+91 6002993949
submission@iarconsortium.org
Open Access
ISSN (Print) : 2709-3271
ISSN (Online) : 2709-3263
One of the most prevalent public health issues, diabetes affects 387 million people worldwide, with type 2 diabetes accounting for over 90% of cases (DM type 2) [1]. Diabetes, which is currently the fourth most common cause of death and illness globally, is on the rise. It is imperative to attain optimal glycemic control at an early stage in order to avert complications and death [2]. Despite the fact that only 53.6% of type 2 diabetics reach the desired goal of a glycated hemoglobin (HbA1c) of less than 7% [3]. Personalized targets are recommended by the American Diabetes Association (ADA) and the European Association for the Study of Diabetes (EASD) based on a number of factors, including co-morbidities, patient preferences, needs, values, duration of diabetes, risk of hypoglycemia, costs, and the assurance of a patient-centered approach [4]. Targets of less than 6.5% for newly diagnosed patients and less than 7.5% for people receiving two or more medications are advised by the National Institute for Health and Clinical Excellence (NICE) in the United Kingdom [5]. One of the main causes of not reaching these goals is the co-occurrence of psychological problems.
Roughly 10–20% of elderly people experienced symptoms of depression [6]. The risk is higher—between 25 and 33 percent—for people with chronic diseases [7]. According to Yaseen and Dauod (2019) [8], these illnesses have a detrimental impact on quality of life and have significant economical ramifications [9]. According to several studies (Lustman et al., 2000; Gross et al., 2005) [10-11], diabetes patients have a higher prevalence of depression, which contributes to their poor glycemic control and complications. According to other research, depression is linked to both cognitive decline and physical disability, both of which are more common in people with diabetes [12-13]. And additionally imply that depression frequently has a prolonged course [14-15]. Depression and anxiety symptoms may arise as a result of the neuroendocrine abnormalities linked to diabetes mellitus (DM), such as elevated cortisol levels and changed dopamine concentrations [16-17]. The purpose of this research is to identify diabetes patients' levels of anxiety and despair. To ascertain the association between diabetes patients' anxiety and depression and demographic information like age, gender, etc.
The International Diabetes Federation estimates that one in eleven persons worldwide suffers from diabetes, and that one in fifteen adults worldwide has impaired glucose tolerance. These statistics support the organization's claim that diabetes is "one of the largest global health emergencies of the 21st century." It is projected that these numbers will rise sharply, especially among urban residents, leading to an increase in medical and financial problems [18]. It is anticipated that this increase will bring the total amount spent on diabetes treatment to 12%. In Iraq, the total number of people affected by diabetes was 561000 in 1995 and 678000 in 2000; by 2025, that figure is predicted to rise to 1,739,000 [19]. According to Bromet et al. (2011) [20], the lifetime prevalence of depression, a highly serious illness, ranges from 11% in low-income nations to 15% in high-income ones. According to Hewlett et al. (2014) [21], there is a 50% lifetime risk of mental health issues, along with a significant decline in productivity and employment. In high-income countries, diabetes is thought to be the eighth cause of disability-adjusted life years, while depression and anxiety rank fourth [22]. The Diagnostic and Statistical Manual of Mental Disorders (DSM-5) published by the American Psychiatric Association defines depression as a mood disorder that reunites multiple symptoms that impair an individual's functionality. Emotions, thoughts, and actions are disrupted by depression [23]. Depression is classified as a first episode, a recurrent or chronic episode, mild, moderate, or severe, with or without psychotic symptoms, according to the DSM-5. Research has demonstrated that there is a higher chance of depression in individuals with pre-diabetes and diabetes who are not yet diagnosed. Diabetes is more common in patients with a history of the illness than in healthy individuals. and could be two times higher in type 2 diabetics than in the general population [24].
Anxiety and depression can exacerbate the prognosis of diabetes, increase medication non-adherence 9, and lower health-related quality of life. Additionally, there is a risk of According to Rubin et al. (2008) [25], the risk of type 2 diabetes mellitus increases to 60%. There seems to be a reciprocal, intricate interaction between depression and diabetes. biological mechanisms, the understanding of which improves harmful consequences. Recent assessments of the literature have indicated three possible routes for the relationships. Diabetes may increase the likelihood of depression in the future, and depression may have a common etiology with diabetes. This cross-sectional study sought to highlight the need of screening for depression in individuals with diabetes and to demonstrate the connections between depression and diabetes [26].
Study design: Interview Study design conducted at the period of 1st of August 2023 to 20st November 2023 to determine anxiety and depression among patients with diabetes in from the primary health care centers in Al-Nasr sector, Dhi Qar city, Iraq
Sitting: The study carried out at 4 the primary health care centers in Al-Nasr sector, Dhi Qar city, Iraq
Sample: The study sample consisted of 200 male and female who were patients coming to the early detection unit and who were suffering from diabetes in 4 primary healthcare centers in Nasr sector. They were selected using a probability method (simple random sample) from 4 primary health care centers in Nasr sector.
Instrument: The study instrument is a questionnaire composed of 2 parts:
Part one: Part one: demographic data; This part consists of 6 items : Age , Gender, Level of education, Marital status, Disease duration, Sugar check.
Part two: Anxiety And Depression Scale; This part consists of 2 domain items. Each domain contains seven questions .
Data Collection: Data is collected by the researcher, and the researcher explains the study and the purpose of the sample and obtains the consent of the sample to participate in the study and then uses the Interview Study method to collect data from the sample. Data will be collected by the researcher through a face-to-face interview with the help of the nursing staff.
Ethical consideration: The researcher explains the study and the objectives to the sample and asks them to participate in the study. After taking the sample agreement, the investigator collects the data through the use of the interview method.
Validity of the Questionnaire
Validity is concerned with the extent to which an instrument corresponds. The content validity of the instrument was established through a panel of (4) experts from different specialties. The results of the review of the questionnaire by the experts revealed that all of the experts agree that items of the study instrument are clear and adequate for the measurement of the phenomenon.
Data Analysis: The descriptive purposes of the study were determined through the frequency distribution. The association of two proportions was evaluated by Chi-square tests. The predictors of depression in diabetes patients were determined through the univariate analyses. The significant level was considered as a P-value of less than 0.05. All calculations were performed by Statistical Package for Social Sciences (SPSS, version 22).
Table 1: distribution of the sociodemographic characteristic of sample
Variables | Frequency | Percent | |
Age | 20-29 | 5 | 2.5 |
30-39 | 15 | 7.5 | |
40-49 | 80 | 40.0 | |
50-59 | 91 | 45.5 | |
60-69 | 9 | 4.5 | |
Total | 200 | 100.0 | |
Mean and standard deviation 49.8±7.775 | |||
Gender | Female | 104 | 52.0 |
Male | 96 | 48.0 | |
Total | 200 | 100.0 | |
Education | Secondary school | 71 | 35.5 |
Institute | 62 | 31.0 | |
BSN | 54 | 27.0 | |
Higher education | 13 | 6.5 | |
Total | 200 | 100.0 | |
Marital status | Single | 1 | .5 |
Married | 181 | 90.5 | |
Single | 8 | 4.0 | |
Widow | 10 | 5.0 | |
Total | 200 | 100.0 | |
Diseases diagnosis period | Mean and standard deviation 7.495±3.086 | ||
This finding in table 1 shows that 45.5% of sample at age (50-59) years, 52% of them were females, 35.5% of them had secondary school graduated, 90.5% of them married and the mean of DM diagnosis period was 7.495.
Table 2: distribution of distribution of Anxiety and Depression among patients with DM
Variables | Frequency | Percent | |
Anxiety | Normal (0-7) | 0 | 0 |
Borderline (8-10) | 40 | 20.0 | |
Severe (11 and more) | 160 | 80.0 | |
Total | 200 | 100.0 | |
Depression | Normal (0-7) | 5 | 2.5 |
Borderline (8-10) | 47 | 23.5 | |
Severe (11 and more) | 148 | 74.0 | |
Total | 200 | 100.0 | |
This finding in table 2 and figure 1 shows that 80% and 74% of patients with DM had severe anxiety and depression respectively.
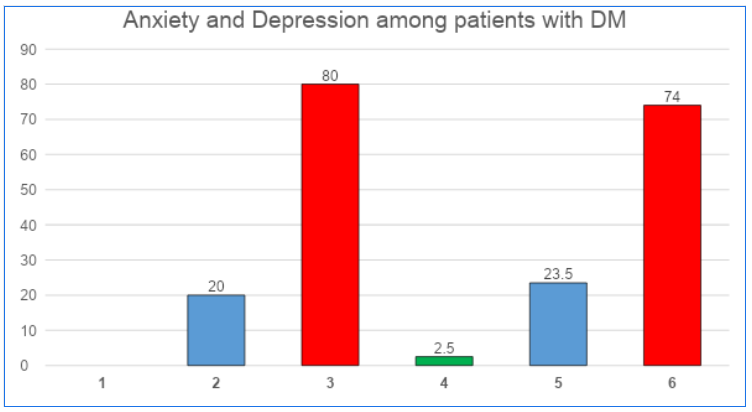
Figure 1 distribution of Anxiety and Depression among patients with DM
Table 3: relationship between Anxiety among patients with DM and sociodemographic characteristic
Variables | Anxiety | Total | Chi square | ||
Borderline | Severe | ||||
Age | 20-29 | 3 | 2 | 5 | Chi=9.452 P=0.051 Sig.=NS |
30-39 | 4 | 11 | 15 | ||
40-49 | 10 | 70 | 80 | ||
50-59 | 20 | 71 | 91 | ||
60-69 | 3 | 6 | 9 | ||
Total | 40 | 160 | 200 | ||
Gender | Female | 24 | 80 | 104 | Chi=1.282 P=0.258 Sig.=NS |
Male | 16 | 80 | 96 | ||
Total | 40 | 160 | 200 | ||
Education | Secondary school | 11 | 60 | 71 | Chi=3.218 P=0.359 Sig.=NS |
Institute | 11 | 51 | 62 | ||
BSN | 15 | 39 | 54 | ||
Higher education | 3 | 10 | 13 | ||
Total | 40 | 160 | 200 | ||
Marital status | Single | 0 | 1 | 1 | Chi=5.425 P=0.143 Sig.=NS |
Married | 35 | 146 | 181 | ||
Single | 4 | 4 | 8 | ||
widow | 1 | 9 | 10 | ||
Total | 40 | 160 | 200 | ||
P= p value, Sig= significant, HS= high significant, S=significant, NS= non- significant
In table 3, there is no significant statistical relationship between Anxiety among patients with DM and sociodemographic characteristic
Table 4: relationship between Depression among patients with DM and sociodemographic characteristic
Variables | Depression | Total | Chi square | |||
Normal | Borderline | Severe | ||||
Age | 20-29 | 0 | 0 | 5 | 5 | Chi=8.755 P=0.363 Sig.=NS |
30-39 | 0 | 6 | 9 | 15 | ||
40-49 | 1 | 18 | 61 | 80 | ||
50-59 | 4 | 19 | 68 | 91 | ||
60-69 | 0 | 4 | 5 | 9 | ||
Total | 5 | 47 | 148 | 200 | ||
Sex | Female | 1 | 21 | 82 | 104 | Chi=3.748 P=0.154 Sig.=NS |
Male | 4 | 26 | 66 | 96 | ||
Total | 5 | 47 | 148 | 200 | ||
Education | Secondary school | 2 | 18 | 51 | 71 | Chi=2.804 P=0.833 Sig.=NS |
Institute | 1 | 16 | 45 | 62 | ||
BSN | 2 | 9 | 43 | 54 | ||
Higher education | 0 | 4 | 9 | 13 | ||
Total | 5 | 47 | 148 | 200 | ||
Marital status | Single | 0 | 0 | 1 | 1 | Chi=1.927 P=0.926 Sig.=NS |
Married | 5 | 41 | 135 | 181 | ||
Single | 0 | 3 | 5 | 8 | ||
widow | 0 | 3 | 7 | 10 | ||
Total | 5 | 47 | 148 | 200 | ||
In table 4, there is no significant statistical relationship between Depression among patients with DM and sociodemographic characteristics.
The purpose of the study being conducted by the author was to confirm the level of depression and anxiety in a sample of Iraqi patients with Type 2 diabetes who were receiving care in Al-Nasr medical centers. According to the study, 80% of the patients experience anxiety, and 74% experience depression. Population prevalence of anxiety and depression based on the degree of diabetes mellitus and diabetes severity. Everywhere in the world is a different place. While an Iraqi study indicated that 37.2% of depression cases were reported in Babylon, Khamisa (2019) [27] found that a similar depression rate of 71.8% was identified in an adult Iranian sample [28]. a reduction in the depression score. As stated in affluent nations, for instance, in the US, between 2% to 28.8% [29], and in Greece, 33.4% [30].
According to the study, aging is a significant predictor of major anxiety and depression in people with type 2 diabetes. The outcome as it stands is debatable. That is all. While some researchers [28] have endorsed this, others [31] have not negative consequences for health. Older patients often report related quality of life [32]. As senior people endure a higher lack of support and use poorer healthcare services. Previous research has shown that being a woman is a strong predictor of depression severity. 26 Research indicates that women are twice as likely as men to have depression [33], and that estrogen levels may have an impact [34]. Women may also be more emotional and open because of the societal roles that are assigned to them, such as emotional expressiveness, submissiveness, and passivity.
Contrary to findings from earlier investigations, the current study indicated that the duration of DM was not substantially linked with depression. However, it should be noted that the length of the diabetes condition increases the complications associated with it [35], and as a result, depression risk increases [36].
Shows no significant association between anxiety and the following socio-demographic factors: age (0.051), gender (p = 0.258), Education (p = 0.359), marital status (p = 0.143).
shows no significant association between depression and the following socio-demographic factors: age (0.363), gender (p = 0.154), Education (p = 0.833), marital status (p = 0.926).
The depression and anxiety percentages among diabetes are divisive among studies globally. Some studies showed approximately similar results 56.1% [37] and 60.0% [38] for depression and 55.1% [39] and 57.9% [40] for anxiety respectively. Other studies in India, Malaysia, and Saudi Arabia reported a lower result 26.3% [41], 26.6% and 22.45% [42] for depression and 27.6% [43] and 28.5% [42], for anxiety respectively.
There are a number of plausible causes for the high rate of mental illnesses among diabetes in this study, including inadequate understanding and societal barriers that discourage general practitioners from treating these diseases' symptoms. The study was carried out during a period of unstable politics, a corrupt economy, and a lack of a health insurance system, which led to several societal complexities. Together, these elements led to comparatively elevated symptoms of anxiety and depression.
The study revealed that a large percentage of diabetic patients suffered from anxiety and or depressive symptoms. The results should alert all physicians working in primary health centers to consider these symptoms since they have a direct impact in improving treatment.
Better strategies for the early identification and treatment of depression in patients with diabetes mellitus, as well as increased healthcare provider awareness, are imperative given that diabetes remains a major health concern in Iraq. Training programs on depression screening should be offered to medical professionals who care for patients with diabetes mellitus, and it would be beneficial to conduct additional research in Iraq to assess the possible link between type 2 DM and depression.
