methods: A total of 24 eyelids in 15 patients (comprising 8 males and 7 females), with ages ranging from 4 to 19 years, were evaluated. Nine patients presented with bilateral ptosis, while six had unilateral ptosis. All patients exhibited moderate to severe ptosis and poor levator function. The treatment approach involved tarsus to frontalis suspension using 3/0 monofilament nylon with a straight needle, following the double rhomboid design. Results: Among the 24 eyelids studied, functional outcomes with respect to postoperative upper eyelid positioning were as follows: 17 eyelids (70.8%) exhibited good results, 3 eyelids (12.5%) showed fair outcomes and 4 eyelids (16.7%) displayed poor results, indicating undercorrection or recurrence during the follow-up period. From an aesthetic standpoint, 17 eyelids (70.8%) demonstrated favorable cosmetic results, while 4 eyelids (16.7%) were rated as fair and 3 eyelids (12.5%) were categorized as poor by three independent observers. A single patient (4.17% of total eyelids) experienced stitch granuloma and no complications related to lagophthalmos, such as exposure keratitis, were observed in any patient. Conclusion: Non-absorbable monofilament polyamide sutures, such as nylon, offer a viable option as a suspension material in frontalis sling surgery. This approach yields satisfactory aesthetic outcomes, especially when combined with a double rhomboid design, demonstrating its potential as a reliable choice for treating congenital blepharoptosis.
Blepharoptosis
Describes a drooping of the upper eyelid and is developed from the Greek words Blepharon = eyelid and Ptosis = falling. The term is almost invariably abbreviated to ptosis [1]. Practically; Ptosis is defined as an abnormally low position of the upper eyelid margin, determined while the eye is looking in primary gaze [2]. The normal lid covers 1 to 2 mm of the upper limbus of the cornea [3], or lies at level midway between the superior edge of 4 mm pupil and the superior corneal limbus [4,5].
The eyelids are formed in the eighth week of gestation by folds of surface ectoderm that overgrow the eyes [6]. The levator muscle develops from the mesodermal layer and passes through similar stage of development of extra-ocular muscles. This explains the possible associated defects [7]. Anatomically, the eyelid consists of following layers, (Figure 1): An integument on the external surface, a connective tissue, orbicularis oculi muscle, the orbital septum, the levator palpebrae superioris and the sympathetically innervated Müller’s muscle, tarsal plate and the palpebral conjunctiva [8]. The Levator palpebrae superioris muscle is the main retractor of the upper eyelid; it is innervated by the superior division of the oculomotor nerve. It originates at the orbital apex; the muscular portion travel 40 mm,
Then transition to aponeurotic portion occur at Whitnall's ligament (fulcrum for levator muscle) and then it travels 14 to 20 mm before inserting on the anterior surface of the lower one half of the tarsal plate. Müller’s muscle originates in the undersurface of the levator aponeurosis. This muscle provides approximately 2 mm of elevation of the upper eyelid [9-11]. The tarsal plates are the dense cartilaginous like structures that provide vertical support and rigidity to the eyelids. The upper eyelid tarsus measures approximately 25 mm in length and 8 to 10 mm in the vertical dimension and 2 mm in depth [12]. Although the tarsus somewhat rigid, it is flexible enough to conform the shape of the globe and the cornea [13]. The conjunctiva provides the posterior layer of the eyelid [9].
Forntalis muscles is a vertically oriented extension of the galea that begin at the level of anterior hairline and extends caudally to cover almost the entire forehead, insertion is into the dermis of the forehead skin, its action is eyebrow elevation and Its supplied by frontal branch of facial nerve [14].
Most authors classify Ptosis on the basis of congenital or acquired dysfunction and pseudoptosis. Congenital ptosis can be further classified into: simple (myopathic) congenital ptosis, Blepharophimosis syndrome and Marcus Gunn’s jaw-winking syndrome. In Congenital Ptosis the underdeveloped levator muscle often functions poorly [13]. In the literature there have been publications reporting a 90% preponderance of congenital ptosis versus acquired Ptosis [15]. Simple congenital ptosis is unilateral in 69% of cases. Bilateral involvement may be symmetrical or asymmetrical in appearance [2]. Over 100 techniques for the treatment of Ptosis have been reported which illustrates that Ptosis appears difficult to treat as the postoperative eyelid position is highly unpredictable [16]. The main goal of Ptosis surgery is to obtain symmetrical elevation of upper lids and to get the best functional and aesthetic appearance [17].
Between January 2010 and March 2011, 15 patients (24 eyelids) with moderate to severe ptosis and poor levator muscle excursion underwent surgical correction using 3/0 monofilament nylon upper tarsus to frontalis suspension in Al-Wasity, Al-Shaheed Ghazii, Al-Hareri for surgical specialties and Ibn-Al Haitham hospitals. Their ages ranged between (4-19 years); the number of males was 8 while females number was 7. Bilateral ptosis observed in 9 patients (18 eyelids) while unilateral ptosis occurred in 6 patients. Except for one patient, none of the patients previously received any corrective Ptosis surgery (12.5%) of the patients had amblyopia preoperatively.
Preoperative Evaluation
An informative general history was obtained from the patient or the family regarding the age, gender, family history of Ptosis and any associated congenital anomalies and the history of other anesthetic problems and medical diseases. The ophthalmic history included the underlying cause of Ptosis, any previous eye injury, diplopia, changes of the lid level during the day. In most of the cases we consult an ophthalmologist for visual acuity assessment. Ophthalmic examination focused on determining the type of Ptosis whether mild, moderate or severe and the function of levator muscle. The assessment also includes the shape of lid contour and the presence of lid lag and lagophthalmos. Evaluating the presence of a positive Bell’s phenomenon is a prerequisite for all the surgeries. When ophthalmological examination was performed we focused on the measurement of the vertical dimension of the palpebral fissure. The lid margin-reflex distance (MRD) was measured. The severity of ptosis is then determined and patients with severe ptosis are ideal candidates for the procedure with upper eyelid margin covering more than 5 mm of the upper limbus of the cornea.
We measure the levator muscle excursion of upper lid from downward gaze to up gaze while holding the frontalis muscle action with the examiner’s thumb without bending the neck by using a transparent ruler. Spinelli’s classification of the levator function was adopted and categorized into: good, fair and poor. Next, we assess the state of skin crease by measuring the maximum distance between the eyelid margin and the dominant eyelid crease. The strength of eyelid closure was evaluated reflecting the strength of orbicularis oculi. Any patient with a history of dry eye condition is instructed to consult an ophthalmologist for tear film assessment. In the next step we measured the frontalis muscle action which represents the eyebrow excursion measured with the brow relaxed and then when rose, which should be about 10mm.The surgery is thoroughly explained for the patients or their parents including possible complications and recurrence with a proper informed consent, oral and written, obtained from the patients and/or their relatives. All the patients of this series had severe congenital ptosis with poor levator function and they have a normal corneal sensation with a normal Bell’s phenomenon.
Investigations
General investigations included hematological lab work: Blood grouping, hemoglobin level, PCV, bleeding time and clotting time, creatine phosphokinase and chest X ray. Preoperative photographs were taken for the patients.
Surgical Technique
With the patient in the upright position, the degree of Ptosis is determined and preoperative marking was done. The frontalis sling with a double rhomboid configuration (Figure 1) begins by marking seven access points, three above the eyebrow and four above the lash line; marking areas medially (point G), centrally (Point F) and laterally (Point E) at 3 mm superior to the border of the eyebrow hairs, the medial and lateral marks are set approximately in line with the medial and lateral canthi respectively, while the central mark is made in the middle of these two marks. Four upper eyelid’s marking are delineated across the tarsal plate approximately 3 mm superior to the lash line. These upper eyelid markings are designed so that the most medial (point D) and most lateral (point A) marks located on the tarsus about 5 mm from the medial and lateral ends of the eyelid respectively, while the other 2 central marks are designed so that the central medial (point C) and central lateral (point B) marks are 5 mm from (point D) and (point A) respectively, this leaves a 5 mm distance between (point B) and (point C).
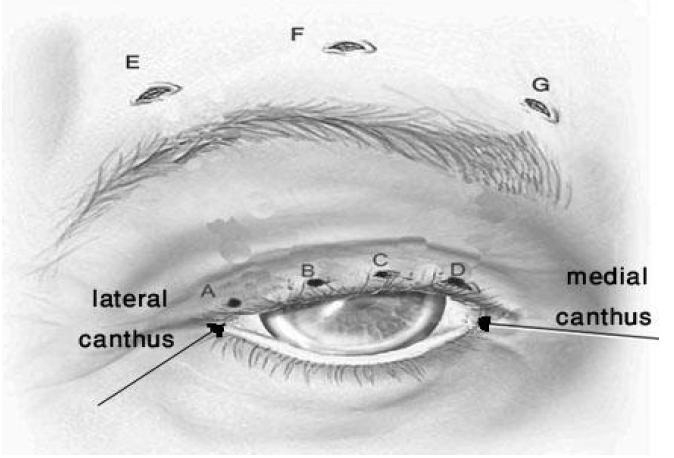
Figure 1: Double Rhomboid Marking for Frontalis Suspension
All the patients were seated in a supine position with the head and shoulders slightly elevated. General anesthesia was used in all patients. Preoperative preparation of the eyelids and brow with an iodine- based solution is routinely done. The upper eyelid was infiltrated with 1:100,000 epinephrine. 8-10 minutes is allowed to elapse for hemostasis. The globe and corneal protection with metal plate was used in all cases. Stab incisions are made above the eyebrow marks extending down to the periosteum. The medial rhomboid can be performed as shown in Figure 2.
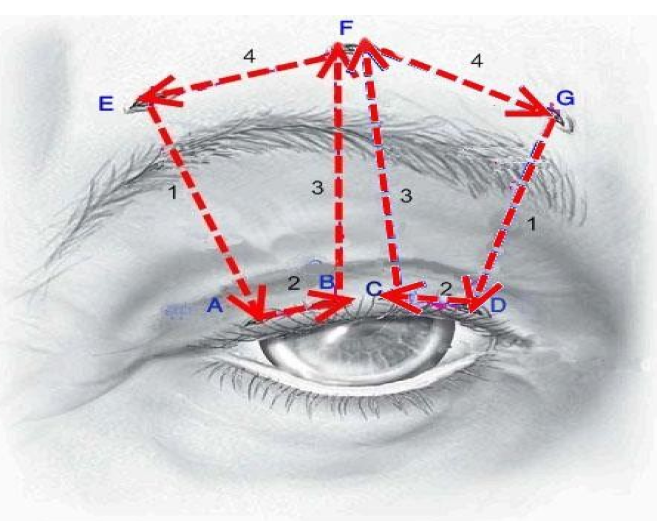
Figure 2: Configuration of Double Rhombioid
With a long (58-60mm) straight cutting needle attached to a 3-0 monofilament Nylon (MONOSOF®) or (ASSUT®) (needled suture) from the medial brow incision (point G) deep to the orbicularis muscle through the pretarsal area and exit through the most medial mark on the tarsus (point D), the needle inserted again through the same exit point on the most medial tarsus and pass horizontally to the central medial mark (point C) through the tarsus. An effort is made to engage superficial tarsus as the needle passes parallel to the lid margin.
The needle is passed again through the same mark on the central medial mark point of the tarsus and advanced towards the superior orbital rim in a sub-orbicularis muscle plain into the central stab incision above the eyebrow (Point F); the rhomboid design is completed by passing the needle deep in the frontalis muscle towards the start point at the medial eyebrow stab incision (point G). The ends of the suture are pulled up carefully to achieve the most cosmetically acceptable contour for the upper eyelid; the same sequence is applied for the lateral rhomboid. The undersurface of the upper eyelid should be everted after each move and before tying any knots on these slings to ascertain whether there is any exposure or conjunctival penetration. It is helpful to tighten the sling so that the upper lid reaches the superior limbus or the upper corneoscleral junction. Linkage is assessed by manual elevation of the eyebrow on the operated side and measurement of motility of the upper eyelid along with eyebrow elevation. The Nylon sutures are tied several times and it’s buried beneath the frontalis muscle before the skin closure was performed. Postoperative dressing in the form of broad spectrum antibiotic eye ointment is applied over the cornea and eye coverage with mild compressive dry gauze for one day; head elevation and instillation of broad spectrum antibiotic eye drops, with oral antibiotic cover.
The patient is discharged from the hospital next day and continued on an antibiotic for further 2 days and the dressing is kept for two days with antibiotic eye drops and antibiotic eye ointment such as Gentamycin 1% applied for 3 weeks, meanwhile all the patients were instructed to use artificial tears for 1 month. After 5-7 days the sutures used for skin closure is removed and the patients were advised to use the frontalis muscle to elevate the upper eyelid several times during the day.
Post-Operative Assessment
The functional and aesthetic outcome evaluation starts 1 week, 1,3,6 and 12 months later. Post-operative photographs were obtained one week and 3-9 months after the operation., The evaluation included upper eyelid level (over correction or under correction) and upper eyelid skin crease, the lagophthalmos and exposure keratitis any stitch granuloma, ectropion or hematoma.
According to Katowitz, the major criterion for a successful result was the postoperative lid level in relation to the superior limbus. Lid levels were judged good, fair and poor. A good result was defined as a postoperative lid level resting 2 to 3 mm below the superior limbus without the use of the frontalis muscle in a bilateral case, or within 1 mm of the opposite normal lid in a unilateral case. A fair result was defined as a lid level in the same position as described above with the use of the frontalis muscle required achieving this cosmetically acceptable position. A poor result was defined as a postoperative lid level 4 mm or more below the superior limbus, even with maximal use of the frontalis muscle.
Recurrences due to trauma or either a functional or cosmetic complications that required removal of the suspension suture were also recorded as poor results, regardless of the position of the lid prior to such events. The upper lid contour and cosmetic outcome was graded by three observers: the surgeon, the patient or the parents and a third observer, their observations were graded as good, fair and poor.
The preoperative waiting period for our patients ranged from five to twelve months, with an average duration of 8.73 months. All patients, except one, had not undergone any previous corrective ptosis surgery. The study identified three patients with unilateral ptosis (12.5%) and amblyopia had been diagnosed by an ophthalmologist before surgery. Based on Katowitz JA criteria, which primarily assesses eyelid function, the results were as follows: Seventeen eyelids (70.8%) showed good outcomes, three eyelids (12.5%) had fair results and four eyelids (16.7%) exhibited poor outcomes characterized by under-correction or recurrence during follow-up (Figure 3).

Figure 3: Patient No. 3 (A) Preoperative View (B) Preoperative Marking, (C, D) Postoperative Results After 4 Months
Twenty of the eyelids (83.3%) did not experience recurrence or any other complications. Among the four eyelids categorized as having poor functional results (16.7% of the total number of eyelids), either due to under-correction or recurrence, the same procedure was repeated.
No recurrence was reported after the repeated correction. In one eyelid, under-correction became apparent within the first few weeks postoperatively due to knot loosening, requiring knot retightening without repeating the entire procedure. In the other three eyelids, recurrence occurred six to nine months after the initial procedure, prompting a repetition. From an aesthetic standpoint, seventeen eyelids (70.8%) exhibited good cosmetic outcomes, while four eyelids (16.7%) showed fair results and three eyelids (12.5%) were classified as having poor cosmetic outcomes by three different observers. One patient (4.17% of the total number of eyelids) experienced stitch infection. Mild lid notching was observed in one patient but resolved spontaneously within three months. Ectropion was not observed in any patient following the procedure Table 1 displays individual patient data, Table 2 lists postoperative complications and Figures 4 to 5 illustrate some of the results.

Figure 4: Patient No. 5 (A) Preoperative View. (B, C) Postoperative View 5 Months After the Operation

Figure 5: Patient No.11 (A) Preoperative View. (B, C) Postoperative View 6 Months After the Procedure
Table 1: Patient Main Data and Results After the Follow-ups Period
Patient order | Age (year) | sex | (U)/(B) | Functional results R/L | Cosmetic outcome R/L | Other complications | Notes |
1. | 6 | ♀ | B | G/G | G/G | - | Repeated |
2. | 7 | ♂ | U | P/- | P/- | - | |
3. | 15 | ♀ | B | F/G | F/G | - | Repeated |
4. | 9 | ♂ | U | -/P | -/P | + | |
5. | 5 | ♂ | U | G/- | G/- | - | (Knot retightening) |
6. | 7 | ♀ | U | -/P | -/P | - | |
7. | 9 | ♀ | B | F/F | F/F | - | |
8. | 10 | ♂ | B | G/G | G/G | - | |
9. | 18 | ♂ | B | G/G | G/G | - | |
10. | 6 | ♀ | U | -/G | -/G | - | |
11. | 15 | ♂ | B | G/G | G/G |
| |
12. | 8 | ♀ | B | G/G | G/G | - | |
13. | 4 | ♀ | B | G/P | G/F | - | Repeated |
14. | 9 | ♂ | U | G/- | G/- | - | |
15. | 19 | ♂ | B | G/G | G/G | - |
♂: Male, ♀: Female, B: Bilateral, U: Unilateral, G: Good Result: F: Fair Result, P: Poor Result. , †: Stitch Infection as Other Complication
Table 2: Postoperative Complications and Their Percentages
Complications | No. | Percentage |
Under correction | 4 | 16.7 |
Overcorrection | 0 | 0 |
Stitch abscess/Stitch infection | 1 | 4.17 |
Lagophthalmos and Exposure keratitis | 0 | 0 |
Exposure keratitis | 0 | 0 |
Blepharoptosis is one of the most challenging and commonly encountered oculoplastic problems. It comprises various factors that have to be met to get the best result, which would depend on the nature of the ptosis, type of operation selected and the skill with which the operation is performed [6]. There is no single best method for all forms of ptosis, but most would agree that the best method would cause the least damage to the eyelid, would be easiest for the surgeon to acquire skill with and would result in the best function and appearance [22]. For any surgery in the orbital region, the primary consideration should always be the protection of the eye and maintenance of vision in addition to aesthetic consideration [7]. Frontalis suspension is a surgical procedure that is performed to address myogenic ptosis. It creates a linkage between the frontalis muscle and the tarsus of the upper eyelid, which allow for a better eyelid position in primary gaze. Eyelid elevation is then performed with the use of the frontalis muscle [26-28]. Frontalis suspension is also used in case of poor levator palpebrae superioris muscle function, neuromuscular disease and when linkage between the muscle and the eyelid is abnormal such as Marcus Gunn jaw winking phenomenon (with levator resection) [29,30].
Several surgical techniques and different sling materials may be used in frontalis suspension surgery. Materials include autogenous or banked fascia lata and alloplastic materials that include chromic gut collagen, polypropylene, silicone, stainless steel and Nylon monofilament [31], the latter was used in this study.
Our study showed that 60% of patients had bilateral ptosis and 40% had unilateral ptosis which coincides with findings of Katowitz [32], were bilateral eyelid involvement occur in (56.25%) and Ben et al. [24], were bilateral involvement occur in (55.5%). The pre-operative evaluation is the key stone in the identification of the patients who are suitable candidates for the procedure. The evaluation included the vertical height of the palpebral fissure which is the distance between the upper and lower eyelid margins, normally the distance is about 10 mm and it is useful in determining the severity of ptosis when compared to the normal eye in unilateral ptosis [1]. The evaluation of the severity of ptosis by measuring how much of the upper limbus is covered by the lid margin is used in this study. Normally the eyelid covers 1-2 mm of the upper limbus of the cornea. We have adopted Spinelli’s grading system of ptosis severity; in which the severity was regarded mild if the eyelid covers 2-3 mm of the cornea, moderate if between 3-5 mm and severe if more than 5 mm. Spinelli’s grading system of levator excursion was adopted in this study were the levator function was classified into good (10–15mm), fair (6–9mm) and poor <5mm [21]. Frontalis muscle suspensions was considered in patients with poor levator muscle excursion with moderate to severe ptosis and poor levator function, this agreed with. Katowitz [32] and Ben et al. [24]. For all the patients Bell’s phenomenon was assessed and it was present in all of them. Katowitz found that Bell’s phenomenon was abnormal in (3.13%) of his patients [32]. This might be due to the larger sample of patients which he used in his series. The timing of the surgery depends primarily on the age at presentation, The mean age of our patients was (9.73 years) compared to Ben et al. (34 years) [24] and Liu et al. (12 years) [33]. To achieve good homeostasis, Epinephrine 1: 100,000 were used as a vasoconstrictor, this agreed with Ben et al. [24]. Although it has been stated that severe blepharoptosis does not interfere with development of visual function (Benerch); Anderson Harred and Collin proved that there is correlation between the incidence of visual function impairment, development of amblyopia and the degree of ptosis [34]. Our study showed that preoperative amblyopia developed in) 12.5% (of the cases which is consistent with the findings of Carty et al., concluding that amblyopia developed in about (10%) of unilateral ptosis in his study [33]. According to our adopted criteria which depend mainly on the eyelid level; eighteen eyelids (75%) showed good result; two eyelids (8.4%) have fair results and four eyelids (16.6%) showed poor result. A retrospective study which was conducted by Ben Simon et al. at the Jules Stein Eye institute, Los Angeles, California between 1996-2002, were they reviewed the medical records of 99 patients (164 surgeries) who underwent frontalis suspension surgery for upper eyelid ptosis using different autogenousand alloplastic material [24]. One of these alloplastic materials which was used in 20 cases (12.2%) is the 3/0 Monofilament Nylon, this study showed good postoperative lid level and cosmetic outcome (75%) with the use of Nylon which is consistence with our achieved results. They used different suture designs (single loop, double pentagon), but showed no cosmetic difference, whatever suture design was use [24]. We adapted double rhomboid suture design, as it’s often advocated for optimal frontalis suspension as advised by Katowitz et al. [33]. The design is easy to perform and provides a better upper eyelid contour and is easily adjustable postoperatively as proposed by Goldberger et al. [35]. The long straight needle used in this study has the advantage of passing in a straight course in the sub-orbicularis plane and the ease of penetration directly through the tarsus and the other advantage of this needle is that the thin and flat design reduces distortion and trauma to the lid tissues with passage of the suture [33].
The essence of any ptosis surgery is a normal postoperative lid level in relation to superior limbus of cornea which was achieved in the majority of cases (75%). Also the symmetry and natural appearing cosmetic result were also adopted in evaluation of postoperative result. Mild lid notching was noticed in one patient, which was resolved spontaneously within three months which is consistent with Ben Simon et al. [24]. The recurrence rate in our study was (16.7%) of the total number of eyelids, which appeared six to nine months (average 8.73 months) after the first procedure, although the recurrence rate in Ben Simon et al. series was nearly consistence with the recurrence rate of our study (25.6%), but the follow up time of recurrence was much longer than our follow up time (up to 16.5 months postoperative). In our study less recurrence rate (16.7%) was noted compared to the publications of Wasserman et al. (69%) [36], Wagner et al. (40.5%) [11].
Ptosis recurrence is a severe problem that evolves after surgery; many investigators believe that eventually all cases of congenital ptosis that are treated with frontalis suspension will recur. this evident from a higher recurrence rate published in studies with longer follow up periods, regardless of suture material (range, 7% to 100%) [33,37]. Although in our study the recurrence rate was 16.7%, but this was during a short follow up period (4-12 months); so in case of congenital ptosis, parents and children should realize that ptosis recurrence is high after surgery and that the patient is likely to have additional surgeries. One eyelid (4.17% of total no. of the eyelids) had stitch infection, none of patients had any other complication related to exposed keratitis or corneal ulcerations or postoperative hematoma. No suture exposure was notice in our study, this agreed with Ben Simon et al. [24], were suture exposure occur in two of cases (1.2%) and Wasserman et al. [36], which occurred in one case (7.7%) and require suture removal later on.
It’s believed that suture material serves as temporary skeleton for scar formation by local inflammation. Scar tissue and not sling material may be the actual bridge between frontalis muscle and the eyelid; therefore, no difference is anticipated between different suture materials as long as they remain in good position during inflammation and scaring process although a better cosmetic outcome was noted in cases in which a nylon sling was used and despite the fact that autogenous fascia has better biocompatibility than alloplastic materials, similar function and cosmetic outcome may be achieved with alloplastic materials [24]. Thus the use of 3/0 monofilament nylon is not associated with the donor site morbidity of harvesting fascia lata. Also the decrease in the total operative time attributed to the absence of donor site incision [38].
Some of the Non-autogenous materials such as silicon rods, Mersilene and banked fascia lata had been associated with complication rates higher than suture materials. Those complications include extrusion, recurrence of ptosis and inflammation [39].
In addition to the low complication rate, the suture materials are ready available, easily introduced to the eyelid and do not carry the risk of transmitting infectious diseases. The adjustment of the eyelid level and post-operative refinement can be achieved easily with Nylon suture [36].
The old assumption regarding the high rate of infection and exposure of the nylon suture used in frontalis suspension surgery, advocating its use as a temporary measure is exaggerated
Double rhomboid design of tarsus to frontalis suspension is a very convenient method for obtaining a cosmetically acceptable contour of the upper eyelid
The follow-up period of this study was short; a longer time period is needed to assess the recurrence rate of any material used in frontalis sling surgery
Manners, R. “Ptosis.” Fundamentals of Clinical Ophthalmology: Plastic and Orbital Surgery, edited by R. Collin and G. Rose, 1st ed., BMJ Books, 2001, pp. 32–34.
Custer, L.P. “Blepharoptosis.” Ophthalmology, edited by M. Yanoff and J. Duker, 3rd ed., Mosby, 2008, pp. 450–477.
Rose, J. and M. Lucarelli. “Cosmetic facial anatomy.” Gladstone and Nesi’s Oculoplastic Surgery Atlas, edited by J.G. Gladstone et al., Springer, 2005, pp. 1–23.
Jelks, G.W. et al. “The influence of orbital and eyelids anatomy on the palpebral aperture.” Clinics in Plastic Surgery, vol. 18, no. 1, January 1991, pp. 183–195.
Frueh, B.R. “The Mechanistic classification of ptosis.” Ophthalmology, vol. 87, no. 10, October 1980, pp. 1019–1021.
Gleen, W.J. “Reconstruction of the eyelid and related structures.” McCarthy Plastic Surgery, vol. 2, W.B. Saunders, 1991, pp. 1752–1774.
Sevel, D.A. “Reappraisal of the development of the eyelid.” Eye, vol. 2, 1988, pp. 123–129.
Seeley, R. et al. “The special senses.” Anatomy and Physiology, 2003, pp. 502–546.
Hassan, A. “Eyelid reconstruction.” Michigan Manual of Plastic Surgery, edited by D. Brown and G. Borschel, Lippincott Williams & Wilkins, 2004, pp. 109–115.
Torre, J. et al. “Aesthetic eyelid ptosis correction: A review of technique and cases.” Plastic and Reconstructive Surgery, vol. 122, no. 2, 2003, pp. 655–660.
Wagner, R. et al. “Treatment of congenital ptosis with frontalis suspension: A comparison of suspensory materials.” Ophthalmology, vol. 91, 1984, pp. 245–248.
Newman, M. and H. Spinenelli. “Reconstruction of the eyelids, correction of ptosis and canthoplasty.” Grabb and Smith’s Plastic Surgery, edited by C.H.M. Thorne, 6th ed., Lippincott Williams & Wilkins, 2007, pp. 397–412.
Carraway, J.H. “Reconstruction of the eyelids and correction of ptosis of the eyelid.” Grabb and Smith’s Plastic Surgery, edited by S.J. Aston et al., 5th ed., Lippincott-Raven, 1997, pp. 529–544.
Thorne, C.H.M. and J.H. Aston. “Aesthetic surgery of the aging face.” Grabb and Smith’s Plastic Surgery, edited by S.J. Aston et al., 5th ed., Lippincott-Raven, 1997, pp. 633–650.
Chen, W.P. “Blepharoptosis.” Color Atlas of Cosmetic Oculofacial Surgery, edited by W.P. Chen and J. Khan, 2nd ed., Saunders Elsevier, 2010, pp. 193–210.
Azurin, D.J. and A. Versaci. “Eyelid Reconstruction.” Plastic Surgery Secrets Plus, edited by J. Weinzweig, 2nd ed., Mosby, 2010, pp. 388–394.
Machula, K.B. “Congenital ptosis and complications of surgery.” Plastic and Reconstructive Surgery, vol. 81, 1988, pp. 789–810.
Moscato, E. and S.R. Seiff. “Frontalis suspension for the correction of blepharoptosis.” Evaluation and Management of Blepharoptosis, edited by A. Cohen and D. Weinberg, Springer, 2011, pp. 217–227.
Friedhofer, H. “Correction of blepharophimosis with silicone implant suspensor.” Plastic and Reconstructive Surgery, vol. 117, 2006, pp. 1428–1434.
Dickinson, A.J. “The eyelid.” Oxford Textbook of Ophthalmology, vol. 1, Oxford University Press, 1999, pp. 355–1142.
Spinelli, H.M. “Ptosis and upper eyelid reconstruction.” Atlas of Aesthetic Eyelid and Periocular Surgery, Elsevier, 2004, pp. 92–119.
Rice, T.A. et al. Operative Surgery. Butterworth, 1984, pp. 28–42.
Arajy, Z.Y. “Open loop fascial sling for severe congenital blepharoptosis.” Journal of Craniomaxillofacial Surgery, August 2011.
Ben Simon, G.J. et al. “Frontalis suspension for upper eyelid ptosis: Evaluation of different surgical designs and suture material.” American Journal of Ophthalmology, vol. 140, 2005, pp. 877–885.
Metha, P. et al. “Functional results and complications of polyester mesh use for frontalis suspension ptosis surgery.” British Journal of Ophthalmology, vol. 88, 2004, pp. 361–364.
Evoil, A. et al. “therapeutic options in ocular myasthenia gravis.” Neuromuscular Disorders, vol. 11, 2001, pp. 208–216.
Becher, M. et al. “Oculopharyngeal muscular dystrophy in hispanic new mexicans.” JAMA, vol. 286, 2001, pp. 2437–2440.
Beard, C. “A new classification of blepharoptosis.” International Ophthalmology Clinics, vol. 29, no. 4, 1989, pp. 214–216.
Roggonkamper, P. and Z. Nussgens. “Frontalis suspension: The treatment of essential blepharospasm unresponsive to botulinum-toxin therapy—long-term results.” Graefe’s Archive for Clinical and Experimental Ophthalmology, vol. 235, 1997, pp. 486–489.
Patrinely, J. and R.L. Anderson. “The septal pulley in frontalis suspension.” Archives of Ophthalmology, vol. 104, no. 11, 1986, pp. 1707–1710.
Spoor, T. and G.M. Kwitko. “Blepharoptosis repair by fascia lata suspension direct tarsal and frontalis fixation.” American Journal of Ophthalmology, vol. 109, no. 3, 1990, pp. 314–317.
Katowitz, J. “Frontalis suspension in congenital ptosis using a polyfilament, cable-type suture.” Archives of Ophthalmology, vol. 97, 1979, pp. 1659–1663.
Liu, D. “Blepharoptosis correction with frontalis suspension using a nylon monofilament sling: Duration of effect.” American Journal of Ophthalmology, vol. 128, 1999, pp. 772–773.
Harrad, R.A. et al. “Amblyopia and strabismus in congenital ptosis.” Eye, vol. 2, 1988, pp. 625–627.
Goldberger, S. et al. “Double rhomboid silicone rod frontalis suspension.” Ophthalmic Plastic and Reconstructive Surgery, vol. 7, no. 1, 1991, pp. 48–53.
Wasserman, B. et al. “Comparison of materials used in frontalis suspension.” Archives of Ophthalmology, vol. 119, 2001, pp. 687–691.
Wilson, M.E. and R.W. Johnson. “Congenital ptosis: Long-term results of treatment using lyophilized fascia lata for frontalis suspension.” Ophthalmology, August 1991, vol. 98, pp. 1234–1237.
Grover, A.K. et al. “Recent advances in lid, orbital and lacrimal surgery.” Advances in Ophthalmology, vol. 2, edited by A. Garg et al., Jaypee Brothers Medical Publishers, 2005, pp. 713–716.
Hintschich, C.R. et al. “Mersilene mesh brow suspension: efficiency and complications.” British Journal of Ophthalmology, April 1995, vol. 79, no. 4, pp. 358–361.
