
+91 6002993949
submission@iarconsortium.org
Open Access
ISSN (Print) : XXXX-XXXX
ISSN (Online) : 2708-3594
Suicide as a cause of death is a tragic consequence. This study aim to show the suicide cases in Basrah during the period from 1990-2001. Cases were collected from the Autopsy reports of medicolegal cases. 144 cases were enrolled in this study based on diagnosis of suicide cases during this period. The incidence rate of suicide in Basrah was about 1 per 100,000 population over the twelve years period of 1990 -2001. No constant trend or change in suicide rate was observed apart from minor fluctuations. The majority of suicide cases were adolescents and young Adults with predominant male cases (male to female ratio was 4:1) most of them committed their act in home. High proportion of suicide cases were committed by military personnel. The main methods used for suicide were firearms followed by poisoning and hanging.
The National Institute of Mental Health, Maryland, USA defined Suicide as death caused by self-directed injurious behavior with intent to die as a result of the behavior [1-2].
The international Classification of disease the tenth revision (I.C. D. 10) was used to classify the methods of suicide as follows [3]:
X 61 intentional self-harm by anti- epileptic, sedative hypnotic, anti-parkinsonism and psychotropic drugs
X 68 intentional self- harm by exposure to pesticides
X 70- intentional self-harm by hanging, strangulation and suffocation
X 72- intentional self- harm by hand gun discharge
X 73- 1intentional self-harm by rifle, shot- gun and large firearmdischarge
X 76 Intentional self-harm by fire and flames
X 79 Intentional self-harm by blunt object
Study Design:
This is a retrospective record-based study included all medicolegal cases admitted to the forensic medicine unit of Basrah Governorate for post-mortem report. The
period of the study was from the first of January 1990 to the end of December 2001.
Source of Data
Autopsy reports of medicolegal cases including Toxicological examination of blood, histopathological examination of tissues, gross examination findings, and hospital notes (for those who were admitted). In addition other information were derived from:
Forensic medicine annual death records and death certificates
Police requests
C- National statistics office (Basrah- Center)
About 14648 medicolegal reports were reviewed and examined thoroughly, for each case the following information were obtained: Age, sex, occupation, address, the date of police request and medicolegal report, religion, time of act of suicide, place of death and method of suicide.
Each completed or documented case was reviewed with the Autopsy report in details item by item to ensure consistency with the police request. More details about each case were obtained through direct interviewing of doctors in charge of the forensic medicine unit.
The diagnosis of suicide cases by the doctors in charge was based on the followings:
Gun Shot
Circumstance of death
Scene of death
C- Site of 1njury, selected sites for suicide include head, mouth
heart, epigastrium....ect. and whether he or she was right or left handed.
Number of bullets, most commonly single
Distance of discharge (contact, near, distant) usually near
(Short) distance associated with elements of discharge (flame, smoke, Unburned powder or tattoos)
II) Burning injury based mostly on circumstance of death and police inquest
III) Poisoning and drug overdose and asphyxia (hanging) depend on circumstances of death and taxological and autopsy findings
Age and Gender Distribution
During the 12-year period a total of 144 suicide cases were recorded in the forensic medicine unit in Basrah Governate, of these 114 79.2% were males and 30 20.8% were females giving a male: female ratio of 4:1. The majority 57.6% of cases were in the age group of 15-24 years. The percentage declined with the increase in age to reach less than one percent 0.7% in the age group 65 and above. Table1.
Table1: Distribution of suicide cases according to age and sexsex

Occupation Distrbution
Of the 114 suicide cases among males, 49 (43%) were involved in military work, 29 (25.4%) were self-employed, students and unemployed represented (7.9%) each, while those involved in the other govevmental services and the retired represented 6.1% and 5.3% respectively. With respect to female cases, the majority (96.7%) were housewives. Table 2
Table 2: Distribution of suicide cases according to sex and occupation
Place of Residence Distrbution
About threequarters 76.3% of the suicide cases recorded in the forensic medicine unit were residents of Basrah Governorate, the remaining were from other pa8s of the country, about half the Basrah resident cases were from the city center. Table 3.
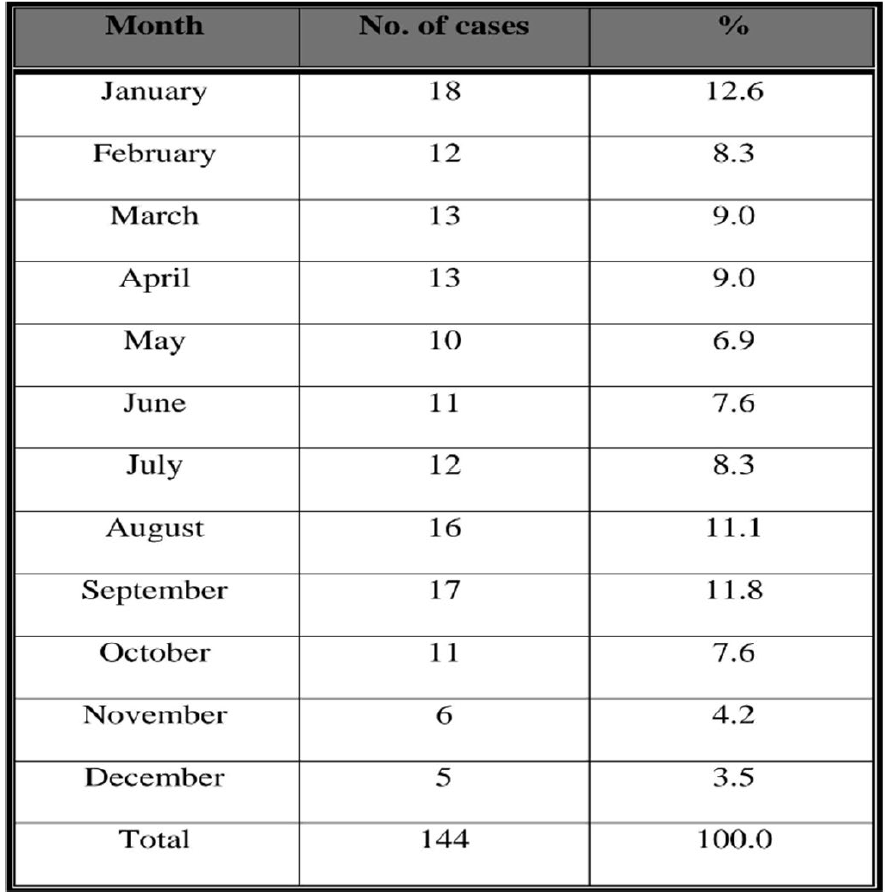
Table 3: Distribution of suicide cases according to month of reporting
Religion Distribution
All the suicide cases in the present study except two (one male and one female), were Muslims.
Seasonal Variation Distribution
The distribution of suicide cases according to month of reporting is shown in Table 4. As can be seen from the table, the majority of suicide cases took place in January 12.6% followed by September and August 1 .8% and 11.1% respectively.
Time of Suicide Distribution
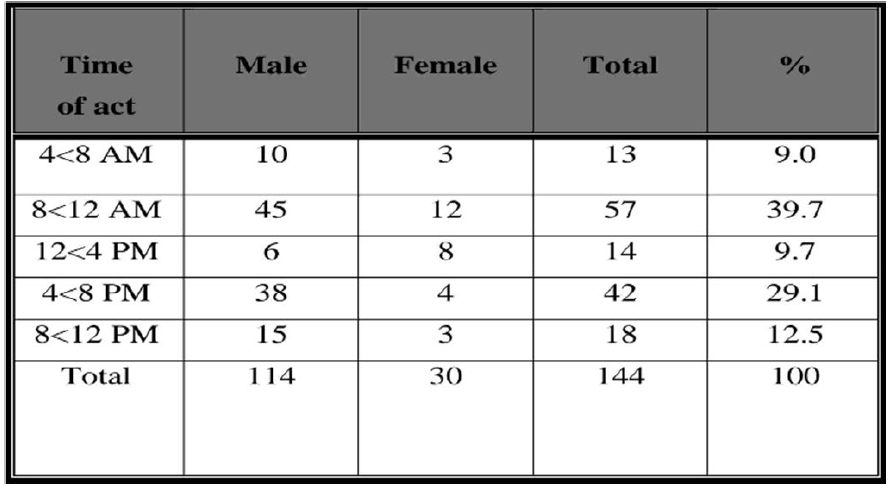
Most cases of suicide were committed at hours 8-12 AM 39.7%, another peak time for suicide was at 4-8 PM 29.1% as shown in Table 5
Figure 5: Distribution of suicide cases according to time of act of suicide
Place of Suicide
The majority (68.1%) of suicide cases were committed at home, (26.4%) at work, and only few cases (5.6%) were committed at public places.
Figure 6: Distribution of suicide cases according to place of suicide
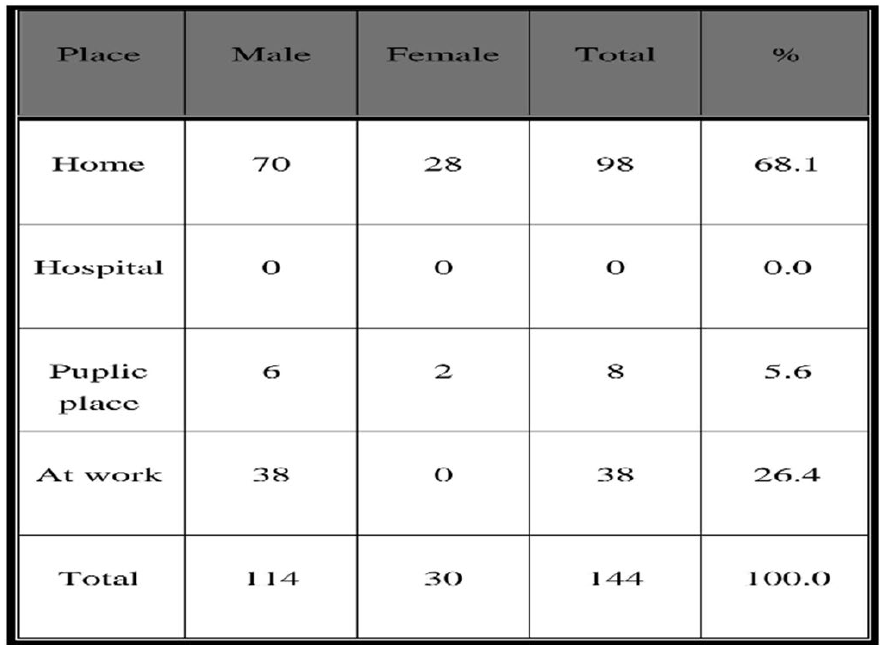
Table 7: Distribution of suicide cases according to the method used for suicide
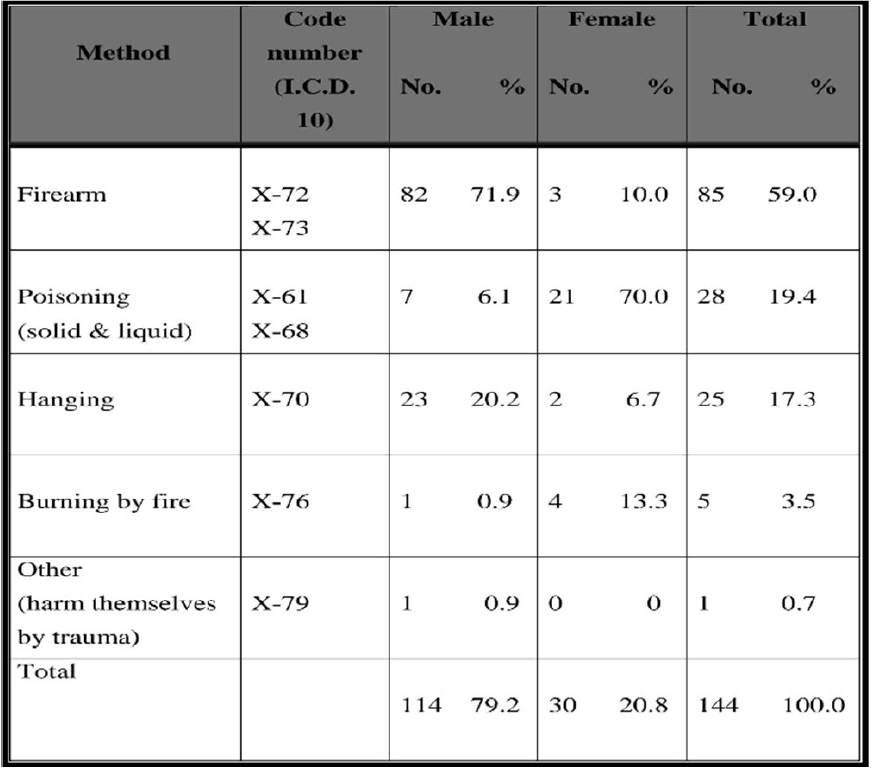
Mothed of Suicide
Firearm was the main method used to commit suicide. Eighty-two 71.9% of males and females used this method. Poisoning was the second most common method used by 7 6.1% of males and 21 70% of females. This is followed by hanging 20.2% and 6.7% of male and females respectively.
According to this retrospective record-based study the approximate annual incidence rate of suicide in Basrah during the period 1990 --2001 was found to be one per 100,000 population. This is close to the results of a study carried out in Baghdad in 1991--1992 which found an incidence rate of 1.6 per 100,000 and to that of a study in Egypt which reported an incidence rate of 0.7 per 100,000[4-5].
However it was markedly lower than that reported for other developing anddeveloped countries. The reported rates were as follows : India [6] 37/100,000, West Germany, Austria and Hungary [7] 20-30 /100,000, and Italy, Greek, Norway, Uganda and Thailand [8] 2-3/100,000.The low incidence rate of suicide in Basrah according to the present study may be due to:
The limitation of studies based on routinely collected data whichare almost always incomplete and 1n many respects 1inaccurate (presence of error and deficiency are the main disadvantages)'”. In addition one of the problems 1s that many medicolegal deaths are not autopsied because of legal decision
Word wide a lower rate of suicide was observed in Catholicregions the United States and Europe, and in Islamic countries in which suicide 1s formidable due to a variety of social, legal and religious factors
Many individuals who commit suicide make it look like an accident so their survivors spared of any stigma, this makes reporting and diagnosis of suicide difficult. This also makes 1t impossible to estimate accurately the number of deaths by suicide.
The time trend of suicide rate in Basrah over the years of study showed no major changes a part from minor fluctuations.
The majority of suicide cases were in the age group 15-24 years 57.6% of total cases, followed by the age group 25-34 years 18.7%. This may indicate a higher incidence among adolescents and young adults compared to other age. The same result (male to female ratio of 4:1) was obtained in a study of suicide in Australia [9] in 1992 - 1996, which involved a detailed review of coroners records of every suicide). Another study in Pakistan [10] found a male to female ratio of 2 :1
Hebert-Hendin [11] as early as 1962 mentioned that successful suicide is more frequent in men than women with great variations of 2 to 8 times’9’.
Another finding was the range of methods used for suicide especially burning in young females aged 15- 45 years. This method was chosen by females maybe due to the fact that it could appear as an accident, this may protect their families from the stigma of suicide, or it may be thought of as a punishment for a sin that will be difficult to be accepted in regard to cultural and religious factors.
In a study of the epidemiology and mortality of burns in the south west of Iran [12], mortality was found to be significantly higher for self-inflected burn 78% than for accidental burn)
The methods in males were restricted to firearms, hanging, poisoning and drug overdose, no other methods were recorded. This may reflect the availability of the suicide weapon. As for poisoning the presence of chemicals in the form of detergents and insecticides by the hands of almost all housewives especially in agricultural areas account for their being the easiest method for suicide. The same applies for drugs as antidepressants, hypnotics, neuroleptics that were used even without prescription especially at age of 15-24 years. The same points were discussed in many previous studies [13-14].
The incidence rate of suicide in Basrah was about 1 per 100,000 population over the twelve years period of 1990 -2001
No constant trend or change in suicide rate was observed apart from minor fluctuations
The majority of suicide cases were committed by adolescents and young Adults with predominant male cases ( male to female ratio was 4:1)
High proportion of suicide cases were committed by military personnel
The main methods used for suicide were firearms followed by poisoning and hanging
The majority (68.1%) of suicide cases were committed at home
The majority of suicide cases were committed at first twelve hours of the day (8 am—8 pm) which 1s the peak time for depression, highest proportion of suicide cases occurred during January followed by September and August
U.S. Department of Health and Human Services. Healthy people 2010: Understanding and improving health. 2nd ed., vol. 2, Washington, DC: U.S. Department of Health and Human Services, 2000.
World Health Organization. Suicide prevention (SUPRE). Geneva, Switzerland: World Health Organization, 2007.
World Health Organization. Prevention of suicide: Guidelines for the formulation and implementation of national strategies. Geneva, Switzerland: World Health Organization, 1996.
Alkamil, E.A. Health states indicators of geriatric population. PhD thesis, College of Medicine, University of Basrah.
Salman, P. and G. Meyer. Suicide: Abnormal psychology. 2nd ed., Ally and Bacoy, 1984, pp. 329–330.
Pokorny, A. “Suicide rates in various psychiatric disorders.” Archives of General Psychiatry, vol. 139, no. 9, 1964, pp. 449–506.
Feinstein, Robert E. “Suicide and violence.” In Psychiatry, edited by Eutler J. L. and Marcus E. R., Philadelphia: W. B. Saunders Company, 1999, pp. 201–220.
Yip, P.S. “Age, sex, marital status and suicide.” Psychiatry Reports, vol. 82, no. 1, 1998, pp. 311–322.
Khan, M.M.R. “The pattern of suicide in Pakistan.” Crisis, vol. 21, no. 1, 2001, pp. 31–35.
Hendin, H. “Psychiatric emergencies.” In Comprehensive Textbook of Psychiatry, edited by Alfred M. and Fredman H. I. K., Baltimore and New York: Williams and Wilkins Company, 1967, pp. 1170–1179.
Panjeshahin, M. R. et al. “Epidemiology and mortality of burns in southwest Iran.” Burns, vol. 27, no. 3, 2001, pp. 219–226.
Holinger, P.C. “Adolescent suicide: An epidemiological study of recent trends.” American Journal of Psychiatry, vol. 135, 1978, pp. 750–754.
Haynes, R.H. “Suicide in Fiji: A preliminary study.” British Journal of Psychiatry, vol. 145, 1984, pp. 433–438.
