
+91 6002993949
submission@iarconsortium.org
Open Access
ISSN (Print) : 2709-3239
ISSN (Online) : 2709-3220
Bilateral abductor vocal cord paralysis is a distressing condition, often life threatening, most commonly results from iatrogenic trauma to the recurrent laryngeal nerve during surgical procedures in the anterior neck. Patients may require tracheostomy because of acute or gradual onset of dyspnoea and airway compromise. A-32 years-old male presented with stridor without dysphonia. Indirect laryngoscopy revealed paramedian position of bilateral true vocal cord. No etiology could be identified for abductor palsy of bilateral vocal cords. Patient symptomatically improved with medical management and was planned for tracheostomy followed by vocal cord lateralization procedures.
The recurrent laryngeal nerves are more frequently involved in bilateral paralysis than any other cranial nerve. Most of the underlying lesions are iatrogenic, with thyroid surgery being the single most important causative factor. However, a variety of different reasons can lead to such a condition [1]. Whenever the aetiology is uncertain, a complete diagnostic work-up is mandatory. Patients with bilateral vocal cord paralysis have a limited airway and a persistent, soft, inspiratory stridor. Indirect laryngoscopy confirms the diagnosis. Any additional edema of the cords results in extreme dyspnoea, for which intubation or tracheostomy may become necessary. Over time, the airway may worsen as unopposed action of the cricothyroid muscle continues in patients with bilateral recurrent laryngeal nerve paralysis. Patients begin to experience improved voice but notice gradually worsening dyspnoea. We present the case report of idiopathic bilateral abductor vocal cord palsy which is rare but important clinical entity.
Case Presentation
A - 32 - years old male presented in otorhinolaryngology department with acute onset of difficulty in breathing and stridor. Patient had symptoms of upper respiratory tract infection 5 days prior to stridor. Patient had no history of any trauma and neck surgery. Patient had no comorbidity. Indirect laryngoscopy revealed paramedian position of bilateral true vocal cords and congested endolarynx (Figure 1).
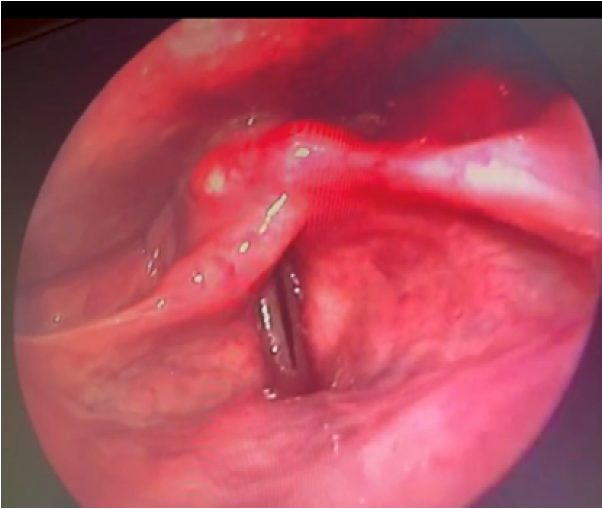
Figure 1: Indirect Laryngoscopy Showing Paramedian Position of Bilateral True Vocal Cords
No obvious endolaryngeal growth was seen. Neurological examination was normal for the patient. Magnetic resonance imaging and contrast enhanced computed tomography of neck found medialization of bilateral aryepiglottic folds with enlarged pyriform sinuses with medialization of bilateral true vocal cords with narrowing at the level of glottis. Contrast enhanced computed tomography of thorax was normal for the patient. Upper gastrointestinal endoscopy was normal. Inflammatory markers such as ESR, qCRP was also normal. Immunological profile (c-ANCA, p-ANCA, ANA) was also normal. Patient was started on injectable steroids followed by oral steroids and nebulisation was done with adrenaline. Anti allergics and proton pump inhibitors was given. Patient improved symptomatically after one week however bilateral true vocal cords were still in paramedian position on indirect laryngoscopy. Patient was planned for tracheostomy and vocal cord lateralization procedures.
Bilateral abductor palsy has tremendous psychological, emotional and social impact as the patient has to be tracheostomised for the rest of life. Vocal cord abductor palsy (VCAP) has also been previously described as ‘‘respiratory paralysis of the larynx’’ which was first described in 1863, also known as Gerhardt syndrome. Rebattu in 1936 reported that ‘‘all cases of vocal cord abductor paralysis should be considered to be secondary to syphilis in the absence of proof to the contrary’’ [2]. VCAP secondary to syphilis has become much rarer in the age of penicillin. VCAP is now essentially observed in the context of neurodegenerative disease. The characteristic clinical features consist of severe dyspnoea exclusively on inspiration, associated with little or no voice changes. Laryngeal examination reveals vocal cords with a normal morphology in a closed or paramedian position. Cases of vocal cord abductor paralysis have been reported much more recently in Parkinson’s disease, progressive supranuclear palsy, amyotrophic lateral sclerosis, autosomal dominant cerebellar ataxias and chronic inflammatory demyelinating polyneuropathy [3-6]. Few cases of VCAP secondary to infection have been reported apart from those related to influenza virus [7], and herpes simplex virus [8]. Cases of herpetic laryngeal palsy have been rarely reported in literature. Etiology of vocal fold paralysis is broad: e. g. iatrogenic/traumatic, associated with neoplasms or with systemic diseases. Iatrogenic is most commonaly seen post thyroidectomy. The incidence of post thyroidectomy vocal cord paralysis has been reported in the range of 3.5-6%, and 93-100% of these patients are reported to make complete recovery [9]. Traumatic causes include neck trauma and intubation trauma. Studies state incidence of intubation related vocal cord palsy as 0.2% [10]. Malignant causes comprise of laryngeal malignancy and no laryngeal malignancy which includes mediastinal and esophageal malignancy. Other causes are idiopathic and neuropathy such as Myasthenia Gravis and Kennedy’s syndrome [1]. In our case no etiology could be identified for the bilateral abductor palsy. Radiological imaging of neck and chest did not reveal any local cause for palsy. Similarly, neuroimaging of brain did not show any neurological cause for bilateral palsy. Immunology was also negative. Markers for inflammation were negative. Laryngeal electromyography would have been useful in our case in order to define the level of the neurological lesion. Similarly, lumbar puncture would have been useful to detect herpes simplex virus in CSF to rule out laryngeal palsy of herpetic origin. Biopsy was also not performed from vocal cords to rule out any herpetic lesion as morphology of vocal cords were normal in our case. Patient was managed conservatively and was planned for elective tracheostomy followed by posterior cordectomy.
Vocal cord abductor palsy is a complex disease in terms of its aetiology and pathophysiology, which has not been fully elucidated. Bilateral abductor vocal cord palsy can result in life threatening airway obstruction for which airway should be promptly secured. Compared to permanent tracheostomy, glottis airway widening procedures have much less impact on the patient’s quality of life and should be preferred whenever possible. Since such an operation is irreversible, a decision should be made only in the presence of a reliable electrophysiological prognosis and/or after 6–9 months of watchful waiting. Inevitably, voice quality is traded for airway normalisation. However, modern surgical techniques accomplish very tolerable phonatory results. Timing, type and extent of surgery need to be customised for every patient individually.
Rosenthal, L.H. et al. “Vocal fold immobility: a longitudinal analysis of etiology over 20 years.” Laryngoscope, vol. 117, 2007, pp. 1864–1870.
Rebattu, J. “Les lésions anatomiques dans la paralysie des dilatateurs de la glotte (à propos d’une observation anatomoclinique).” Acta Otolaryngologica, vol. 15, no. 2–4, 1931, pp. 383–392.
Plasse, H.M. and Lieberman, A.N. “Bilateral vocal cord paralysis in Parkinson’s disease.” Archives of Otolaryngology, vol. 107, no. 4, 1981, pp. 252–253.
Yokoji, I. et al. “A case of progressive supranuclear palsy associated with bilateral vocal cord abductor paralysis.” Rinsho Shinkeigaku, vol. 37, no. 6, 1997, pp. 523–525.
Palesse, N. et al. “Bilateral abductor paralysis of the vocal cords in the course of neurological diseases: report of five cases.” Italian Journal of Neurological Sciences, vol. 9, no. 1, 1988, pp. 59–62.
Isozaki, E. et al. “Myopathology of the intrinsic laryngeal muscles in neurodegenerative diseases, with reference to the mechanism of vocal cord paralysis.” Rinsho Shinkeigaku, vol. 38, no. 8, 1998, pp. 711–718.
Roy, J.N. “A case of bilateral paralysis of the laryngeal abductors of influenzal origin.” Canadian Medical Association Journal, vol. 34, no. 4, 1936, pp. 427–428.
Pou, A. and Carrau, R.L. “Bilateral abductor vocal cord paralysis in association with herpes simplex infection: a case report.” American Journal of Otolaryngology, vol. 16, no. 3, 1995, pp. 216–219.
Toutounchi, S.J.S. et al. “Vocal cord paralysis and its etiologies: a prospective study.” Journal of Cardiovascular and Thoracic Research, vol. 6, 2014, pp. 47–50.
Vyshnavi, S. and Kotekar, N. “Aphonia following tracheal intubation: an unanticipated postoperative complication.” Indian Journal of Anaesthesia, vol. 57, 2013, pp. 306–308.
