+91 6002993949
submission@iarconsortium.org
Open Access
ISSN (Print) : 2789-6056
ISSN (Online) : 2789-6064
Introduction: Organophosphorus compounds (OPCs), widely used in agriculture and households, are a major cause of poisoning-related deaths, especially in developing countries like India. The severity of poisoning depends on the compound type, dose and treatment timing, making early intervention essential for better outcomes. Materials and Methods: This prospective study at MGM Medical College (Sept 2022–June 2024) included 70 OPC poisoning patients, categorized into ventilatory and non-ventilatory groups. Data on demographics, clinical symptoms, GCS scores and lab parameters were collected. Standard treatment protocols were followed and SPSS version 26 was used for statistical analysis. Results: OP poisoning predominantly affected younger individuals, with 64.28% of cases under 40 years and females (55.71%) were more affected than males (44.28%). Housewives (31.42%) were the most affected occupational group and suicidal intent was the primary cause (81.42%). Malathion (25.71%) was the most commonly consumed OP compound. Nausea and vomiting were the most common symptoms (74.28%), while respiratory failure occurred in 51.42% of cases. Moderate to severe impairment was prevalent, with 54.28% of patients having a GCS score of 8-11 and 35.71% scoring below 8. The majority had serum cholinesterase levels of 2001-5000 IU/L (55.71%), while 35.71% had significant inhibition (1001-2000 IU/L). Mechanical ventilation was significantly associated with delayed hospitalization (p=0.012), respiratory failure (p=0.032), fasciculations (p=0.001), low GCS scores (p=0.001) and reduced serum cholinesterase levels (p=0.028), while age, sex and pinpoint pupils showed no significant correlation. Outcomes varied, with 68.57% being discharged, 24.28% dying and 7.14% leaving against medical advice, reflecting the severity and variability in recovery patterns among OP poisoning cases. Conclusion: Our study highlights the critical role of mechanical ventilation, GCS scores, serum cholinesterase and amylase levels in determining OP poisoning outcomes. Patients with severe respiratory failure and low GCS scores had higher mortality, emphasizing the need for early intervention and intensive medical care to improve survival rates.
Organophosphorus compounds (OPCs) find extensive use as pesticides, not only in agricultural and horticultural settings but also in households for combating vector-borne diseases like malaria and dengue. This prevalent usage contributes significantly to the global burden of pesticide poisoning, resulting in approximately 200,000 deaths in developing countries [1]. The World Health Organization (WHO) reported 193,460 deaths worldwide in 2012 due to unintentional poisoning, with an additional 370,000 deaths attributed to suicidal pesticide poisoning [2]. Rural areas in Asia, particularly in India, bear a disproportionate share of this issue, with Southern and Central India experiencing higher instances of OPC poisoning-related deaths [3]. The easy accessibility of OPCs makes them a common choice for self-harm, constituting a notable percentage of suicidal poisoning cases in India, ranging from 10.3% to 43.8% according to various studies [4].
Understanding the factors that drive the choice between ventilatory and non-ventilatory support is crucial for optimizing patient care and improving outcomes in cases of organophosphorus compound poisoning. Factors such as the time of exposure, the type and amount of the toxic agent, individual patient characteristics and the availability of medical resources all play integral roles in shaping the clinical course.
This prospective comparative study was conducted at MGM Medical College, Kamothe, Navi Mumbai, over a period from September 2022 to June 2024. The study aimed to compare the clinical outcomes of patients with organophosphorus compound (OPC) poisoning who required ventilatory support to those who did not. Patients were categorized into two groups based on their need for mechanical ventilation. The study adhered to standard clinical protocols for the management of OPC poisoning, including administration of antidotes, supportive care and ventilatory assistance when required. Ethical approval was obtained from the institutional review board and informed consent was obtained from all participants before inclusion.
A total of 70 patients diagnosed with OPC poisoning and admitted to MGM Medical College were recruited. The inclusion criteria required patients to be above 18 years of age, of either sex and diagnosed with OPC poisoning. Exclusion criteria included patients under 18 years of age, poisonings other than OPC, history of chronic lung disease (such as asthma, emphysema or tuberculosis) and snake bite patients. Eligible patients were randomly assigned to either the ventilatory support group or the non-ventilatory support group using a computer-generated randomization list. The allocation was concealed using sealed opaque envelopes to prevent selection bias. To ensure statistical power, a sample size of 67 patients was determined based on prevalence rates and a 10% margin of error, with additional patients included to compensate for dropouts.
Data Collection and Monitoring
Data collection was carried out using a pre-designed and validated research tool. Demographic details such as age, sex and time since exposure were recorded. Clinical parameters included Glasgow Coma Scale (GCS) score, vital signs (blood pressure, heart rate, respiratory rate) and specific symptoms such as salivation, lacrimation, urination, defecation, gastrointestinal distress and emesis (SLUDGE syndrome). Laboratory investigations included arterial blood gas (ABG) analysis, serum cholinesterase levels and oxygen saturation measurements. Patients were monitored intensively for signs of respiratory insufficiency using parameters such as breathlessness, respiratory rate, accessory muscle action, pulse oximetry readings and ABG findings. Those showing signs of respiratory distress were provided with ventilatory support as per the hospital’s protocol.
Intervention and Treatment Protocol
Patients were managed according to standard clinical guidelines for OPC poisoning, which included the administration of injection atropine and injection pralidoxime. Gastric lavage and decontamination were performed in all patients. Supportive care included oxygen therapy, intravenous fluids and symptomatic treatment. For patients requiring ventilatory support, endotracheal intubation and mechanical ventilation were initiated, with ventilatory settings adjusted based on clinical and ABG parameters. Indications for mechanical ventilation included cardiorespiratory arrest, inability to protect the airway, severe metabolic acidosis and poor gas exchange despite oxygen therapy. Ventilatory support was provided using synchronized intermittent mandatory ventilation (SIMV) with pressure support. Positive end-expiratory pressure (PEEP) was adjusted to maintain oxygen saturation above 94% and weaning from mechanical ventilation was carried out using pressure support weaning and T-piece trials.
Statistical Analysis
The collected data were entered into MS Excel and analyzed using SPSS version 26. Descriptive statistics such as mean, mode, median, frequencies and percentages were used for basic data analysis. Continuous data were analyzed using parametric tests like the independent t-test, while categorical data were analyzed using non-parametric tests such as the Chi-square test. A significance level of 0.05 was set for all statistical tests. Ethical considerations were strictly followed, ensuring patient confidentiality and obtaining informed consent from all participants. The study aimed to identify factors leading to the need for ventilatory support in OPC poisoning cases, potentially improving early intervention strategies and optimizing patient management to reduce ventilatory dependency.
OP poisoning predominantly affected younger individuals, with 64.28% of cases under 40 years. The highest incidence was in the <30 age group (34.28%), followed by 30-39 years (30%). Older patients (≥60 years) were rare, comprising only 4.27% of cases. Females (55.71%) were more affected than males (44.28%), indicating a slightly higher prevalence of OP poisoning among women. Housewives (31.42%) were the most affected occupational group, followed by laborers (25.71%) and farmers (18.57%). Suicidal intent was the primary cause (81.42%), while accidental poisoning accounted for 18.57%. Regarding hospital admission time, 38.16% arrived within 6 hours, 32.89% between 6-9 hours and 9.21% after 9 hours. Malathion (25.71%) was the most commonly consumed OP compound, followed by Methyl Parathion (14.28%) and Monocrotphos (12.85%) (Table 1).
Nausea and vomiting were the most common symptoms (74.28%), followed by excessive salivation and abdominal cramps (41.42% each). Respiratory failure was observed in 51.42% of cases, while pin-point pupils were noted in 67.14%. Regarding consciousness, 54.28% had a GCS score of 8-11, 35.71% scored below 8 and only 10% had a GCS of 12-15, indicating a high prevalence of moderate to severe impairment. The majority of OP poisoning patients had serum cholinesterase levels of 2001-5000 IU/L (55.71%), while 35.71% had significant inhibition (1001-2000 IU/L) and 5.71% showed severe inhibition (<1000 IU/L).
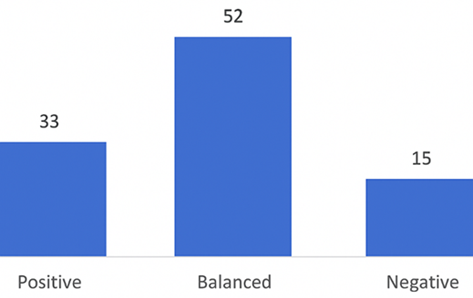
Figure 1: Outcome of OP Poisoning patients
Table 1: Distribution of patients according to type of compound consumed
Type of Compound | Frequency (n) | Percentage |
Diazinon | 6 | 8.57% |
Chlorpyriphos | 2 | 2.85% |
Dichlorovas | 8 | 11.42% |
Dimethoate | 6 | 8.57% |
Malathion | 18 | 25.71% |
Methyl Parathion | 10 | 14.28% |
Monocrotphos | 9 | 12.85% |
Phenylphyrazole | 1 | 1.42% |
Phorate | 1 | 1.42% |
Phosphonic Acid | 1 | 1.42% |
Quinphos | 1 | 1.42% |
Other | 7 | 10.00% |
Total | 70 | 100% |
Table 2: Factors associated with mechanical ventilation in op poisoning
| Factor | Required Ventilation (%) | Not Required (%) | p-value |
| Age Group (<30 to >50) | 34.28% - 11.42% | Varies | 0.520 |
| Sex (Male vs Female) | 45.71% (M) / 54.28% (F) | 42.85% (M) / 57.14% (F) | 0.124 |
| Time to Hospitalization (>9 hrs) | 25.71% (>9 hrs) | 51.42% (<6 hrs) | 0.012 |
| Pinpoint Pupils | 65.71% | 54.28% | 0.072 |
| Respiratory Failure | 77.14% | 22.85% | 0.032 |
| Fasciculations | 31.42% | 2.85% | 0.001 |
| GCS Score (<8) | 68.57% | 2.85% (12-15 GCS) | 0.001 |
| Serum Cholinesterase (<1000 IU/L) | 11.42% (<1000) | 2.85% (>5000) | 0.028 |
| Outcome (Death vs. Discharge) | 40% (Died) / 54.28% (Discharged) | 8.57% (Died) / 82.85% (Discharged) | 0.032 |
This table summarizes the key factors influencing mechanical ventilation in OP poisoning cases, highlighting significant associations with delayed hospitalization (p=0.012), respiratory failure (p=0.032), fasciculations (p=0.001), low GCS scores (p=0.001) and reduced serum cholinesterase levels (p=0.028) and mortality. Age, sex and pinpoint pupils showed no significant correlation (p>0.05) (Table 2).
In our study, atropine administration varied across time points, with 40% receiving less than 30 mg on arrival, 50% receiving less than 100 mg within the first 48 hours and 48.57% receiving 30-79 mg in the following 48 hours. Injection PAM was given to 90% of patients, while 10% were treated symptomatically due to unclassified substances. Regarding outcomes, 68.57% were discharged, 24.28% died and 7.14% left against medical advice (DAMA), highlighting varied recovery patterns in OP poisoning cases.
Self-poisoning with organophosphorus (OP) compounds is a significant public health issue in many agricultural regions, particularly in rural parts of developing countries like India. These regions see a high incidence of OP poisoning due to the widespread availability and use of these pesticides in agriculture. Respiratory failure remains the leading cause of mortality in OP poisoning cases [4,5].
The intent behind OP poisoning in our study revealed a significant majority with suicidal intentions, constituting 81.42% of cases, while accidental poisoning accounted for 18.57%. This overwhelming prevalence of suicidal intent underscores the critical need for mental health interventions and suicide prevention strategies in populations affected by OP poisoning. Similar trends were observed in other studies. Twayana et al. [6] found that 74.5% of OP poisoning cases were due to suicidal attempts, with significant factors including household conflict and depressive illness. This aligns with our findings and highlights the role of socio-economic and mental health issues in suicidal OP poisoning.
In our study, a notable trend was observed regarding the time lapse between poisoning and hospital admission among patients requiring mechanical ventilation. A study by Eddleston et al. [7] found that early intervention was crucial for patient survival, with many patients intubated within 2 hours of admission due to acute cholinergic features, highlighting the importance of rapid response. Rajeev and Arvind [8] also identified the time lag from poison consumption to treatment as a significant predictor for the need for ventilator support, suggesting that timely intervention can reduce mortality.
In our study, the majority of OP poisoning cases involved Malathion, accounting for 25.71% of patients. Comparatively, other studies highlight similar trends in the prevalence of specific OP compounds. Thunga et al. [9] found that Methyl Parathion was the most commonly ingested compound in their study at Kasturba Hospital, Manipal, accounting for 30% of cases. Kamath et al. [3] reported a high incidence of poisoning due to Monocrotophos, mirroring our observation of its prevalence. Ahmed et al. [10] identified Methamidophos and Dichlorvos as the most common agents, differing slightly from our findings where Malathion was predominant. Patil et al. [11] reported a range of OP compounds with notable mentions of Malathion and Monocrotophos, supporting our data. Additionally, Rajeev and Arvind [8] highlighted the frequent use of Chlorpyriphos in their study, which aligns with our observation of its presence, albeit in smaller proportions.
In our study, the majority of OP poisoning patients exhibited moderate to severe impairment of consciousness, with 54.28% scoring between 8 and 11 on the Glasgow Coma Scale (GCS) and 35.71% scoring below 8, indicating severe impairment. These findings align with studies by Sudha Mary Philip [12] and Datla et al. [13], which identified lower GCS scores as strong predictors of mechanical ventilation need, reinforcing the severity of OP poisoning effects on consciousness. Research by Prakash et al. [14] and Farooqui et al. [15] also supports this, linking lower GCS scores to higher mortality rates, highlighting the necessity for early monitoring and intervention. Similarly, serum cholinesterase levels in our study varied significantly, with 55.71% falling between 2001-5000 IU/L and 53.71% between 1001-2000 IU/L, suggesting moderate to significant enzyme inhibition. Comparatively, Shetti et al. [16] and Rajeev & Arvind8 found that lower cholinesterase levels correlated with increased mechanical ventilation needs and prolonged ICU stays, confirming that enzyme inhibition severity plays a key role in prognosis. Ahmed et al. [10], Patil et al. [11] and Madala et al. [17] further supported this by linking low cholinesterase levels to severe clinical outcomes and increased mortality, reinforcing its importance as a prognostic marker.
Additionally, serum amylase levels were assessed to evaluate pancreatic function, with 75.71% of patients exhibiting elevated levels above 140 U/L, indicating potential pancreatic involvement. This finding aligns with studies by Sudha Mary Philip, Thunga et al. [9] and Ahmed et al. [10], all of which highlight the association between elevated amylase levels and pancreatic stress or injury in OP poisoning cases. Research by Rajeev and Arvind [8] further supports the idea that elevated amylase correlates with increased morbidity, underscoring its role in identifying patients at higher risk of complications. Overall, the consistent findings across multiple studies emphasize the critical role of GCS, cholinesterase and amylase levels in assessing OP poisoning severity. Lower GCS scores and cholinesterase levels were significantly associated with worse clinical outcomes, while elevated amylase levels highlighted potential pancreatic complications. These markers are essential for guiding treatment decisions, predicting prognosis and ensuring timely medical intervention in OP poisoning cases.
In our study, OP poisoning outcomes varied significantly, with 68.57% of patients being discharged, 24.28% succumbing to poisoning and 7.14% leaving against medical advice. Comparatively, studies such as those by Patil et al. [11] and Thunga et al. [9] reported similar mortality rates, reinforcing the severity of OP poisoning. The need for mechanical ventilation varied across age groups, with younger patients requiring it more frequently, a trend supported by studies from Gaspari [18], Hulse [19] and Farooqui [15], which found that younger patients often experienced more severe respiratory complications. No significant association was found between sex and ventilation requirements (p=0.124), aligning with findings from Thakur [20], Biradar and Prakash et al. [14], who emphasized that poisoning severity, rather than sex, was the primary determinant for ventilation. Respiratory failure was strongly linked to ventilation needs (77.14%, p=0.032), as also observed by Chintale [2], Prakash[14] and Ali et al. [21], highlighting the necessity for aggressive respiratory management. Lower GCS scores were significantly associated with ventilation needs (p=0.001), a finding consistent with studies by Farooqui[15], Philip[12] and Prakash [14], further supporting GCS as a crucial predictor for mechanical support.
Similarly, lower serum cholinesterase levels increased ventilation needs, with 51.42% of patients in the 1001-2000 IU/L range requiring it (p=0.028). This aligns with research from Datla[13], Hulse[19] and Thakur [20], who identified cholinesterase levels as key predictors of respiratory support. Elevated serum amylase levels were also linked to increased ventilation needs (p=0.033), consistent with studies by Prakash [14] and Thunga [9], which highlighted pancreatic involvement in severe OP poisoning cases. Mortality was significantly associated with ventilation (40% of deceased patients required it, p=0.032), a trend also observed by Prakash[14], Hulse [19] and Philip [12], emphasizing that mechanical ventilation is a strong predictor of poor prognosis. Collectively, these findings highlight the critical role of early intervention, monitoring of GCS, cholinesterase and amylase levels and timely respiratory management to improve patient outcomes in OP poisoning cases.
Our study has limitations, including a small sample size, single-center setting and potential data biases due to its retrospective nature. Variability in OP compound types and doses was not accounted for, which may affect poisoning severity and treatment outcomes.
Our findings emphasize the crucial role of mechanical ventilation, GCS scores, serum cholinesterase and amylase levels in OP poisoning prognosis. Higher mortality was significantly linked to respiratory failure and lower GCS scores, while cholinesterase inhibition and elevated amylase levels indicated severe poisoning requiring intensive care. Early recognition and aggressive management of these clinical indicators are essential to improving survival and treatment outcomes.
Eddleston, Michael et al. "Management of acute organophosphorus pesticide poisoning." The Lancet, vol. 371, no. 9612, 2008, pp. 597–607.
Chintale, K. N. and S. V. Patne. "Clinical profile of organophosphorus poisoning patients at rural tertiary health care centre." International Journal of Advanced Medicine, vol. 3, no. 2, 2016, pp. 268–274.
Kamath, S. D. and V. K. Gautam. "Study of organophosphorus compound poisoning in a tertiary care hospital and the role of Peradeniya Organophosphorus Poisoning scale as a prognostic marker of the outcome." Journal of Family Medicine and Primary Care, vol. 10, no. 11, 2021, p. 4160.
Dubey, T. et al. "Correlation of severity of organophosphorus poisoning as assessed by Peradeniya organophosphorus poisoning scale with serum amylase and CPK level." International Journal of Contemporary Medical Research, vol. 3, no. 9, 2016, pp. 2534–2537.
Blain, P. G. "Organophosphorus poisoning (acute)." BMJ Clinical Evidence, 2011, p. 2011.
Twayana, R. et al. "Clinical correlation of the severity and outcomes of the organophosphorus compound poisoning cases admitted to Kathmandu University Hospital based on POP score and serum pseudocholinesterase level—a prospective observational study in Nepal." International Journal of Internal and Emergency Medicine, vol. 2, no. 1, 2019, p. 1016.
Eddleston, Michael. "The pathophysiology of organophosphorus pesticide self-poisoning is not so simple." Netherlands Journal of Medicine, vol. 66, no. 4, 2008, pp. 146–148.
Rajeev, H. and M. Arvind. "Study of clinical and biochemical parameters in predicting the need for ventilator support in organophosphorus compound poisoning." Journal of Evolution of Medical and Dental Sciences, vol. 2, no. 49, 2013, pp. 9555–9571.
Thunga, G. et al. "Evaluation of incidence, clinical characteristics and management in organophosphorus poisoning patients in a tertiary care hospital." Journal of Toxicology and Environmental Health Sciences, vol. 2, no. 5, 2010, pp. 73–76.
Ahmed, S. M. et al. "Survival pattern in patients with acute organophosphate poisoning on mechanical ventilation: a retrospective intensive care unit-based study in a tertiary care teaching hospital." Indian Journal of Anaesthesia, vol. 58, no. 1, 2014, p. 11.
Patil, A. et al. "Profile of acute poisoning cases treated in a tertiary care hospital: a study in Navi Mumbai." 2014.
Philip, S. M. "Predicting the need for ventilatory support in organophosphorous compound poisoning." 2006.
Datla, A. V. et al. "A prospective study on the predictors of mechanical ventilation in organophosphate poisoning." 2020.
Prakash, S. and G. Ramamoorthy. "Clinical outcome of mechanically ventilated patients of organophosphorous compound poisoning." 2021.
Farooqui, W. A. et al. "Trajectories of vital status parameters and risk of mortality among acute organophosphorus poisoning patients—a latent class growth analysis." BMC Public Health, vol. 20, 2020, pp. 1–9.
Shetti, A. N. et al. "Correlation of serum acetylcholinesterase with the ventilation need, ICU stay and outcome in organophosphorus poisoning—a retrospective study." Anaesthesia, Pain and Intensive Care, 2019, pp. 199–203.
Madala, P. and M. S. Aravind. "Outcome of patients with OPC poisoning who require mechanical ventilation: a statistical analysis." International Journal of Advanced Medicine, vol. 4, no. 2, 2017, p. 357.
Gaspari, R. J. and D. Paydarfar. "Respiratory failure induced by acute organophosphate poisoning in rats: effects of vagotomy." Neurotoxicology, vol. 30, no. 2, 2009, pp. 298–304.
Hulse, E. J. et al. "Organophosphorus nerve agent poisoning: managing the poisoned patient." British Journal of Anaesthesia, vol. 123, no. 4, 2019, pp. 457–463.
Biradar, S. and V. Thakur. "Study of predictors for ventilatory support in patients of organophosphorus compound poisoning." 2018.
Ali, P. et al. "Clinical pattern and outcome of organophosphorus poisoning." Journal of Liaquat University of Medical and Health Sciences, vol. 11, no. 1, 2012, pp. 15–18.
