
+91 6002993949
submission@iarconsortium.org
Open Access
ISSN (Print) : XXXX-XXXX
ISSN (Online) : 2708-3594
Objectives: To evaluate safety and effectiveness of Percutaneous nephrolithotomy (PCNL) over the last 2 years (from January 2018 to January 2020) in a single center in terms of demographic profile, stone characteristics, stone clearance, requirement of additional procedures and reported complications. Materials and Methods: This is a retrospective study which included all patients who underwent PCNL at King Hamad University Hospital (KHUH), Bahrain from January 2018 to January 2020. Both standard and mini PCNL were used as required. Various lithotripters were used according to preference of the surgeon. Data analysis was performed regarding demographic profile, laboratory investigations, imaging, operative time, stone clearance, complications and hospital stay. Stone analysis was performed in all of our cases to know the nature of stones. Collection of data was performed through standard structured questionnaire and retrieved from KHUH data base system. Statistical analysis was performed with statistical package for the social science (SPSS Inc, Chicago, Illinois, USA) version 25.0. Results: A total of 54 cases were included in the study. The mean age was 45.5 years. Forty-two patients were male and 12 patients were female giving a male: female ratio of 3.5:1. Average size of stone was 2.15cm (as assessed by Non contrast CT scan) with most common location being lower calyx and pelvis (33.3%) followed by pelvis alone (18.5%). Partial and complete staghorn stones were present in 14.8 and 11.1 % respectively. Lower calyx the most common site of puncture (94.4%). Mean hemoglobin drop was 0.57gm/dl. Stone clearance rate was 88.9%. We encountered bleeding as major complication with blood transfusion required in 3 (5.5%) of cases. Mean hospital stay of patients was 3.2 days. Conclusions: PCNL performed at KHUH Urology center remains a safe and effective minimally invasive treatment modality for large renal stones with an acceptable stone clearance rate and minimal morbidity in experienced hands.
Nephrolithiasis is a widely prevalent problem all over the world [1]. It is also a major health problem in Bahrain with its increasing incidence, prevalence and in terms of emergency hospital visits [2]. Percutaneous nephrolithotomy (PCNL) is a standard treatment for the large (>2cm) and complex renal stones [3,4]. It was first reported by Fernström and Johansson [5] in 1976. Since then, the technique has evolved over the years with miniaturization of instruments, superior optics and wide range of lithotripters [6]. PCNL has widely been accepted as a very safe and effective method due to its minimal invasiveness, lower morbidity, shorter operative time, lower postoperative complications and shorter hospital stay [7]. In this study, we investigate our experience of PCNL over the last two years in terms of stone clearance, frequency of complications, length of hospital stays and other factors in order to draw a conclusion to the overall safety of this procedure.
This study was conducted in the Department of Urology, King Hamad University Hospital, Bahrain after getting clearance from the hospital ethical committee. This is a retrospective cohort study. Data was analyzed from medical records of our hospital data base system regarding all patients who underwent PCNL from January 2018 to January 2020. Data was collected as per standard questionnaire, including patients’ age, body mass index (BMI), complete blood count, serum creatinine, urinalysis, urine culture and coagulation profile. Non contrast multi-slice CT scan images were analyzed to see stone location and number of stones. Stone size was determined by the largest longitudinal diameter on CT. Stone were termed as complex if present in multiple calyces or staghorn (complete/partial).
Per operative data was collected in terms of operative time, number of punctures, dilatation (standard PCNL / Miniperc), fluoroscopic stone clearance.
Postoperative data were collected regarding complications as per Clavien Dindo classification reference, total number of hospital-stays, post-operative complete blood count post-operative Hb%, stone clearance and additional procedure was required or not.
All procedures were done under general anesthesia. Initially, cystoscopy was performed to insert ureteric catheter into renal pelvi-calyceal system under fluoroscopic guidance. In prone position, a puncture was done by 18G initial puncture needle under fluoroscopic guidance after injecting contrast medium (Sodium diatrazoate 76%). A 0.035/0.038ʺ hydrophilic guide-wire was inserted and advanced down the ureter under image intensifier. Next, balloon dilatation was performed over guide wire. Then standard nephroscope or mini nephroscope was introduced over amplatz sheath. Pneumatic, ultrasound or integrated (Swiss Lithoclast Master, AMS) lithotripter or Ho:Yag laser were used to break the stones. Usually, a ureteric catheter was left in situ instead of Double J stent and removed after 48 hours. Nephrostomy tube was inserted in most cases and removed on second post-operative day.
Postoperatively, a KUB X-ray/USG KUB was done to see the residual stone, if any. Stone analysis was performed in every patient to know nature of the stone.
Data was analyzed on the Statistical Package for the Social Sciences (SPSS Inc., Chicago, IL, USA) version 25.0.
Sixty-two cases were investigated from January 2018 to January 2020.Out of those 62 cases, 54 cases were included in the study as 8 were lost to follow up.
Among these 54 cases, 42 were males and 12 were females giving a Male: Female ratio of 3.5:1 (Figure 1).
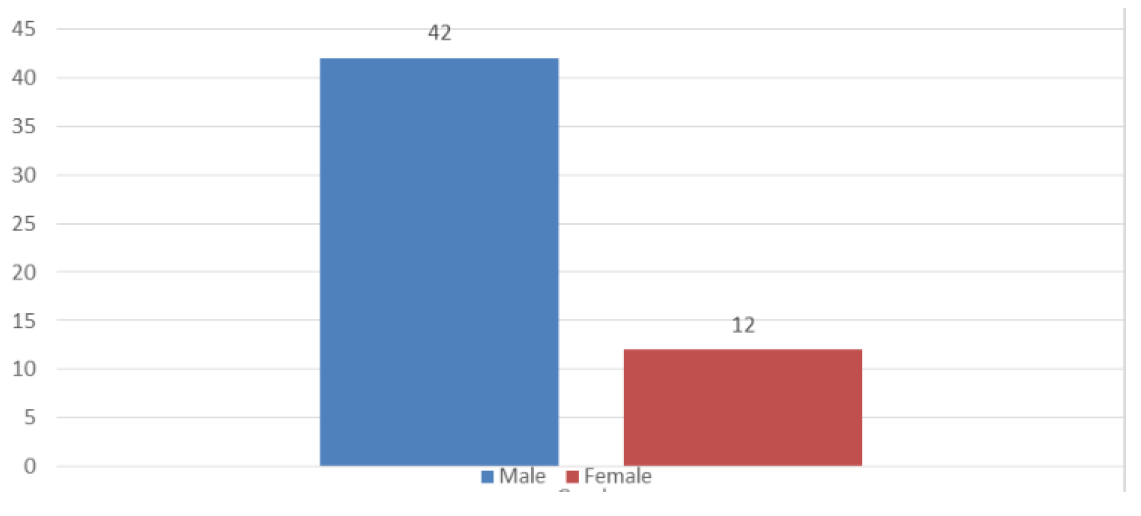
Figure 1: Gender characteristics
The mean age of our patients was 45.5 years (±12 SD) and the mean BMI was 30.18 kg/m2 (± 6.24 SD) as shown in Table 1.
Table 1: Patient clinical characteristics
Variables | Mean ± SD |
Age | 45. 50 ± 12.34 |
BMI | 30.18 ± 6.24 |
Pre-Hb | 13.53 ± 1.86 |
Post- Hb | 12. 96 ± 1.71 |
Hb drop | 0.57 ± 0.99 |
Stone size (cm) | 2.15 ± 0.93 |
Operating time (minutes) | 121.70 ± 21.35 |
Hospital stays (days) | 3.22 ± 0.53 |
The data was divided in 5 age groups: 21-30, 31-40, 41-50, 51-60 and 60-70. There was no difference in stone size, operating time and hospital stay across age groups as shown in Table 2.
Table 2: Test Statistics across age groups
Parameter | Stone size | Operating time | Hospital stays |
Kruskal-Wallis H p-value | 0.663 | 0.367 | 0.711 |
There was no difference in stone size, operating time and hospital stay across gender as shown in Table 3.
Table 3: Test Statistics across gender
Parameter | Operating time | Hospital stays | Stone size |
Mann-Whitney U p-value | 0.837 | 0.697 | 0.505 |
We found stone to be simple in 22 patients (40.7%) and complex (multiple calyces, partial or staghorn stones) in 32 patients (59.3%) as depicts Figure 2.
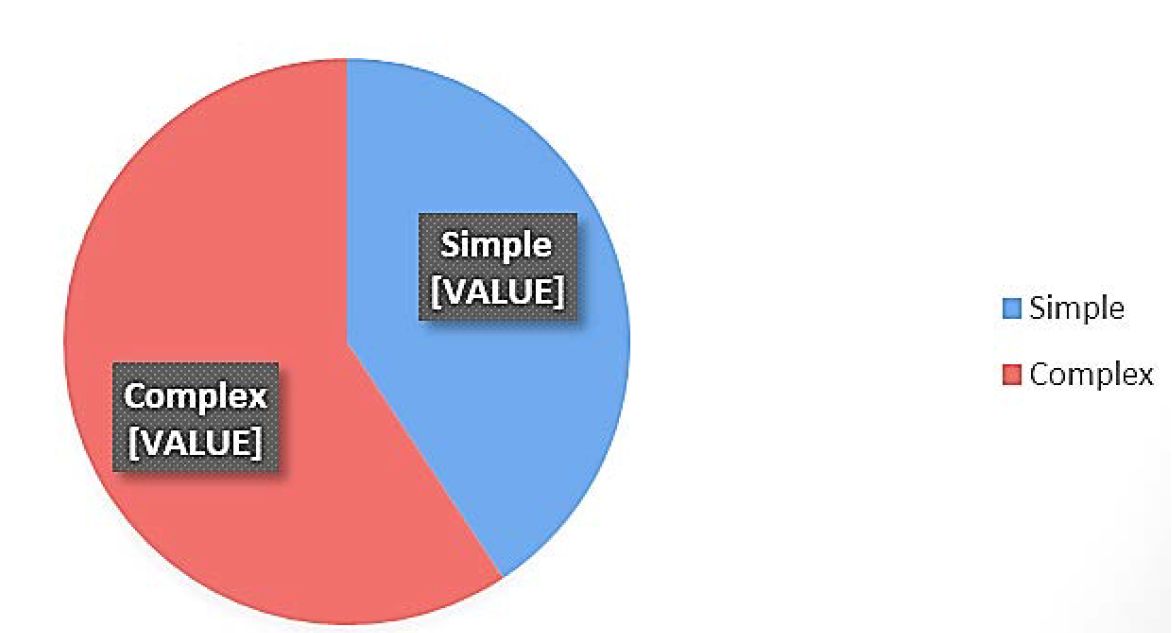
Figure 2: Stone characteristics
Partial and complete staghorn stones were present in 8 cases (14.8%) and 6 cases (11.1%) respectively.
Figure 3 shows eighteen patients had their stones located in both lower calyx and pelvis (33.3%) followed by pelvic stones (n=10; 18.5%) and stones in lower calyx (n=9;16.7%).
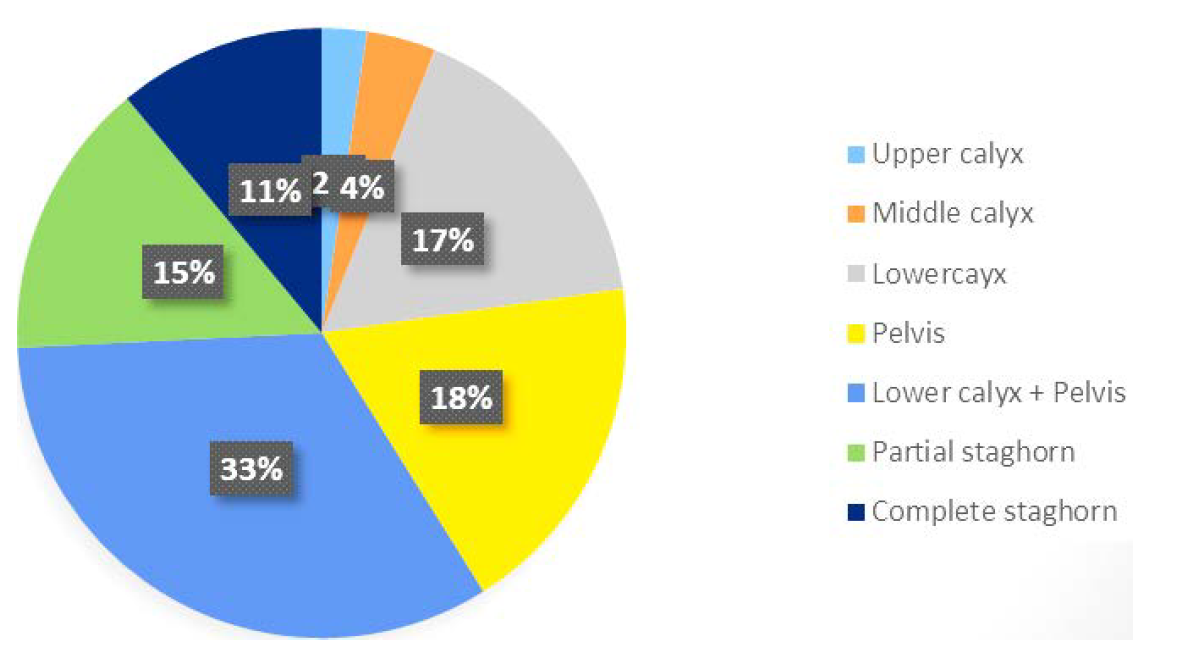
Figure 3: Stone location
In our study, lower calyceal puncture was made in most of the cases (94.4%) with two cases requiring a middle calyceal puncture (3.7%) and one requiring an upper calyceal puncture (1.9%).
Mean operative time in our study was 121 minutes (± 21). Mean hemoglobin drop was 0.57gm/dl (± 0.99). Complete clearance was achieved in 48 cases (88.9%). Six cases (11.1%) had incomplete clearance requiring additional procedures. All of these 6 cases with clinically significant residual fragments (>4mm) subsequently underwent 1-3 session of ESWL and achieved complete clearance. None of our patients required Redo PCNL or ureteroscopy (Table 4).
Table 4: Stone clearance
Variable | Frequency | Percentage |
Complete clearance | 48 | 88.9 |
Incomplete clearance | 06 | 11.1 |
Additional procedure required | 06 | 11.1 |
ESWL | 06 | 11.1 |
Redo PCNL | - | - |
Ureteroscopy | - | - |
The procedure has very low complication rate with 3 cases (5.5 %) had hemorrhage which required blood transfusion. No other complications such as fever, sepsis or pleural injury were found (Table 5).
Table 5: Complications
| Complications | Frequency | Percentage | Clavien Dindo class |
Fever | - | - | - |
Bleeding req transfusion | 3 | 5.5 | 2 |
Pleural injury | - | - | - |
Sepsis | - | - | - |
Ureteric injury | - | - | - |
The average length of hospital stay was 3.22(±0.53) days.
Regarding the nature of stones, most of them are mixed stones (95.2%) with calcium oxalate as major constituent (61%). Calcium oxalate monohydrate was found in 52% of cases and dihydrate in 9% of cases. Uric acid stone was present in 22% of cases and calcium phosphate stone was detected in 15% of cases. Cystine as stone constituent was only found in one of our cases (2%) (Figure 4).
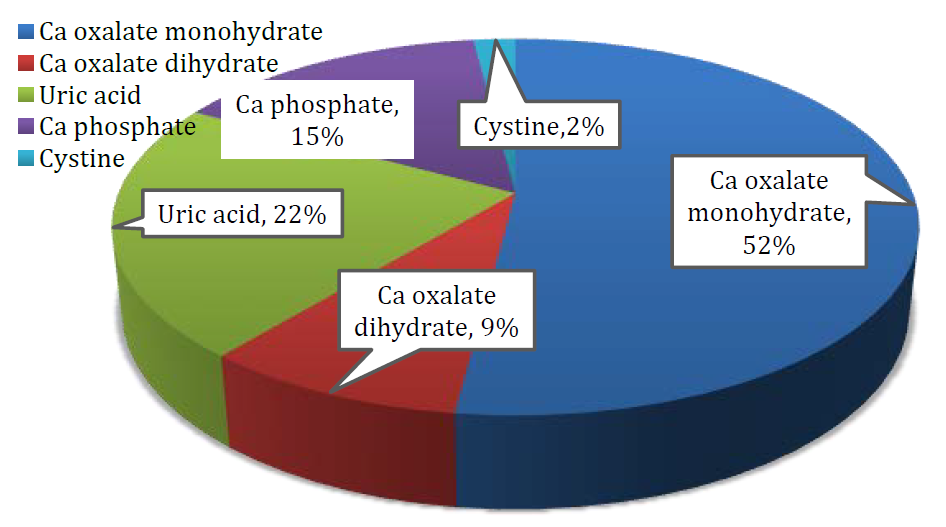
Figure 4 (Stone analysis)
This study aims to describe the safety and effectiveness of Percutaneous nephrolithotomy over the last 2 years in KHUH Urology center.
In our study, M: F ratio was 3.5, which is similar to most of the studies in the literature [7,8] reported male to female ratio as 3.8 and 3 respectively in their studies. But in the study by Agrawal et al. [9], a lower M-F ratio was reported i.e. 1.8:1, which was not found in our study.
The mean age of our patients is 45.5 years which is similar to Shohab et al. [10] who reported the mean age as 45 years. Mousavi-Bahar et al. [11] and Agbo et al. [7], in their studies, reported mean age as 40.7 and 42.2 years respectively.
Most of our patients were in the overweight/obese range by mean BMI (30.18 ± 6.24) which may increase the anesthetic, operative complications and stone clearance.
The site of punctures was through infracostal approach and the commonest site of puncture was lower calyx in 94.4% of cases which is similar to other studies reported in the literature [7,9,12].
The mean operative time in our study was 121 minutes (S.D ± 21, Range 75-177) which is similar to other studies [7,8]. There is positive correlation between stone size and operative time in our study (p value <0.05).
The stone free rate after initial PCNL (as assessed by post-operative Xray KUB or USG) is 88.9%. This is similar to the success rate reported by other authors across the globe (83.2%) [8] to more than 90% [7,12,13].
Although PCNL is considered as a safe and minimally invasive procedure for the treatment of large renal stones, it is not without complications. The two major complications of PCNL are septicemia (4.1%) and severe hemorrhage requiring blood transfusion (2.7%) [11]. In our study, we found bleeding as a major complication requiring blood transfusions in 5.5% of cases which is higher than reported, possibly because of technical difficulties related to increased patient body habitus. No patients suffered from sepsis or pleural injury. This might be explained due to per- and post-operative antibiotics coverage and a supra-costal puncture was not performed in any of our cases.
Regarding stone composition, most of our stones were mixed stones (95.2%), which is similar to the stone composition as reported from European countries [14] where mixed stones are predominant. But this is in contrast to other authors from China [15] or Pakistan [8] where pure stones are found in 37% and 41% cases respectively. The high proportion of mixed stones can be explained by the use in Europe of superior techniques of Fourier transformation infrared spectroscopy and selective sampling of significant areas, including the core and surface of stones [16].
Percutaneous nephrolithotomy (PCNL) is a very safe and effective method of treatment of large renal stones with an acceptable stone clearance rate and minimum morbidity, with reduced hospital stay and low demand for additional procedures.
Limitations
Main limitation of our study is small sample size. This is due to the fact that our center covers a small population (1,89,000) of Muharraq province in Bahrain. As we do more cases, hopefully, we can share our experience with more robust number of patients.
Acknowledgment
We would like to thank our entire urology team of KHUH for their constant help, encouragement and support. We would also like to thank our education department for their help, support and statistical analysis. We are also very thankful to IT and administration for their necessary support.
Scales Jr., C.D. et al. “Prevalence of kidney stones in the United States.” European Urology, vol. 62, no. 1, 2012, pp. 160-165.
Elshehry, A. et al. “Urolithiasis visits and trends.” Bahrain Medical Bulletin, vol. 38, no. 4, 2016, pp. 211-213.
Tiselius, H.G. et al. “Guidelines on urolithiasis.” European Urology, vol. 40, no. 4, 2001, pp. 362-371.
Preminger, G.M. et al. “Chapter 1: AUA guideline on management of staghorn calculi: Diagnosis and treatment recommendations.” The Journal of Urology, vol. 173, no. 6, 2005, pp. 1991-2000.
Fernström, I. and B. Johansson. “Percutaneous pyelolithotomy: A new extraction technique.” Scandinavian Journal of Urology and Nephrology, vol. 10, no. 3, 1976, pp. 257-259.
Ganpule, A.P. et al. “PCNL in the twenty-first century: Role of Microperc, Miniperc and Ultraminiperc.” World Journal of Urology, vol. 33, no. 2, 2015, pp. 235-240.
Agbo, C.A. et al. “Percutaneous nephrolithotomy (PCNL): A single-centre experience.” IOSR Journal of Dental and Medical Sciences, vol. 16, 2017, pp. 38-40.
Rizvi, S.A.H. et al. “Surgical outcomes of percutaneous nephrolithotomy in 3402 patients and results of stone analysis in 1559 patients.” BJU International, vol. 120, no. 5, 2017, pp. 702-709.
Agrawal, M.S. et al. “Ultra-mini-percutaneous nephrolithotomy: A minimally invasive option for percutaneous stone removal.” Indian Journal of Urology: Journal of the Urological Society of India, vol. 32, no. 2, 2016, pp. 132.
Shohab, D. et al. “Effect of body mass index on operative time, hospital stay, stone clearance, postoperative complications and postoperative analgesic requirement in patients undergoing percutaneous nephrolithotomy.” Turkish Journal of Urology, vol. 41, no. 4, 2015, p. 177.
Mousavi-Bahar, S.H. et al. “Percutaneous nephrolithotomy complications in 671 consecutive patients: A single-center experience.” Urology Journal, vol. 8, no. 4, 2011, pp. 271-276.
Damera, R. and K. Karthik. “Percutaneous nephrolithotomy in patients with solitary kidney-SVIMS experience.” IOSR Journal of Dental and Medical Sciences, vol. 15, no. 11, 2016, pp. 100-103.
Ganpule, A. and Mahesh Desai. “Fate of residual stones after percutaneous nephrolithotomy: A critical analysis.” Journal of Endourology, vol. 23, no. 3, 2009, pp. 399-403.
Daudon, Michel et al. “Sex- and age-related composition of 10,617 calculi analyzed by infrared spectroscopy.” Urological Research, vol. 23, no. 5, 1995, pp. 319-326.
Jing, Z. et al. “Analysis of urinary calculi composition by infrared spectroscopy: A prospective study of 625 patients in eastern China.” Urological Research, vol. 38, no. 2, 2010, pp. 111-115.
Rizvi, S.A. et al. “Evaluation of children with urolithiasis.” Indian Journal of Urology: Journal of the Urological Society of India, vol. 23, no. 4, 2007, p. 420.
