
+91 6002993949
submission@iarconsortium.org
Open Access
ISSN (Print) : XXXX-XXXX
ISSN (Online) : 2708-3594
Bisalbuminemia is a rare condition associated with two distinct bands in albumin region seen on serum protein electrophoresis due to difference in their mobility. The condition can either be inherited in autosomal dominant pattern or acquired. It is seen in association with various conditions like diabetes mellitus, sarcoidosis, Waldenstrom's macroglobulinemia, nephrotic syndrome, chronic kidney disease, multiple myeloma, Alzheimer's disease, pancreatic pseudocyst and in patients receiving high doses of penicillin. The band may be misinterpreted as an abnormally located M band if the person is not aware of the band. Here we are presenting a case of multiple myeloma with incidentally detected bisalbuminemia.
Bisalbuminemia is a rare condition characterized by an extra band in the albumin region with prevalence between 1:10000 to 1:1000 [1]. It is autosomally inherited or can be acquired. The transient acquired form is being detected in multiple conditions including diabetes mellitus, sarcoidosis, Waldenstrom's macroglobulinemia, nephrotic syndrome, chronic kidney disease, multiple myeloma and in patients receiving high doses of penicillin [1-5]. SPEP shows two distinct bands in albumin region with two peaks in the albumin region on densitometry, multiple myeloma, also known as plasma cell myeloma, is clonal proliferation of plasma cells in the bone marrow and comprises around 10% of hematological malignancies [5].It is a multifocal process occurring in association with M spike in serum and/or urine electrophoresis measured by densitometry.
Case 1 was a 53-year-old male presenting with lower back pain and bilateral lower limb weakness for five months. X ray skull revealed multiple lytic lesions. Bone marrow aspirate was hypercellular and showed 45% plasma cells. Flowcytometry showed clonal plasma cells, which were strongly positive for CD138 and lambda restricted. Serum protein electrophoresis (SPEP) showed two distinct bands in the albumin region and a prominent M-spike in the gamma globulin region (Figure 1).

Figure 1: Serum protein electrophoresis showing 2 bands in albumin region with an M band in gamma region
Case 2 was a 53-year-male, with a history of chronic kidney disease. SPEP showed two distinct bands in the albumin region; there was no M-spike. (Figure 2). Urine protein electrophoresis (UPEP) did not show any band. For both the patients, SPEP and UPEP were performed by the agarose gel electrophoresis method.
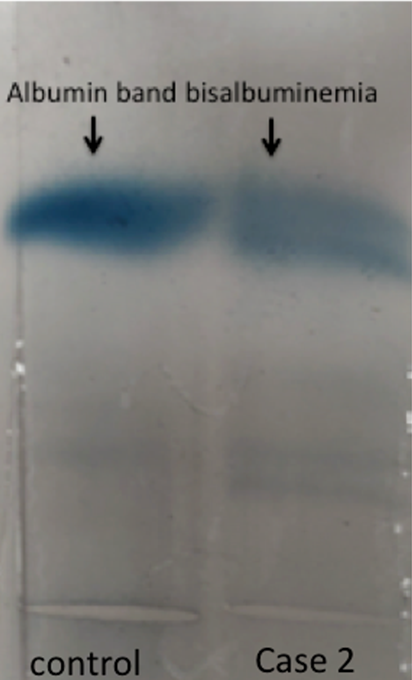
Figure 2: Serum protein electrophoresis showing 2 bands in albumin region
Bisalbuminemia can complicate the diagnostic process due to misinterpretation of the extra band of albumin variant. SPEP shows two distinct bands in the albumin region, resulting from alloalbumins, which indicate the fast- and slow-moving variants of albumin. Alloalbumins can be detected by agarose gel electrophoresis as well as by capillary zone electrophoresis [6]. M-spike or M-band is a distinct prominent and /or sharp band in the globulins region and is IgG immunoglobulin in about 50% of cases. IgA and light chains are each present in around 20% of cases and IgE, IgD, IgM and biclonal are each found in fewer than 10% of the remaining cases. M spike is an estimation of M protein, resulting from plasma proteins secreted by myeloma cells. The clonality of plasma cells can be proven by kappa or lambda restriction.
Immunofixation electrophoresis may be a solution in such situations, which leads to discernible bands in heavy and/or light chain regions in case of M-spike but not in albumin region. Though, bisalbuminemia interferes with the SPEP diagnosis, as such bisalbuminemia does not influence the disease progression or treatment. The experience and expertise in SPEP reporting help ensure the identification of even a faint M-band or spike and distinguish it from the other bands including the albumin variants.
Bisalbuminemia as such does not affect disease process though it can interfere with the interpretation of the SPEP. Subsequently, this may lead to difficulties in the reporting of SPEP in multiple myeloma. They however, can be differentiated in IFE and also need to be aware of the entity for clinching the diagnosis.
Chan, P.C. “Bisalbuminemia: Lack of association with monoclonal gammopathy and value-justification for reporting in serum protein electrophoresis.” Journal of Clinical Chemistry and Laboratory Medicine, vol. 1, no. 1, 2017, p. 108.
Chhabra, S. “Bisalbuminemia: A rarely encountered protein anomaly.” Journal of Laboratory Physicians, vol. 5, no. 2, 2013, pp. 145–146.
Ejaz, A.A. “Bisalbuminemia in chronic kidney disease.” Clinical and Experimental Nephrology, vol. 8, no. 3, 2004, pp. 270–273.
Agarwal, P. “Bisalbuminemia: A rare finding on serum electrophoresis.” Indian Journal of Hematology and Blood Transfusion, vol. 34, 2018, pp. 558–559.
Angouridaki, C. “Detection of hereditary bisalbuminemia in a Greek family by capillary zone electrophoresis.” Hippokratia, vol. 12, no. 2, 2008, pp. 119–121.
