+91 6002993949
submission@iarconsortium.org
Open Access
ISSN (Print) : 2708-5155
ISSN (Online) : 2708-5163
Indoor air pollution is predominantly known as a perilous global issue by today, which poses a major threat to public health, sustainable development, socio-economic growth and prosperity in a country. Millions of deaths are produced in South Asia due to exposure of drastic health-damaging pollutants from biomass burning, poor ventilations, using inefficient stoves etc. Thus, most of the South Asian countries are exceeding the interim target for air quality defined by World Health Organization (WHO). However, Sri Lanka remains somewhat outstanding relating of air quality among other South Asian countries in case of low population and being an island most conceivably. Population of a country also partially affects to the air quality nationwide. This study assesses the Indoor Air Pollution (IAP) in Sri Lanka compared to other countries in South Asia Region (SAR) using most recent and related studies and WHO data. The indoor air quality in Sri Lanka provokes on human health and burden on the economy as a developing country yet stands at an average optimum stage among other countries in SAR, albeit it is far behind in the world.
Air pollutant is defined as “a substance in the air that, in high enough concentrations produce a detrimental environmental effect” by the United States Environmental Protection Agency (US-EPA) and further states that “these effects can be either health effects or welfare effects” [1].
Air pollution cannot be controlled as other pollutions (e.g., water, soil and solid pollutions) and predominantly associates with the environmental health problems [2-4] while increasing the global mortality rate [4]. Air pollution affects not only on public health but also on economy and aesthetics [5], resulting much concern raising among policymakers, clinicians, public health experts and the general public [1] to maintain the air quality according to the WHO standards and regulations specifically to protect public health.
Desolately, 91% of the world population live in places where air quality exceeds WHO guideline limits, while the air pollution kills an estimated 7.0 million people worldwide in every year. The serious confirmation is that the low and middle-income countries are suffering from the highest exposures of air pollutants from both indoor and outdoor, also do not have quality standards of life especially for medical care [6].
Air pollution is a major factor for ill-health in SAR [7]. In 2009, WHO has estimated the attributable deaths due to IAP would be about 4200 in Sri Lanka [1]. Previous studies indicate that the indoor air quality is much less than the WHO certified levels mainly in India, Pakistan, Bangladesh and Nepal among the SAR countries [8].
Particularly indoor air pollutants are comprised of PMs (PM2.5, PM10), biological pollutants and over 400 organic (with a low boiling point (ranging from 50/100°C to 240/260°C)) and inorganic compounds (COx, SO2, NOx, O3) (Table 1) [9]. IAP receives an orthodox concern majorly when comparing to Outdoor Air Pollution (OAP) although it is twice higher than the OAP because people spend their time mostly in air-tight buildings [9].
Thus this paper aims to review the IAP in Sri Lanka by comparing to that of in South Asian Region while summarizing the overall facts on IAP with the aid of necessary prevailing data of SAR to assess the air pollution mainly in Sri Lanka as a comparison. Section 2,3,4,5 respectively discuss the IAP in SAR and its health effects, economic cost, mitigation of IAP basically.
IAP in SAR
Household air pollution is a major source of IAP that affects the human health in both urban and rural areas. WHO conveys, almost all of the burden is in developing countries mostly reside in SAR due to inefficient solid fuel burning and usage of highly polluting stoves [10], resulting, about 0.65 million deaths and 123/DALYs/1000 capita annually in SAR [8]. In Sri Lanka, the WHO estimated number of deaths was 4300 in 2004 due to IAP [5].
The major indoor air pollutant, PM is produced through the main domestic energy sources; conventional fuels (coal, kerosene oil, domestic litter, dung and crop residues) in open fires and typical leaky stoves [7,8,11] and indoor cigarette smoking [1] and significantly affects to lung functions and growth in children [4]. Though other countries in SAR use generally charcoal, coal, cow dung, solid fuels, Sri Lanka is limited to wood for cooking and heating mainly [1]. About 78% of the Sri Lankan population use biomass stoves and mostly cooks in indoors [12], which causes a widespread of burn unclean fuels (wood, crop residue, dung) leading to a massive IAP [13]. CO, Benzene, Acetic acid, Lead, Anthracene, Phenanthrene, Benzo(α) anthracene, Dibenzoanthracene, Benzofluoroanthracene, Benzo (α) Pyrene are some of the air pollutants identified in wood smoke [5] that leads to ill-health. The traditional stoves expose to a higher rate of IAP than those with improved stoves while households with chimneys have less exposure to IAP than to without chimneys [14] while Sri Lankan households use mainly three stone or semi-enclosed type cook stoves [12,13]. Cooking with biomass fuels produces a range of harmful substances (CO, NOx, SOx, PM, formaldehyde, polycyclic organic matter) to human health [13]. In Sri Lanka indoor PM2.5 measurements were found as a mean of 84.4 mg/m3 and 44.4 mg/m3 respectively for 132 urban homes and 66 rural homes while the highest PM2.5 reported from domestics that use biomass for day today cooking [5]. Thus, IAP is a perilous risk for a large population that are inside the home during the unsafe stove operation (using solid fuels) [13]. Figure 1 indicates the WHO statistics-2018 of population with primary reliance on polluting fuels and technologies for cooking (in millions).
India is a promising consumer of unclean fuels for cooking while Maldives is ominous according to the WHO statistics. Among SAR countries, it is revealed that the Indian female cooks undergo the highest PM10 exposure (446 mg/m3) personally compared to that of both females (276 mg/m3) and males (255 mg/m3) elsewhere [8]. 62% of Pakistan people consume solid fuels [15]. Junaid et al. [8] reported that 2.8 billion people of developing countries are exposed to solid fuel burning and SAR countries are predominantly expose to extreme levels of PM due to consumption of biomass fuels in poorly ventilated households. Approximately, 74% of SAR people use solid fuels (wood, dung, coal) for heating and cooking in households [7].
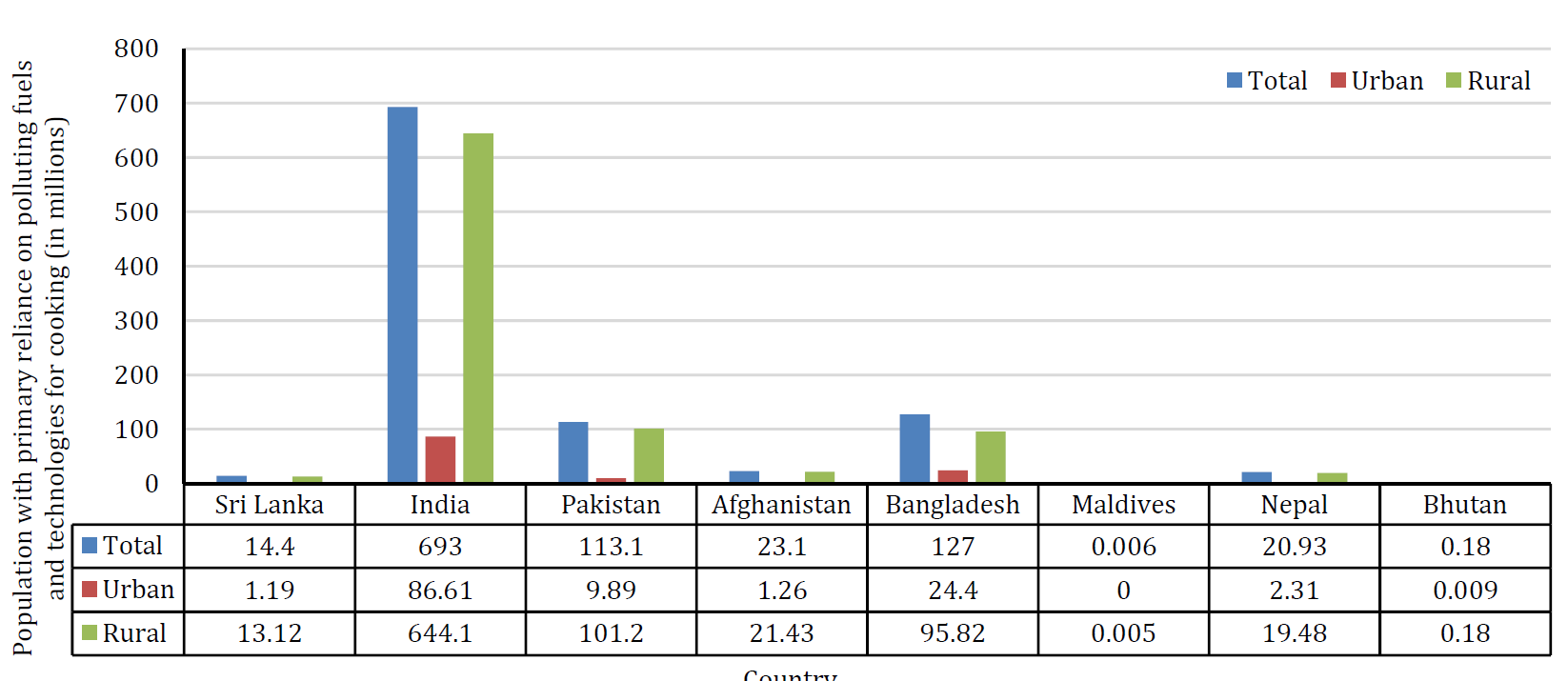
Figure 1: Population with Primary Reliance on Polluting Fuels and Technologies for Cooking of SAR Countries (2018) [18]
When considering the indoor home setting exposures, the highest levels of PM10 emissions had reported respectively in rural areas of Nepal (1400 µg/m3), in Bangladesh (1177 µg/m3) and Pakistan (957 µg/m3) among SAR countries specifically due in using biomass fuels, while, the highest PM10 levels had reported from an Indian school (during winter 1414 mg/m3 and summer 490 mg/m3) [8]. Less than 5% of people use solid fuels while the majority use electricity and Liquid Petroleum Gas LPG for cooking in households in Maldives [16].
Second Hand Smoke (SHS) is another prevailing major IAP threat in both developed and developing countries and strongly associated with a risk increment for lung cancer respiratory illnesses and cardiovascular diseases among both smokers and non-smokers [17]. About 40% of children are exposed to SHS and an estimated 165,000 children under 5 years of age die worldwide in both developing and developed world each year of lower respiratory tract infections due to SHS exposure [4]. Alagiyawanna et al. [19] achieved the facts through uni and multivariable analysis considering a group of 311 students in Sri Lanka; resulted that there was no significance in the sexuality of being exposed to SHS, mother’s unemployment status and being in the presence of smokers were the major associative risks of SHS exposures both at home and public places in Sri Lanka. In Pakistan, a restaurant with a cigarette smoking zone and pipe smoking cafe expressed the alarming levels of PM2.5 respectively 4491 mg/m3 and 2550 mg/m3due to indoor smoking and same in Nepal [8]. Nafees et al. [20] demonstrated that “Unacceptably high levels of PM2.5 exposure associated with SHS at various entertainment venues of Karachi (in 2002) even after 8 years since the promulgation of the smoke-free ordinance in Pakistan”. Lee et al. [17] has indicated that the PM2.5 level in venues (related hospitality venues such that restaurant, café, bar/club and entertainment in India, Pakistan and Sri Lanka) where smoking was observed was approximately four times higher than in non-smoking venues [17]. In fact, the studies indicate that SAR shows the daily PM2.5 concentrations (300 µg/m3 to 3000 µg/m3) beyond higher than the WHO recommended value [7].
Burning mosquito coils and incense `sticks in home also add a severe aspect in IAP producing fine PM, benzene and CO that directly affect the human health [5]. A mosquito coil generates PM2.5 about that of 100 cigarettes produces when burning [5]. Radon, which is a responsible gas for lung cancers is produced from decaying Radium in soil adjacent to the house and enters inside through pressure-driven flow [21]. Formaldehyde emits from building materials (medium-density fiber wood, plywood paneling etc.) and tobacco smoking is another indoor air pollutant which increase the respiration and skin diseases [21]. Aerosol heavy metal in domestic area is another mean of IAP. Pitawala et al. [22] studied the domestic heavy metal pollution level in Kandy and Colombo area taking household dust samples and found that the pollutant concentrations (Pb, Mn, Cr, Cu, Zn) were higher in Kandy than that of in Colombo and concluded that the reason would be the dispersion of pollutants due to sea breeze and high humidity prevailing in Colombo although it is more urbanized than Kandy.
According to Figure 2, Sri Lanka, Maldives and Bhutan indicate optimistic household air pollution attributable DALYs values (1883, 1902 per 100,000 populations respectively [23]) than that of in other SAR countries according to the recent WHO statistics. Afghanistan, Pakistan and India indicates the highest DALYs values for household air pollution respectively proving that the country’s poor indoor air quality among eight other countries in SAR. The previous studies illustrated that India, Nepal, Pakistan, Bangladesh indicate the alarming levels in IAP while Sri Lanka and Bhutan confronted with comparably lower levels [7] confirming that the high population in India, Bangladesh and Pakistan causes the higher exposure and therefore, higher number of people affect with chronic diseases [7]. Nasir et al. [24] predicted that location and region of the household, poverty, household size, low level of human capital, asset ownership and asset structure and access to basic utilities are the key factors associated with fuel choice in Pakistan using a multinomial logit model. Relatively, Maldives is in place of less DALYs rate (105, per 100,000 populations [23]) when considering IAP among SAR countries.
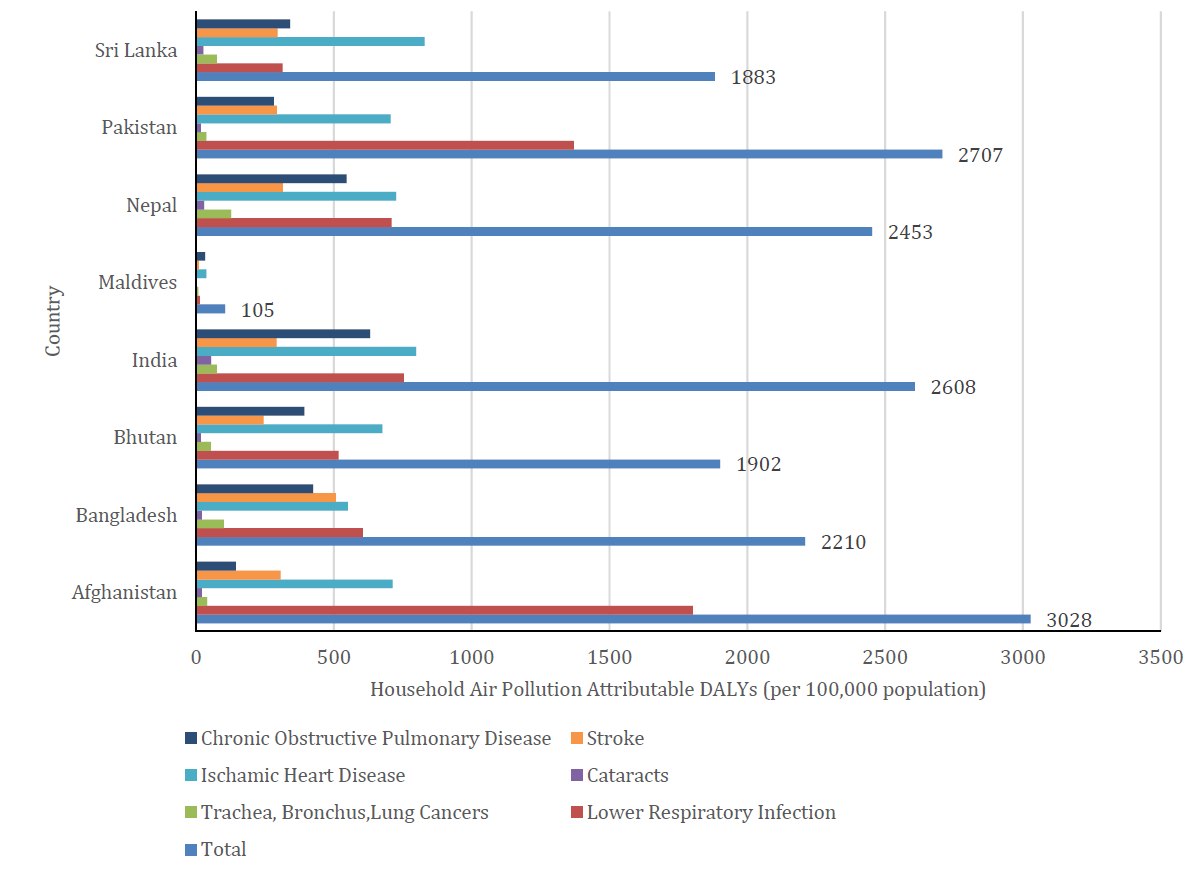
Figure 2: Household Air Pollution Attributable DALYs Values (per 100,000 population) in SAR
Source: WHO Country Health Statistics-2016 [23]
IAP and Health in SAR
Air pollution directly reduces the quality of life causing imperfections in human health and well- being for many decades worldwide [6]. The combined effects of outdoor and indoor air pollution cause about 7 million premature deaths every year globally, mostly as a result of increased mortality from diseases such that chronic obstructive pulmonary disease, stroke, heart disease, lung cancer, acute respiratory infections, stroke, chronic bronchitis (Table 1).
Several vulnerable groups that are susceptible to health outcomes of air pollution can be found in the society (unborn and small children, women in the maternity, elderly people, those who suffer from respirator-cardio diseases as well as socio economically deprived people and those who interact with toxic materials and air pollutants in day to day lives) [1,7,25]. Generally, the more suffer from severe health effects are the more susceptible to air pollutants [1]. A range of adverse health effects (Stimulation of local and systematic inflammation increased reactivity of the respiratory epithelium, bronchial irritation, reduction of O2 delivery to key organs, reduction of mucociliary clearance in the respiratory tract) can be occurring as a result of partly inter-related biological mechanisms with the reactions of many pollutants together [1].
Abdulla et al. [16] states that chronic obstructive airway diseases (emphysema and chronic bronchitis) and asthma accounts for the major reason for the chronic respiratory diseases in SAR due to indoor and outdoor air pollution. Meanwhile, Cohen et al. [26] states that the air pollution due to PM2.5 directly attributable for the mortality from cardiovascular disease (IHD and cerebrovascular disease) and DALYs globally.
Substantially, each primary household cook reported respiratory diseases such as phlegm, cough, wheeze, asthma [27] in SAR. Children who live in houses having chimneys are at less exposure to indoor PM2.5 concentrations and not significantly associated with respiratory health outcomes [27]. Studies suggest that the cook stove characteristics such as stove type, presence of chimney, location of cooking area are significant indicators of respiratory health of being lower the PM concentrations. Ranathunga et al. [28] revealed that children (under 5-year old) have high exposures to high concentrations of PM2.5 and CO in homes where cooking is done using kerosene and biomass fuel that causes infection induced asthma. Biomass fuel is the major source of cooking of about 78% of households in Sri Lanka [13]. More than half of the new pneumonia episodes are reported from India (43 million), Pakistan (10 million) and Bangladesh (6 million) considerably due to using coal, charcoal and cow dung as solid fuels as the main energy source [34].
PM2.5 is more perilous in comparison to PM10 because of the properties such as the ability to deep penetration into the alveolar sacs, high adsorption capacity and large surface area [12]. Dharshana et al. [35] clearly revealed that the PM10 has a strong relation with three types of respiratory diseases (bronchitis, emphysema and chronic obstructive pulmonary diseases) significantly among children. A high prevalence of obstructive airway disease has a direct association with industrial pollution in Sri Lanka [36]. Researchers had observed that there would be a high tendency of increasing asthma with the exposure to the dust at home (for children of 5-11 years of age) [3].
Exposure to IAP from solid fuels causes chronic and acute diseases (such as cardiovascular diseases, cataracts, adverse perinatal health outcomes, acute respiratory tuberculosis, asthma, pneumonia) while cancer and other long term latency may occur due to its long term exposure [13]. IAP steers to chronic pulmonary disease (COPD) in adults and acute lower respiratory infections (ALRI) among children of five years [13]. Further, approximately 37% of the burden of disease from solid fuel (DALYs) occur in SAR [37].
Biomass burning is a major reason for the morbidity of SAR. Sri Lanka is also facing a burden of diseases due to IAP [8] but the risk is less than that of India, Bangladesh, Pakistan and Nepal [26]. Globally, the largest number of blindness cases due to biomass burning exposure has reported from India as well as more cataracts cases [8]. Further, most people from various locations, genders, as well as age groups, has reported as victims (with respiratory and non-respiratory diseases) of IAP significantly with biomass burning in India [8]. About 65 million cases of morbidity from respiratory diseases due to air pollution is recorded in India [38]. Rana et al. [39] reports that most of the children (under age of five) (70.2% of 27565 samples) in Afghanistan suffer from ARI due to spend more time with their mothers while cooking with solid fuels with unclean cooking stoves and kitchen inside that cause a vast IAP. In Bangladesh, it is increased the relative risk of COPD, cardiovascular disease (CVD) in adult females with long term exposure to indoor PM2.5 from traditional unventilated stoves [8]. Previous studies are reported an estimation of a 4.3% increase in CVD deaths in Delhi, India with exposure to both indoor and outdoor suspended particulates (an increase of 100 µg) and a positive coefficient for SO2 [40]. Smith [41] states that about 400-500 thousand premature deaths can be accredited annually due to use unclean fuels by (about three-quarter of) Indian households with respect to applying resulting risks with consideration of existing epidemiological studies prevail in India. Mortality rates and the respiratory and non-respiratory diseases were highly increasing with appalling rates in India, Nepal and Bangladesh indicating the paramount cause would be the conventional biomass burning [8]. A research study performed using 10 cluster of homes (Mirpur, Dhaka) in Bangladesh has convinced that the biomass burning in indoors could be affected several homes in the community causing pneumonia and other respiratory diseases with exposure to PMs and CO resulted unclean fuel combustion majorly while cooking [42].
Lead (Pb) causes adverse health problems in almost every human being without considering the age limit. Lead has 50 days in soft tissue while having a half-life of 25 days in the bloodstream [43]. In Sri Lanka, evidence has proved that the people living in traffic congested areas approach the toxic levels of blood lead concentrations [43]. When OAP arises it would be drastically affected to the households occuring IAP (due to air exchaging rate increases from outdoors to indoors) who lives in less-ventilated homes in subburban areas. A series of epidemiological studies have proved the strong connection between lung cancers and indoor Radon [21].
A finite number of epidemiological studies have been investigated the facts on health effects related to air quality in Sri Lanka [4,44]. Thus, several studies had proved the association of IAP with non-respiratory diseases such that low birth weight of infants due to the exposure to biomass fuels during the pregnancy and also neural tube defects, the neurodevelopmental performance of school children, cardiovascular diseases, cataracts, diabetes [4]. Sri Lanka owns a considerable burden of stillbirths and neonatal deaths like many other developing countries proving that pregnant mothers and unborn babies undergo additional risks from the exposures to burning biofuels and IAP [13].
Recent epidemiological meta-analysis reported, Parental smoking; Second-Hand Smoking (SHS) severely has an association with the occurrence of middle ear infection in children [4]. Studies prove that the Maternal factor, such that exposure to SHS significantly has a connection with Low Birth Weight (LBW) in developing countries. About 22% of Sri Lankan infants are born with LBW [33]. Khan et al. [45] reports that according to the analysis of Bangladesh national data, Acute Respiratory Infection (ARI), LBW and caesarean delivery are the most significant factors due to household air pollution occurring as a result of cooking indoors and using solid fuels amidst less necessary stove ventilation. In Bangladesh, 30% of children under age 5-year-old were stunted according to the study conducted by Goyal et al. [46] using the Bangladesh Demographic and Health Survey information (204-2014). Also concluded that the PM2.5 exposures at maternal period leads to the child anthropometric failure (stunting, wasting, underweight, LBW) significantly [46]. Khan et al. [15] convince that the major reason for ARI symptoms in children (of age under 5) in Pakistan is the usage of polluting fuels in households according to the study of the cross sectional data from Pakistan DHS 2012-2013. Rahut et al. [47] ensures the higher using domestic dirty fuel influences the higher amount of health impacts (tuberculosis, eye diseases, skin diseases) in Bhutan according to the survey study.
In comparison with other South Asian neighboring countries, Sri Lanka stands at a good position in having a favorably good public health status [8], frequently in a similar profile with solid fuel usage in both indoor and outdoor air pollution. Probably it may help in mitigating adverse health problem in exposures to air pollution such that better immunization coverage, better nutrition indicators, widely accessible and well established public health system etc. [4].
IAP and Economic Cost
Air pollution is not just a health risk but also a drag on development because illness and premature death reduce the quality of life and it causes a loss of productive labor directly, which mainly affects the economy of a country. The expenses can be due to personal or institutional health costs (medical costs, nursing care, drugs, etc.), productivity loss due to absence from work or inefficiency, etc. [1]. Further, the estimations reveal that indoor air pollution due to cooking with solid fuels were the major cause of loss in SAR [48].
In fact, the estimated total “lost income” is more than $66 billion (equivalent to nearly 1% of GDP) for the SAR countries from air pollution in 2013 [48]. The World Bank reported that the air pollution costs have grown such that the welfare losses were nearly doubled and labor income losses increased by 40% from 1990 to 2013 globally although the countries achieved the great gain in economic development and health outcome [48]. Pakistan attributes a cost about 1% of GDP annually due to ill-health of population resulted from IAP [24].
It can be termed that there is a burden on economic status in SAR due to prevailing health outcomes that are directly attributable to IAP as developing countries proving that IAP is more serious.
Minimize IAP Effects
In 2018, WHO published facts in case of helping regional and national policymakers to mitigate the environmental risk to public health due to air pollution. Table 2 states the most affiliated facts relating to IAP.
Modifying and enforcing the existing laws and introducing new laws, strict household and community regulations, robust research studies would be a strongly beneficial role in mitigating the impacts of air pollution [1]. The air quality of a country can be improved through an optimum strategic urban planning process in the long run by strategic location of polluting sources and exposed population, also encouraging a city structure that would minimize pollution emissions [49]. Unfortunately, urban regulations in SAR have historically contributed to misallocation of land use and growth of urban shapes that are not necessarily conducive to both air quality improvement and economic development [50].
Installing an optimum ventilation schema is the productive measure to avert from IAP such that introducing mechanical ventilation systems and increasing outdoor exchange rate in presence of less OAP [9]. Physical-chemical technologies (e.g., Filters) and biological based purification methods (biotechnologies) are used for mitigating IAP [9]. Sufficient controlling of indoor humidity and temperature would assist to control the emissions of organic pollutants from indoor materials [9]. Biotechnologies has been appeared as a sustainable and modest platform at present.
Using improved cooking stoves (“Anagi”-initially promoted by CEB since 1991 in Sri Lanka [4]) instead of traditional cooking stoves, better construction of houses with optimum ventilation, using of clean fuels (gas or Liquefied Petroleum Gas (LPG), Biogas, Solar cookers, electricity) [8,11] and conducting public awareness programs on maintaining the air quality among physicians, health administrators and primary health care workers [4] of the country may useful specifically in minimizing exposure to air pollutants by performing preventive activities in the society. The improvement of socio-economic conditions is mostly having a strong connection to mitigating air pollution [1].
In Sri Lanka, the National Authority on Tobacco and Alcohol Act No. 27 of 2006 properly takes actions to regulate public tobacco smoking to prevent SHS [50]. Some South Asian countries have implemented partial or comprehensive smoke-free policy nation-wide; Bangladesh (2005), Bhutan (2004), India (2008) respectively [17].
Energy ladder (Figure 3) showcase the relationship between socio economic status and the energy efficiency. The poorer households rely on primitive fuels while others consume higher ranked fuel types and mostly, switching of fuel types respectively from primitive, transition and advanced fuels are affected the factors of human capital, labour economy, household income, culturul backgrounds and cost levels of fuels [51].
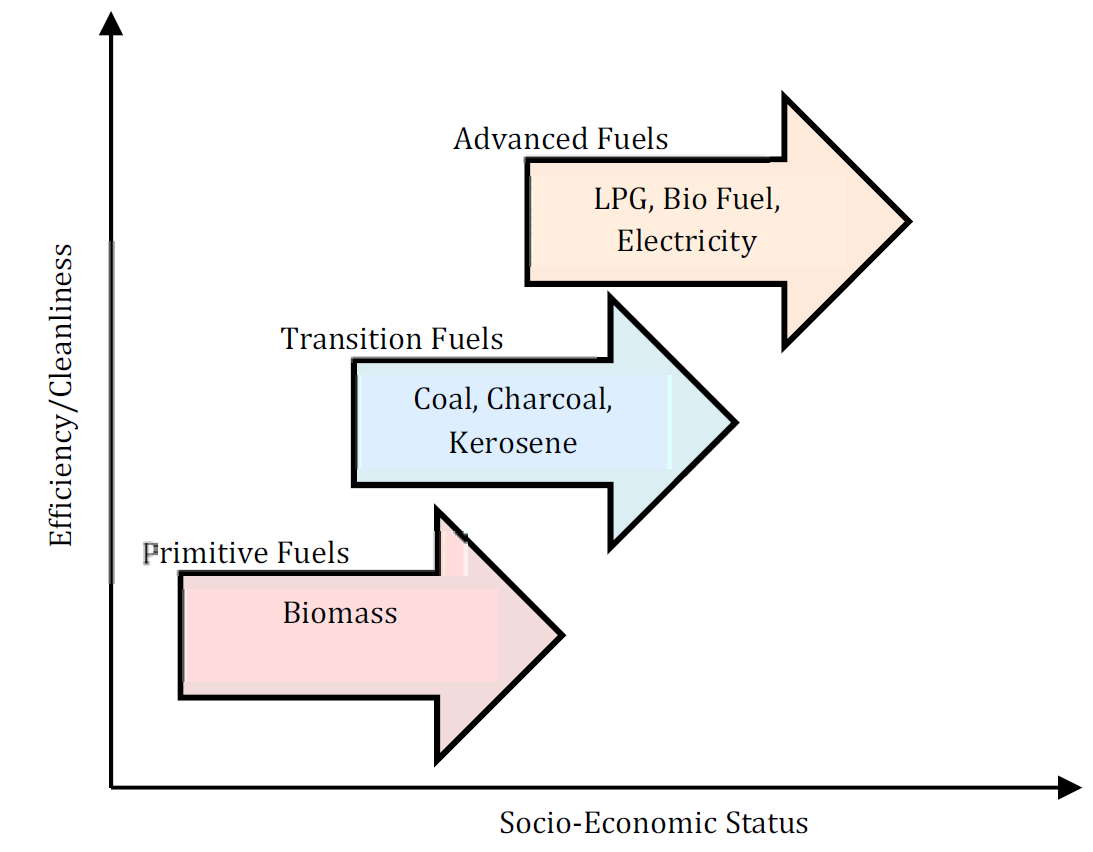
Figure 3: Energy Ladder [54]
In Pakistan, “Clean Fuel” Scenario (CFS) was implemented to broaden the clean fuel usage with the clean air concept by replacing solid fuels with LPG, substitute gasoline and diesel oil to CNG in transport sector and introducing gas-fired power plants by 2020 [52]. Bhutan is significantly producing hydro-electric power ensuring people to use renewable energy for their daily needs (cooking, heating, lighting) in recent years progressively as the household energy sources mainly effect for the socio-economic and sustainable development in a country [47]. Existing political platforms, such as South Asian Association for Regional Cooperation should be authorized and leveraged to perform the action plans for the betterment of air quality [7].
Bhutan, Maldives, Sri Lanka remain somewhat optimum level in national air quality among all other countries in SAR. Almost all action plans generally indicate the overall suggestions of the strategies simply such that transferring towards clean fuels, maintain emissions inventory, developing environmentally viable infrastructure systems, establishing efficient air quality monitoring stations, managing household air pollution technically through social interventions, monitoring the power plant efficiency and industrial sector viability to mitigating air pollution etc.
Table 2: Successful Policies Proposed by WHO for Mitigating Air Pollution [53]
Successful policies in: | |
Industry |
|
Energy |
|
Power Generation |
|
Though Sri Lanka stands at an optimum stage of the IAQ when compared to that of other countries in SAR, it is far behind in the world. Sri Lanka comes up with a considerable disease burden due to IAP, yet less in relation to most other SAR Countries (India, Pakistan, Bangladesh, Nepal). Most of the epidemiological studies suggest many satisfactory pieces of evidence for it. Bangladesh, India, Nepal, Pakistan also has a strong disease burden due to air pollution. The Maldives plays a relative stage overall. Also lacking many robust studies on IAP here in Sri Lanka except accessing health outcomes. Enactment of new legislation, enforcing the existing, national action plan and raising public awareness (knowledge) of the problem is highly needed to mitigate the effects of IAP in Sri Lanka as well as in other South Asian countries towards the sustainable stability of the country. Using clean fuels and improved stoves, omitting smoking in indoors as well as upgrade ventilation schema in households would potentially help to well-being of public by shielding IAP flaws. Robust researches and modelling studies should be developed to investigate the evolution of indoor air pollution in order to uplift the air quality in indoors in South Asia.
Acknowledgment
This study is supported by the University Research Grant, Faculty of Technology, University of Sri Jayewardenepura, Sri Lanka. (Grant No: ASP/01/RE/FOT/2017/76).
Nandasena, S. et al. “Air Pollution and Public Health in Developing Countries: Is Sri Lanka Different?” Journal of the College of Community Physicians of Sri Lanka, vol. 17, 2012.
Jacquemin, B. et al. “Air Pollution and Asthma Control in the Epidemiological Study on the Genetics and Environment of Asthma.” Journal of Epidemiology & Community Health, vol. 66, no. 9, 2012, pp. 796-802.
Karunasekera, K.A.W. et al. “Genetic and Environmental Risk for Asthma in Children Aged 5-11 Years.” Sri Lanka Journal of Child Health, vol. 34, 2009.
Nandasena, S. et al. “Respiratory Health Status of Children from Two Different Air Pollution Exposure Settings of Sri Lanka: A Cross-Sectional Study.” American Journal of Industrial Medicine, vol. 55, no. 12, 2012, pp. 1137-1145.
Ileperuma, O.A. “Review of Air Pollution Studies in Sri Lanka.” Ceylon Journal of Science, vol. 49, no. 3, 2020, pp. 225-238.
WHO. Air Quality Guidelines for Particulate Matter, Ozone, Nitrogen Dioxide and Sulfur Dioxide: Global Update 2005. 2005, https://apps.who.int/iris/bitstream/handle/106 65/69477/WHO_SDE_PHE_OEH_06.02_eng.pdf.
Begum, B. “Tackling the Health Burden of Air Pollution in South Asia.” The BMJ, vol. 359, 2017.
Junaid, M. et al. “Status of Indoor Air Pollution (IAP) through Particulate Matter (PM) Emissions and Associated Health Concerns in South Asia.” Chemosphere, vol. 191, 2018, pp. 651-663.
González-Martín, J. et al. “A State-of-the-Art Review on Indoor Air Pollution and Strategies for Indoor Air Pollution Control.” Chemosphere, vol. 262, 2021.
WHO. Air Pollution. 2021, https://www.who.int/health-topics/air-pollution#tab=tab_1.
WHO. WHO Indoor Air Quality Guidelines: Household Fuel Combustion. 2014b, https://apps.who.int/iris/bitstream/ handle/10665/141496/9789241548885_eng.pdf.
Elledge, M.F.P. et al. “A Profile of Biomass Stove Use in Sri Lanka.” International Journal of Environmental Research and Public Health, vol. 9, no. 4, 2012.
Elledge, M. et al. “Environmental Health Risk and the Use of Biomass Stoves in Sri Lanka.” RTI Press, 2010.
Chartier, R. et al. “A Comparative Study of Human Exposures to Household Air Pollution from Commonly Used Cookstoves in Sri Lanka.” Indoor Air, vol. 27, no. 1, 2017, pp. 147-159.
Khan, M.S.B. and H.D. Lohano. “Household Air Pollution from Cooking Fuel and Respiratory Health Risks for Children in Pakistan.” Environmental Science and Pollution Research, vol. 25, no. 25, 2018, pp. 24778-24786.
Abdulla, N.I. “Climate Change and Health in Maldives: Protecting Our Common Future.” WHO South-East Asia Journal of Public Health, vol. 6, no. 2, 2017.
Lee, J. et al. “Secondhand Smoke Exposures in Indoor Public Places in Seven Asian Countries.” International Journal of Hygiene and Environmental Health, vol. 213, no. 5, 2010, pp. 348-351.
WHO. Population with Primary Reliance on Polluting Fuels and Technologies for Cooking (in Millions). 2018b, https://www.who.int/data/gho/data/indicators/indicator-details/GHO/population-with-primary-reliance-on-polluting-fuels-and-technologies-for-cooking-(in-millions).
Alagiyawanna, A.M.A.A.P. et al. “Prevalence and Correlates of Exposure to Secondhand Smoke (SHS) among 14 to 15-Year-Old Schoolchildren in a Medical Officer of Health Area in Sri Lanka.” BMC Public Health, vol. 18, no. 1, 2018.
Nafees, A.A. et al. “Indoor Air Pollution (PM2.5) Due to Secondhand Smoke in Selected Hospitality and Entertainment Venues of Karachi, Pakistan.” Tobacco Control, vol. 21, no. 5, 2012, pp. 460-464.
WHO. WHO Guidelines for Indoor Air Quality: Selected Pollutants. 2010, https://apps.who.int/iris/handle/106 65/260127.
Pitawala, H.M.T.G. et al. “Chemical Characterization of Household Dust in Two Major Cities: Colombo, the Capital and Kandy, the Hill Capital, Sri Lanka.” Carpathian Journal of Earth and Environmental Sciences, vol. 8, 2013, pp. 89-95.
WHO. Household Air Pollution DALYs (per 100,000 Population). 2016, https://www.who.int/data/gho/ data/indicators/indicator-details/GHO/household-air-pollution-attributable-dalys-(per-100-000-population)-.
Nasir, Z.A. et al. “Role of Poverty in Fuel Choice and Exposure to Indoor Air Pollution in Pakistan.” Journal of Integrative Environmental Sciences, vol. 12, no. 2, 2015, pp. 107-117.
WHO. Health Aspects of Air Pollution: Results from the WHO Project ‘Systematic Review of Health Aspects of Air Pollution in Europe’. Copenhagen: WHO Regional Office for Europe, 2004.
Cohen, A.J. et al. “Estimates and 25-Year Trends of the Global Burden of Disease Attributable to Ambient Air Pollution: An Analysis of Data from the Global Burden of Diseases Study 2015.” Lancet, vol. 389, no. 10082, 2017, pp. 1907-1918.
Phillips, M.J. et al. “Sri Lanka Pilot Study to Examine Respiratory Health Effects and Personal PM2.5 Exposures from Cooking Indoors.” n.p., vol. 13, no. 8, 2016.
Ranathunga, N. et al. “Effect of Household Air Pollution Due to Solid Fuel Combustion on Childhood Respiratory Diseases in a Semi Urban Population in Sri Lanka.” BMC Pediatrics, vol. 19, no. 1, 2019.
HEI. Health Effects of Outdoor Air Pollution in Developing Countries of Asia: A Literature Review. Boston, MA, 2004, https://www.healtheffects.org/system/files/SpecialReport15.pdf.
EPA. Criteria Air Pollutants. 2020, https://www.epa.gov/ criteria-air-pollutants.
WHO. WHO Guidelines for Indoor Air Quality: Household Fuel Combustion. Geneva, 2014a.
Senarath, C. An Overview of Air Pollution and Respiratory Illnesses in Sri Lanka. York University, 2005.
Tran, V.V. et al. “Indoor Air Pollution, Related Human Diseases, and Recent Trends in the Control and Improvement of Indoor Air Quality.” International Journal of Environmental Research and Public Health, vol. 17, no. 8, 2020.
Nandasena, S. et al. “Indoor Air Pollution and Respiratory Health of Children in the Developing World.” World Journal of Clinical Pediatrics, vol. 2, no. 2, 2013, pp. 6-15.
Dharshana, Thishan K.G. and N. Coowanitwong. “Ambient PM10 and Respiratory Illnesses in Colombo City, Sri Lanka.” Journal of Environmental Science and Health, Part A, vol. 43, no. 9, 2008, pp. 1064-1070.
Premaratna, R. et al. “Effects of Pollution on Health of Residents in an Industrial Area in Sri Lanka.” Archives of Environmental Health, vol. 57, no. 6, 2002, pp. 579-583.
Bruce, N. et al. “Indoor Air Pollution.” Disease Control Priorities in Developing Countries, edited by Jamison, D.T. et al., The World Bank and Oxford University Press, 2006.
Ghaffar, A. et al. “Burden of Non-Communicable Diseases in South Asia.” BMJ (Clinical Research Ed.), vol. 328, no. 7443, 2004, pp. 807-810.
Rana, J. et al. “Associations between Indoor Air Pollution and Acute Respiratory Infections among Under-Five Children in Afghanistan: Do SES and Sex Matter?” International Journal of Environmental Research and Public Health, vol. 16, no. 16, 2019.
Yamamoto, S.S. et al. “A Systematic Review of Air Pollution as a Risk Factor for Cardiovascular Disease in South Asia: Limited Evidence from India and Pakistan.” International Journal of Hygiene and Environmental Health, vol. 217, nos. 2-3, 2014, pp. 133-144.
Smith, K.R. “National Burden of Disease in India from Indoor Air Pollution.” PNAS, vol. 97, 2000.
Weaver, A.M. et al. “Air Pollution Dispersion from Biomass Stoves to Neighboring Homes in Mirpur, Dhaka, Bangladesh.” BMC Public Health, vol. 19, no. 1, 2019.
Senanayake, M.P. et al. “Blood Lead Levels of Children before and after Introduction of Unleaded Petrol.” Ceylon Medical Journal, vol. 49, no. 2, 2004, pp. 60-61.
Senanayake, M. et al. “A Relational Analysis of Acute Wheezing and Air Pollution.” Sri Lanka Journal of Child Health, vol. 30, 2009.
Khan, M.N.B. et al. “Household Air Pollution from Cooking and Risk of Adverse Health and Birth Outcomes in Bangladesh: A Nationwide Population-Based Study.” Environmental Health, vol. 16, no. 1, 2017.
Goyal, N. and D. Canning. “Exposure to Ambient Fine Particulate Air Pollution in Utero as a Risk Factor for Child Stunting in Bangladesh.” International Journal of Environmental Research and Public Health, vol. 15, no. 1, 2018.
Rahut, D.B. et al. “Domestic Use of Dirty Energy and Its Effects on Human Health: Empirical Evidence from Bhutan.” International Journal of Sustainable Energy, vol. 36, no. 10, 2017, pp. 983-993.
World Bank. The Cost of Air Pollution: Strengthening the Economic Case for Action. Washington, DC, 2016, https://openknowledge.worldbank.org/handle/10986/25013.
World Bank Group. Urban Planning and Air Quality. 2002, http://documents1.worldbank.org/curated/en/515081468101343461/pdf/multi0page.pdf.
WHO. Global Youth Tobacco Survey (GYTS), Sri Lanka: Country Report. 2015, https://extranet.who.int/ncdsmicro data/index.php/catalog/226/related_materials.
Van der Kroon, B. et al. “The Energy Ladder: Theoretical Myth or Empirical Truth? Results from a Meta-Analysis.” Renewable and Sustainable Energy Reviews, vol. 20, 2013, pp. 504-513.
Purohit, P. et al. “Scenario Analysis of Strategies to Control Air Pollution in Pakistan.” Journal of Integrative Environmental Sciences, vol. 10, no. 2, 2013, pp. 77-91.
WHO. Ambient (Outdoor) Air Pollution. 2018a, https:// www.who.int/news-room/fact-sheets/detail/ambient-(outdoor)-air-quality-and-health.
Fatmi, Z. “Biomass Fuel and Coronary Heart Disease among Women in Pakistan.” n.p., 2017.
