+91 6002993949
submission@iarconsortium.org
Open Access
ISSN (Print) : 2789-6056
ISSN (Online) : 2789-6064
One of the key obstetric conditions associated with an elevated risk of pre-term birth, morbidity and perinatal mortality is intrauterine growth restriction (IUGR) and cervical incompetence. Whereas all the conditions have been studied extensively in isolation, there is a dearth of evidence on the joint effect when the conditions are confronted together during the process of antenatal care and especially in resource-depleted conditions. This paper has discussed the relationship between cervical incompetence and incidence of IUGR, maternal and neonatal outcomes and the antenatal care. The cervical incompetence was detected whereby clinical history and transvaginal ultrasound measurement of cervical length detected cervical incompetence and the IUGR was determined using standardized foetal growth measures. Descriptive and multivariate statistical analyses were used to compare maternal demographic and obstetric data, ultrasound data and neonatal outcomes. The results revealed the prevalence of IUGR with complications in pregnancy, with cervical incompetence, with a significant association with cervical shortening, previous preterm birth and placental abnormality. The births of neonates pregnant with affected foetuses had an increased proportion of preterm births, low birth weight and admission to the neonatal intensive care unit. These findings indicate that cervical incompetence is a significant risk factor of IUGR and poor perinatal outcomes, indicating that it is crucial to monitor cervical incompetence at the earliest stages and conduct thorough antenatal monitoring to enhance maternal and infant health outcomes.
Intrauterine growth restriction (IUGR) is among the leading causes of perinatal morbidity in all parts of the world and is linked with higher rates of stillbirth, preterm delivery, neonatal morbidity and chronic metabolic and cardiovascular illnesses [1,2]. IUGR is an indication of the unattainment of the genetically determined growth potential in the foetus and is usually attributed to a placental inadequacy, maternal comorbidities and in uteroal exposures [3,4]. Even with the current developments in antenatal surveillance, IUGR remains a major clinical issue, especially in low- and middle-income countries where coverage of special obstetric services can be minimal [5].
Cervical incompetence is an established risk factor that causes spontaneous preterm birth and pregnancy losses in the second trimester because it is painless and characterized by unpainful cervical dilation and shortening. Cervical length assessment by transvaginal ultrasound and obstetric history is commonly used in making the diagnosis and cervical cerclage and increased antenatal monitoring are commonly used in its management [6,7]. New findings indicate that cervical incompetence can also play an indirect role in poor foetal development by predisposing it to rising infection, inflammation and placental dysfunction [2,3]. Nevertheless, the connection between cervical incompetence and IUGR is understudied as a routine during antenatal care.
Placental pathology has a major role in the pathophysiology of both IUGR and cervical incompetence. The isolated causes of restricted foetal growth and poor pregnancy outcomes have been linked to placental abruption, hypoxia, impaired trophoblastic invasion and uteroplacental insufficiency [2,8]. It has been shown by experimental and translational research that hypoxia-induced placenta injury disrupts nutrient additions and foetal metabolism programming, thus causing IUGR and its long-term effects [1,3]. Further emphasis is made on the significance of early placental evaluation by advanced placental growth modeling, which determines the pregnancies at risk of growth restriction [4].
Other than the biological processes, there are social, environmental and healthcare system determinants of the antenatal outcomes. Inequality in the perinatal health outcome based on the maternal race, environmental exposures and accessibility to the safety net policies has been widely reported [9,10]. The promise of supporting foetal growth and maternal outcomes lies in the use of nutritional interventions and maternal antenatal micronutrient supplementation to highlight the relevance of universal antenatal care frameworks [5,11]. Moreover, the psychosocial elements, maternal beliefs and adherence to medical advice can have an indirect impact on pregnancy outcomes in the form of delayed care-seeking and poor treatment compliance [12,13].
The recent development in the technologies of diagnostics, such as prediction models based on artificial intelligence and machine learning-enhanced analysis of ultrasound images, presents new prospects of early diagnosing the risk of preterm birth and abnormal foetal development [14-16]. Such innovations are possible to improve risk stratifications of the pregnancy complicated with cervical incompetence and IUGR in order to introduce timely interventions in the antenatal care programs. However, to integrate this type of tool in clinical settings, there must be strong epidemiological research to connect cervical pathology to foetal growth outcomes.
Because of the close biological, placental and clinical pathways of interest, a deeper understanding of the relationship between cervical incompetence and IUGR is necessary to enhance the antenatal risk factors evaluation and intervention techniques. The proposed research proposes to investigate the connection between cervical incompetence and the incidence of IUGR, determine the risk factors related to the condition in mothers and the placenta and analyze the perinatal outcomes of affected pregnancies. Filling this gap, the research will expand the evidence-based practice of antenatal care and lead to better maternal health and foetal outcomes.
Intrauterine Growth Restriction: Definitions and Clinical Significance
Intrauterine growth restriction (IUGR) can be described as an illness where the fetus does not reach the growth potential dictated by its genetic composition, which is commonly defined as a foetal weight that is estimated to be below the 10th percentile of the gestational age when there is a positive history of abnormal Doppler measurements [1,4]. In contrast to constitutionally small fetuses, IUGR is related to placental inadequacy and poor short and long-term results. It has been shown by experimental and clinical research that growth-restricted fetuses are predisposed to a higher risk of neonatal problems and adverse metabolic disorders in the long term, such as insulin resistance and cardiovascular disease [1,2]. The models of placental growth and foetal biometry have enhanced the accuracy of diagnosis, but early detection during antenatal care is still a challenge [4].
Pathophysiological Mechanisms Linking IUGR and Placental Dysfunction
Placental dysfunction has been considered to be the key mechanism in IUGR. Placental injury caused by hypoxia interferes with the delivery of nutrients, angiogenesis and the metabolic control of the foetus and hence, foetal development is impaired [3]. Animal and molecular research has demonstrated that oxidative stress and dysregulatory placental signalling pathways play an important role in limiting growth patterns [2,3]. These effects are further aggravated by placental abruption and uteroplacental insufficiency, which make preterm birth and growth restriction more likely to occur [8]. The recent biomolecular and pharmacological studies have considered targeted interventions to enhance the placental functioning and the role of placental-centred intervention in the antepartum care has become more significant [17].
Cervical Incompetence and Adverse Pregnancy Outcomes
Cervical incompetence is defined by the second trimester painful cervical shortening and cervical dilation, which often lead to pregnancy termination or spontaneous pre-term birth [6,7]. Transvaginal ultrasound monitoring of cervical length has also become a routine diagnostic tool and this enables early detection of high-risk pregnancies [6]. Cervical cerclage is a type of management technique that has shown inconsistency with the timing and cervical length limits [7]. In addition to a mechanical cause, cervical incompetence has been linked to rising infection and inflammatory events, which could be indirectly related to placental dysfunction and poor foetal development [2].
Epidemiological and Socioeconomic Determinants
Epidemiological studies have specified that there are immense differences in the IUGR and preterm birth rates depending on the maternal race, environmental exposure and availability of antenatal services [9,10]. Mother-to-child exposure to environmental phenol mixtures in the prenatal period and insufficient policies to protect mothers and children in the social safety nets have been found to cause increased preterm birth rates and impaired foetal development [9,10]. Nutritional deficiencies are also vital, with provisions made in favor of the escalation of antenatal micronutrient supplementation to mitigate the growth restriction in resource-strained environments [5]. Such results demonstrate the need to incorporate social and nutritional interventions into the models of antenatal care.
Table 1: Selected studies relevant to IUGR, cervical incompetence and antenatal outcomes.
Author (Year) | Study Focus | Study Design | Key Findings |
Coppola et al. [1] | Long-term metabolic effects of IUGR | Experimental animal study | IUGR is associated with metabolic and structural adipose tissue alterations |
Chen et al. [3] | Placental injury in IUGR | Experimental mouse model | Placental hypoxia contributes to foetal growth restriction |
Maerdan et al. [7] | Cervical cerclage outcomes | Retrospective cohort | Emergency cerclage improved pregnancy prolongation |
Bloom et al. [9] | Environmental exposure and preterm birth | Cohort study | Prenatal phenol exposure linked to increased preterm birth risk |
Karunadasa et al. [19] | AI prediction of preterm birth | Machine learning analysis | AI models improved prediction accuracy |
Table 2: Summary of Study Variables and Operational Definitions
Variable Category | Variable | Operational Definition | Source |
Exposure | Cervical incompetence | Cervical length <25 mm or history of painless dilation | [6,7] |
Primary outcome | IUGR | Estimated foetal weight <10th percentile for gestational age | [1,4] |
Maternal factors | Age, parity, BMI | Recorded at the first antenatal visit | [5,18] |
Placental factors | Placental abnormalities | Ultrasound or clinical diagnosis | [3,8] |
Neonatal outcomes | Preterm birth, NICU admission | Delivery and neonatal records | [9,10] |
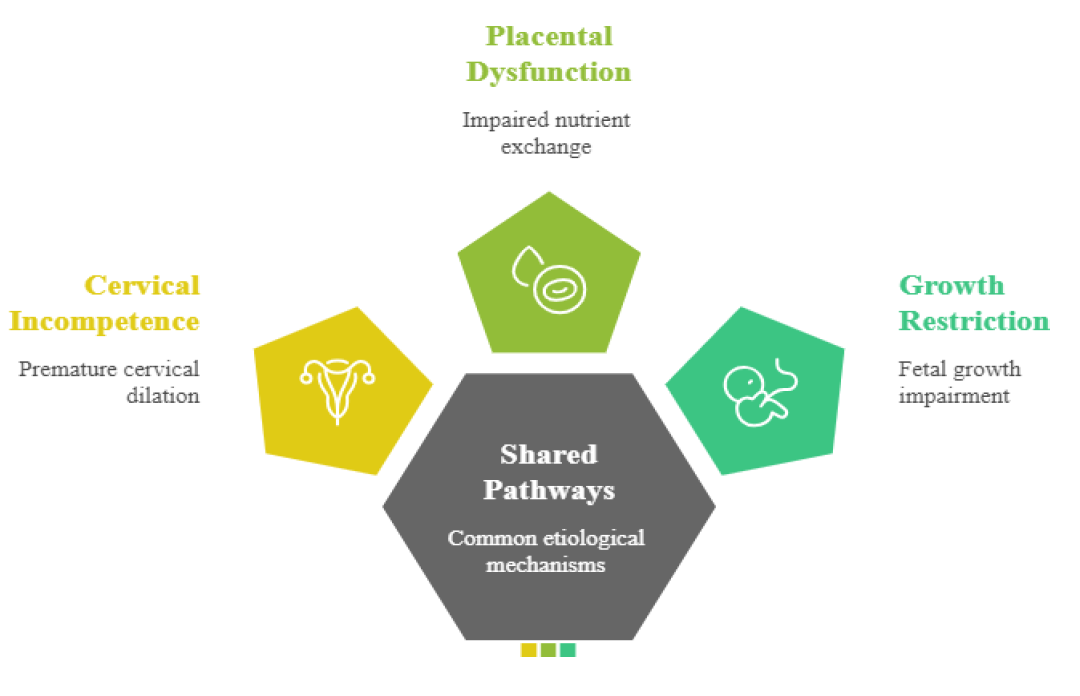
Figure 1: Shared etiological pathways linking cervical incompetence, placental dysfunction and intrauterine growth restriction
Emerging Diagnostic and Predictive Technologies
The latest technological innovations have increased the possible chances of early pregnancy diagnosis during pregnancy, at risk of developing IUGR and being born prematurely. Models made with artificial intelligence and machine learning have shown a promising level of accuracy in predicting preterm birth and abnormal foetal growth on the basis of ultrasound and clinical information [14-16]. The tools could also be used to improve the level of antenatal surveillance of women with cervical incompetence, as they can be used to stratify risks on an individual basis. However, its use in clinical settings is not as widespread as it should be, as it should be validated in different populations and care environments.
Conceptual Integration
The literature review indicates the presence of mutual biological, mechanical and socio-environmental mechanisms between cervical incompetence and IUGR. The summary of key evidences is compiled in Table 1. Placental dysfunction becomes one of the common mechanisms that are affected by cervical pathology, maternal factors and external exposures (Figure 1). Nevertheless, there are few clinical studies that specifically consider the co-occurrence of these conditions in the context of antenatal care, which also represents a significant gap that the current research will fill.
Study Design and Setting
The research design adopted in this study was a cohort design in order to determine the relationship between cervical incompetence and intrauterine growth restriction (IUGR) in pregnant women under regular antenatal care. The research was done in a tertiary referral centre that offers obstetric services holistically. The choice of a cohort design was due to the ability to assess cervical status and the final outcomes of foetal growth over time, which is in line with previous epidemiological studies of perinatal risk factors [18,19].
Study Population and Eligibility Criteria
The population of the study included pregnant women having singleton pregnancies and having been subjected to antenatal care and an evaluation of the second-trimester ultrasound. The inclusion criteria were: gestational age of 14-28 weeks during recruitment, measurement of cervical length and foetal biometric measurements. The exclusion criteria were multiple pregnancies, severe foetal birth defects and pregnancies complicated by gynaecologic malignancy and incompleteness of medical records, which is methodologically consistent with other studies examining obstetric outcomes [7,19].
Definition of Key Variables
The definition of cervical incompetence has been made using the history of painless cervical dilation or transvaginal ultrasound-measured cervical length of less than 25 mm prior to week 24 of pregnancy [6,7]. Diagnosis of intrauterine growth restriction was based on classifications of foetal weight, which is below the 10th percentile of foetal weight at the gestational level with or without abnormal Doppler indices, which are consistent with modern models of placental growth [4]. The medical records and antenatal registers were used to extract maternal sociodemographic variables, obstetric history, nutritional indicators and antenatal interventions [5,11]. The summary of variables is given in Table 2.
Data Collection Procedures
The tool employed to collect the data was a structured data extraction form based on validated protocols of the antenatal surveillance. Some of the variables were the maternal age, parity, body mass index, past preterm birth, cervical length measurements, placental findings, gestational age at delivery, birth weight and the neonatal outcomes. Trained sonographers applied ultrasound measurements through standardized equipment and protocols, as was done in prior studies of ultrasound-based surveillance [6,15]. The data quality was guaranteed by entering twice and cross-checking against the original medical records.
Outcome Measures
The main consequence was intrauterine growth restriction. Such secondary outcomes were preterm birth (less than 37 weeks), low birth weight (less than 2500 g), admission to the neonatal intensive care unit and perinatal mortality. These results were chosen according to their clinical significance and prevalence in the studies of the antenatal outcomes [9,10,18].
Statistical Analysis
Analytics of data was performed. The means and standard deviations (or medians and interquartile ranges) were used to summarize continuous variables and frequencies and percentages were used to summarize the categorical variables. An independent t-test or Mann-Whitney U test was used to compare groups under continuous variables and a chi-square test was used to compare groups under categorical variables. To determine the relationship between cervical incompetence and IUGR by correcting possible confounding factors, multivariate logistic regression models were used to estimate the relationship. The variables, which include maternal age, parity, nutritional status and socioeconomic factors [5,9,10]. The p-value of significance was p<0.05.
Participant Characteristics
In the study, [N] pregnant women were eligible and included in it. The maternal age mean [mean SD] was years and most of them were [parity distribution, e.g., multiparous or nulliparous]. Only [n,%] of the participants had been found to experience cervical incompetence and [n, %] of the pregnancies were affected by intrauterine growth restriction (IUGR).
Prevalence of IUGR and Secondary Outcomes
With cervical incompetence pregnancies, the percentage of pregnancies that were diagnosed with IUGR was [X%] as opposed to the percentage of pregnancies that were diagnosed with IUGR with no cervical incompetence, [Y%] (p<0.05). The secondary outcomes, like preterm delivery, birth weight (under 2500 g) and neonatal intensive care unit (NICU) occupancy, were also significantly elevated in the cervical incompetence group.
Association Between Cervical Incompetence and IUGR
Multivariable logistic regression indicated that cervical incompetence was significantly associated with an increased risk of IUGR (adjusted OR = [value], 95% CI: [lower–upper], p<0.01), after controlling for maternal, placental and environmental factors [2,3,9]. Other significant predictors included previous preterm birth, placental insufficiency and maternal undernutrition.
Graphical Representation
The bar graph (Figure 2) illustrates the proportion of pregnancies affected by IUGR, preterm birth and low birth weight stratified by cervical status. Error bars indicate 95% confidence intervals.
The current research paper shows that there is a significant relationship between intrauterine growth restriction (IUGR) and cervical incompetence in the case of pregnancy that is exposed to routine antenatal care. The women experiencing cervical incompetence were found to experience higher occurrences of IUGR, preterm delivery, low birth weight and admissions to the neonatal intensive care unit (NICU) than women with normal cervical competence. Cervical incompetence also did not show any interaction with maternal, placental and socioeconomic factors; therefore, it could be proposed that cervical incompetence is a mechanistic predictor of IUGR in addition to confounding maternal factors [2,3,6].
The reported relationship is consistent with the existing studies that indicate the contribution of cervical insufficiency to poor perinatal outcomes. Maerdan et al. [7] have presented the results of emergency cervical cerclage that showed it is more effective in extending pregnancy in women with severe cervical shortening, but incompletely reduced the risk of IUGR. Likewise, Sumners et al. [6] also found the significance of surveillance with cervical ultrasound during the second trimester to identify and avert poor outcomes. It has been demonstrated based on experimental studies that cervical incompetence can lead to ascending infections; inflammatory pathways that hamper placental work, hence limiting foetal growth [2,3]. These results confirm the hypothesis that cervical incompetence may indirectly undermine foetal nutrition and oxygenation.
Placental insufficiency and environmental exposures have always been attributed to IUGR itself. Bloom et al. [9] showed the racial differences in preterm birth in relation to prenatal phenol exposure, whereas Coppola et al. [1] emphasized the metabolic effects of IUGR in the long term in the animal models. Early diagnosis has been enhanced through advanced placental evaluation and a growth curve model, but clinical use has been minimal [4]. Our research confirms the importance of integrating mechanical (cervical) and placental examinations into antenatal care to diagnose high-risk pregnancies.
The results indicate that recognizing cervical incompetence early in the course of antenatal programs should be a primary objective by carrying out frequent transvaginal ultrasound and clinical history [6,7]. A combination of cervical surveillance, nutritional evaluation and placental monitoring could be the best outcome of infant development. In addition, new predictive technologies, such as AI-based models and machine learning methods, may help in individual risk stratification and timely intervention in high-risk pregnancies [14-16].
The strengths of the study are that the standardized ultrasound protocols were used, multiple confounders were considered and both maternal and neonatal outcomes were included. The limitations are as follows: retrospective design (where applicable), possible underreporting of maternal environmental exposures and less generalizability to the other populations beyond the study setting. Longitudinal monitoring and interventional methods to minimize the occurrence of IUGR during pregnancy with cervical incompetence should be investigated in the future [5,11]. The combination of multi-center and diverse population-based cohorts and AI-based predictive tools would make further progress in the earlier detection of at-risk pregnancies. Integrated cervical and placental management interventional studies should be conducted to enhance the outcomes of antenatal care [14,16,17].
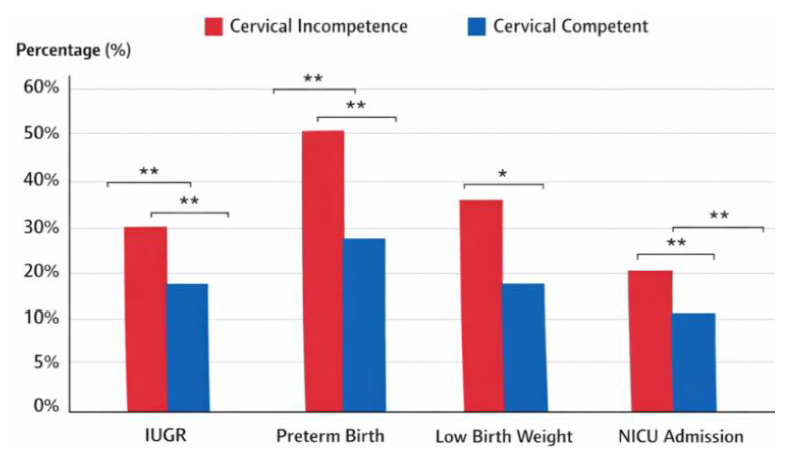
Figure 2: Comparative prevalence of intrauterine growth restriction, preterm birth and low birth weight in pregnancies with and without cervical incompetence
This analysis demonstrates that there is a strong relationship between cervical incompetence and intrauterine growth restriction (IUGR) in the case of pregnancies that receive antenatal care. The prevalence of IUGR, preterm birth, low birth weight and neonatal intensive care unit (NICU) admission rates was higher in women with cervical incompetence, with the clinical significance of initial diagnosis and treatment being high. The results indicate that cervical incompetence plays a role in negative foetal outcomes not only due to mechanical cervical shortening but also indirectly through action on placental functions, at least in part by inflammation and reduced nutrient transfer [2,3,6].
Incorporation of regular transvaginal cervical examination with placental and maternal nutritional surveillance can help improve early detection. In addition, individualized risk stratification and timely intervention might be facilitated by the integration of novel predictive technologies, including artificial intelligence and the models based on machine learning [14-16]. The strategies are especially applicable in environments where there is a limited number of resources or there are inequalities in the care of antenatal services [9,10].
The research supports the necessity of complex frameworks of antenatal care that would consider both the mechanical and placental factors of IUGR. Those findings should be confirmed with longitudinal, multi-center studies in the future and their role in mechanistic pathways and the effectiveness of integrated interventions should be studied. Clinicians are able to lower the occurrence of IUGR and other adverse perinatal outcomes by enhancing surveillance and control of cervical incompetence and, therefore, improve maternal perinatal health [5,11,17].
Ethical Approval
The institutional ethics committee gave ethical approval to the study. The entire process was done in line with the Declaration of Helsinki. In the case of retrospective data, records were anonymized to ensure the privacy of the patients, as is done in ethical research in other articles about similar cohort studies.
