
+91 6002993949
submission@iarconsortium.org
Open Access
ISSN (Print) : 2709-3239
ISSN (Online) : 2709-3220
Background: One of the most frequent causes of a Massive hemothorax, which refers to a buildup of blood in the pleural area, is either blunt or penetrating injury to the chest wall. In the USA, the majority (70-80%) of cases of hemothorax occur as a result of accidents involving motor vehicles that inflict harm on structures in the mediastinum such as the heart, vessels of major importance, thoracic spine, mammary or intercostal arteries, the diaphragm, or the lung tissue. Case Description: A 16-year-old teenager arrived to the Emergency Room (ER) with stab wound on the left side of the chest caused by a scissor. The patient presented with chest pain, breathlessness and hypoxia. A general surgeon performed emergency management by inserting a chest tube due to the significant left hemothorax. The patient's respiratory problem necessitated the immediate insertion of a chest tube in order to assess future treatment needs. Because the patient was hemodynamically unstable, resuscitation was performed immediately and we then performed a chest X-ray. We did not perform a CT scan of the thorax because the patient's hemodynamics were unstable. The thoracic and vascular surgeon performed an emergency posterolateral thoracotomy to address and stopped the bleeding from the intercostal artery. The patient had been discharged from the hospital seven days after surgery with no complications and stable hemodynamics. A week later, the patient visited the outpatient department for follow-up. Conclusion: The initial step for an emergency physician in treating a hemothorax is to diagnose the condition with imaging techniques like a chest x-ray, ultrasound, or CT scan of the thorax. When dealing with hemothoraces, a chest tube should be inserted to prevent the development of empyemas and fibrothorax. Massive hemothoraces require a thoracotomy, consultation with a trauma surgeon and volume resuscitation. The key to reducing morbidity and mortality from hemothoraces is prompt diagnosis and treatment. Additional testing is required to determine if the aesthetic and motor functions of the left hand joint space are impaired.
Hemothorax, or blood collection in the pleural space, most frequently results from injuries to the chest wall, either penetrating or blunt [1-3].
Mediastinal structures (the heart, major vessels, thoracic spine, intercostal or mammary arteries and the diaphragm or lung parenchyma) are commonly injured in motor vehicle incidents, accounting for 70-80% of hemothoraces in the United States [4-7].
Evaluation of intrathoracic injuries with CT scan is the gold standard, but this may not be possible in the unstable trauma patient. CT scans are not always easily accessible, especially in smaller facilities. Historically, chest radiography has been used as a quick diagnostic tool for potentially fatal injuries. Point-of-care ultrasound (POCUS) has shown promise as a complementary imaging modality, according to recent research. POCUS is convenient because it can be used anywhere at any time. At the bedside, it can be used to determine which injuries are the most serious and begin treatment immediately. Since the middle of the 2000s, the pulmonary window has been a part of the Extended Focused Assessment with Sonography in Trauma (eFAST) protocol. The operator can quickly assess for fluid above the diaphragm by sliding the probe cephalad in addition to the conventional right and left upper quadrant views of the Focused Assessment with Sonography (FAST). Chest ultrasonography has been shown to be an effective diagnostic tool for patients with blunt chest trauma in a number of studies [8-13].
Evaluation for hemothorax using lung ultrasound (US) has achieved accuracy, with higher sensitivity than chest radiography [14,15].
4 hours before admission, patient was playing with his brother when suddenly his brother accidentally threw scissor towards him. The scissor penetrated his left side of the chest for a while before it fell out on its own. After the incident, patient felt pain on his left chest, Breathless, no active bleeding. By his family, patient was brought to a local clinic and the wound was cleaned and dressed with sterile gauze. Because patient gradually feel Breathless and the symptom worsen, the family brought him to Moewardi Hospital.
The 16-year-old teenager male patient presented with unstable hemodynamics. Evidence of anemia and cyanosis in the mucous membranes was observed. The patient presented with a blood pressure of 85/50 mmHg, a pulse rate of 117 beats per minute and a respiratory rate of 30 breaths per minute. The patient's arterial oxygen saturation level while breathing ambient air was 92%. Chest examination showed breathing from the right chest was higher than the right one. The open wound size 1.5 x1 cm on 7th rib lateral left of the linea mid clavicle, on percussion lung sounds dim at the level 7th rib (Figure 1).
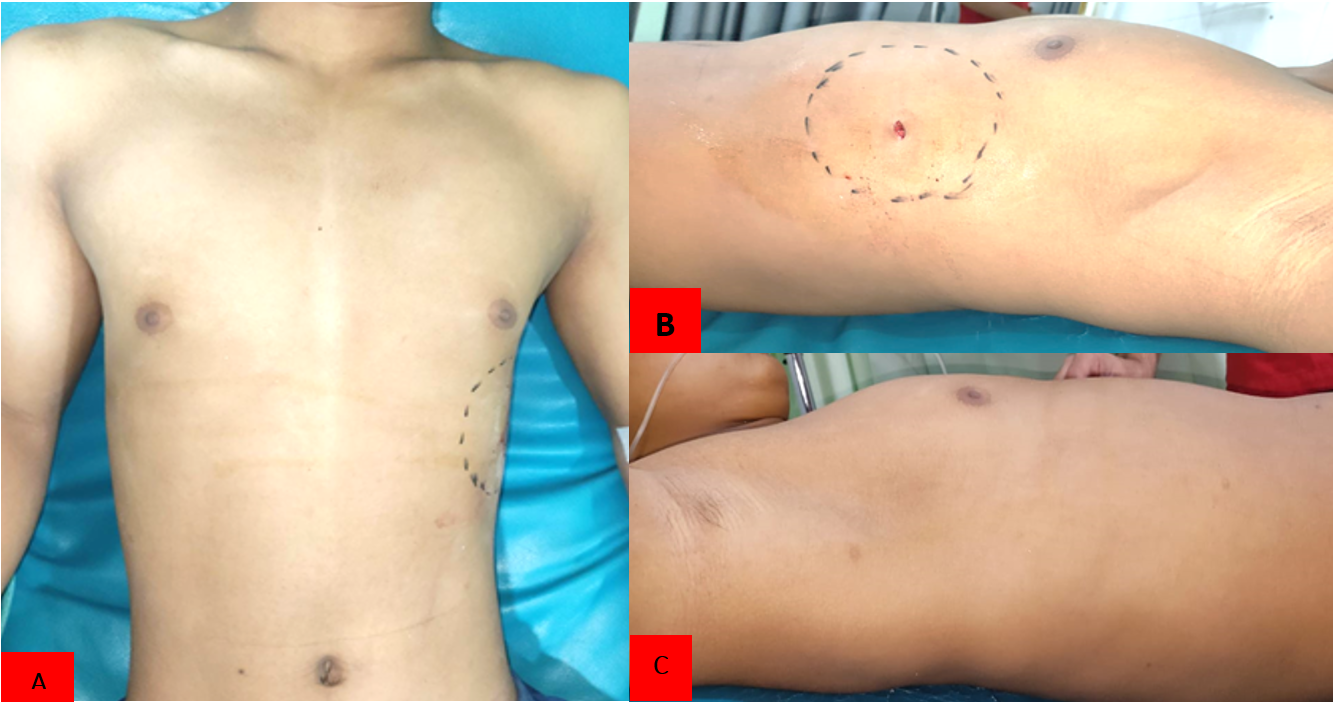
Figure 1. Picture of Patient Before Operating Surgery A: Front View, B: Right Side View and C: Left Lateral Side Views
The patient was administered a 250 UI injection of human tetanus immunoglobulin, 1g injection of ampicillin every 8 hours and 10 liters per minute of oxygen through a non-rebreathing mask during resuscitation.
Clearing the breathing through left side of the chest tube thoracostomy resulted in the loss of 300 ml of blood during the procedure. Blood was being produced at a rate of 250 ml per hour prior to entering the operating room. A transurethral catheter was inserted to collect and analyze urine samples. Testing included a complete blood count, blood glucose and a chest X-ray. Hemoglobin levels were low (9.1 g/dL), white blood cell counts were high (18.7 x 103 cells/L) and segmental neutrophil percentage was high (89.2%). The blood gas analysis found (pH \: 7.2, BE: -1.7 mmol/L), (PO2: 76.6 mmHg) and lactate serum increased to 1.9 mmol/L. Chest X-ray examination showed that a massive hemothorax (Figure 2).
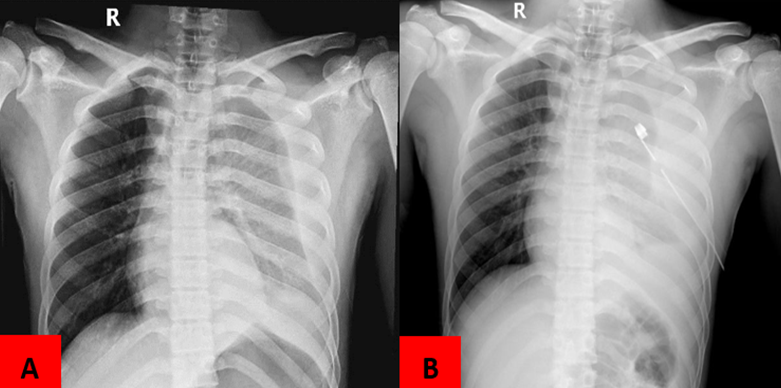
Figure 2. Picture A: Chest X-Ray patient before chest tube thoracostomy, Picture, B: Chest X-Ray patient before chest tube thoracostomy
The patient's respiratory problem necessitated the immediate insertion of a chest tube thoracostomy in order to assess future treatment needs. Because the patient was hemodynamically unstable, resuscitation was performed immediately, the thoracic and vascular surgeon performed an emergency thoracotomy to address and stopped the bleeding from the intercostal artery.
Thoracotomies were delicately performed on the most pressing problem areas. Intercostal artery bleeding required immediate thoracotomy. General anesthesia was administered and the patient was positioned in the lateral decubitus posture on the right lateral side. A 16-centimeter incision was made in the posterolateral area of the left 7th ICS and extended all the way to the intercostal muscle after the area had been properly sterilized. An incision was made just above the left eighth rib and before the midaxillary line.
The surgeon separated the serratus anterior muscle by cutting the fascia in the back. The shoulder blades and scapulae were mentioned. The seventh ICS was found by palpating the full extent of the second set of ribs under the scapula.
Following a successful procedure, the left lung has been deflated. An incision was made between the seventh and eighth left of the ribs in order to reach the parietal pleura. A blood clot was discovered in the pleural space. The ruptured left 8th intercostal artery was ligated using a simple interrupted 4.0 nonabsorbable monofilament thread to secure it and the bleeding was stopped. A single-bottle water seal drainage system was attached to a thoracotomy chest tube (number 28F) placed in the pleural space. By sucking blood from the right pleural cavity, WSD (Water seal drainage) generated 500 ml of blood. A chest tube was successfully fastened using live knots.
A 2.0 multifilament absorbable thread was used in a simple interrupted technique to suture the subcutaneous tissue. Subcuticular suture 3.0 multifilament absorbable was used to close the cutis at the end of the procedure. Active bleeding during surgery necessitated the use of four bags of packed red cells and four bags of whole blood. It was estimated that 950 ml of blood was lost during the operation. The routine hematology performed after surgery showed a decrease in abnormal leukocytes (7.3 x 103 cells/L).
Chest x-rays showed a lung contusion, so a thoracostomy tube was placed. The patient required intensive care and was transferred there. It is standard practice to measure daily : blood pressure, pulse, temperature, urine output and the contents of both chest tubes. There was 80 ml of serohemorrhage from the chest drainage, respectively, on day one. The patient was hospitalized for one day and then released with normal leukocyte counts. After three postoperative days, the chest drainage was stopped, the chest tube was removed and an X-ray of the chest revealed only a pulmonary contusion. The patient is being moved to a regular care facility. After five days in the hospital, the patient was released. The patient's general condition was good, the wound was clean and there were no signs of inflammation during the 14-day post-op follow-up (Figure 3).

Figure 3: Picture of Durante of Operation, Blood Cloth Had Already Evacuate
Thoracic penetrating trauma can cause serious complicated in addition to potentially life-threatening consequences [13].
Trauma to the chest or abdomen can cause serious problems with breathing and circulation if not treated right away. Patients with severe chest injuries, such as a massive hemothorax or a puncture wound, should undergo resuscitative thoracotomy [8].
Patients with hemothoraces can present with a variety of symptoms, including difficulty breathing (25% of hemothoraces are associated with concomitant pneumothoraces) and hemodynamic instability due to hemorrhagic shock [4].
A hemothorax is most easily detected on a chest x-ray in a patient who is hemodynamically stable [4,5].
When taking a chest X-ray, it's best to stand up so that any flattening of the costophrenic angle (caused by 150-300 mL of blood in the pleural space) can be seen [1,2,3].
Chest X-rays taken in the supine position, or even in an inadequate upright position, can be deceiving because blood pools behind the diaphragm. According to reports, the sensitivity of a supine Chest X-ray for detecting a hemothorax is only 40-60% [5].
Despite studies collecting >1,000 mL of blood from the thoracic cavity, only a hazy opacification of the hemithorax was seen on supine Chest X-rays [5,6].
Preliminary medical imaging studies, including a thoracic radiograph and focused abdominal ultrasonography for traumatic injury (FAST), may indicate the presence of hemorrhage in the peritoneal and abdominal cavity, as well as in the pericardium [12].
Tube thoracostomy describes the procedure of inserting a tube into the pleural cavity for the purpose of removing air, blood, bile, pus, or other fluids. Blood clot evacuation from the mediastinum and hemorrhage control may require a thoracoscopic or open thoracotomy procedure. If there is significant bleeding (>1,500 mL) or ongoing hemorrhage (>200 mL/hour), a thoracotomy may be necessary [9].
The thoracic manifestation of a hematoma varies. First, a chest x-ray or CT scan will be used to confirm a diagnosis of hemothorax. Despite the results of a chest x-ray (or CT if the patient's hemodynamics are stable), a hemothorax should be ruled out if the underlying mechanism suggests it. The thoracic tube insertion procedure is used to treat a hemothorax. Transfuse, consult and thoracotomy are the treatments we would use if we discovered a massive hemothorax. If the patient's blood pressure remains low even after pulmonary bleeding has been stopped, other causes should be investigated. More study is required into the effects of auto-transfusion of raw shed hemothorax blood. Hemostasis may be achieved by clamping the lung hilum (pulmonary vasculature) after the parietal pleura has been opened [2].
Persistent hypotension despite treatment for bleeding in the lung parenchyma or hilum is an indication of further injury and should be taken seriously. Perform a thorough patient assessment. If the patient's hemodynamic status does not improve, aortic clamping may be necessary (a trans-esophageal echocardiogram can be performed in the operating room to evaluate aortic injury) [2,3].
The primary focus should still be on resuscitating lost volume. Blood transfusions should be started if deemed necessary. Penetrating chest trauma should prompt immediate medical attention. Most hemothoraces result from damaged lung parenchyma and resolve on their own, making chest tube thoracostomy an effective method of treatment [2].
Placing a chest tube is therapeutic because it helps stop bleeding by allowing the lung to expand and pressing against the visceral and parietal pleura [1]. The common complications of empyema and fibrothorax can be avoided if blood is drained from the parietal cavity [1,2].
Hypoxia, persistent hypotension, a penetrating injury, and/or multiple palpable rib fractures, a flail segment, significant chest wall ecchymosis, or tenderness to palpation on physical examination are all reasons to suspect a hemothorax. Multiple studies have shown that ultrasound is just as sensitive as chest radiographs in detecting hemothoraces. When it comes to diagnosing and assessing hemothoraces, CT continues to be the gold standard. A hemothorax was found in 25% of patients in a 2007 retrospective study by Traub et al. who examined 141 patients with blunt chest trauma who presented to a Level 1 trauma center [10].
In this particular case, we determined that the patient's difficulty breathing was due to a massive hematothorax on the patient's left side, with evidence of ongoing bleeding visible on the x-ray findings. X-ray results from a futile FAST examination showed no evidence of damage to the abdominal wall that had penetrated the lung diaphragm. The examination proceeded with thoracoscopy per the recommendations of the 2014 World Journal of Surgery [11] (Figure 4).
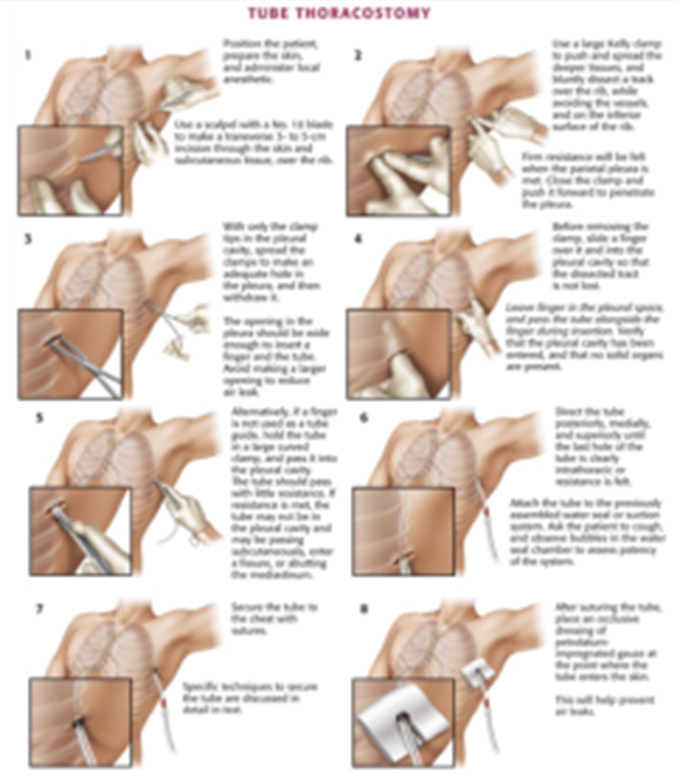
Figure 4: Performing a Tube Thoracostomi [4]
A large-bore tube (32F to 40F) is inserted into the 4th or 5th intercostal space along the anterior axillary line and then sealed and suctioned (20-30 mL H2O) to perform a tube thoracostomy [2].
Serial Chest X-rays should be taken to check on the progress of the lung parenchyma's re-expansion and the hemothorax's resolution [2].
Delaying a thoracotomy in cases of chest injury can lead to complications like empyema and fibrothorax. Recent prospective research involving 293 patients at a level I trauma center compared chest tubes ranging in size from 28F to 32F and 36F to 40F. There was no discernible difference in outcomes between patients with and without a history of chest tube placement. Drainage output below 150 mL/24 hours is being considered for chest tube extubation [10].
The most serious problem is dealing with a massive hemothorax, which is defined as a loss of blood of more than 1,500 mL (or 3 mL/kg/h) within the first two to four hours after a chest tube thoracostomy [5,6].
In addition to the conditions below, these should be taken into account when deciding whether or not to perform an emergency thoracotomy:
Progressive hemothorax observed on subsequent chest radiographs [2]
Hypotension persists despite sufficient blood replacement, after ruling out other potential sources of blood loss [2]
Patient experienced decompensation following initial response to volume resuscitation [2]
An urgent or emergent thoracotomy should be performed as a follow-up procedure
When hemothorax occurs unexpectedly, a thoracotomy must be performed immediately. Several variables, including indications, clinical presentations, trauma mechanism and imaging results, need to be considered when handling a medical emergency [11] (Figure 5).
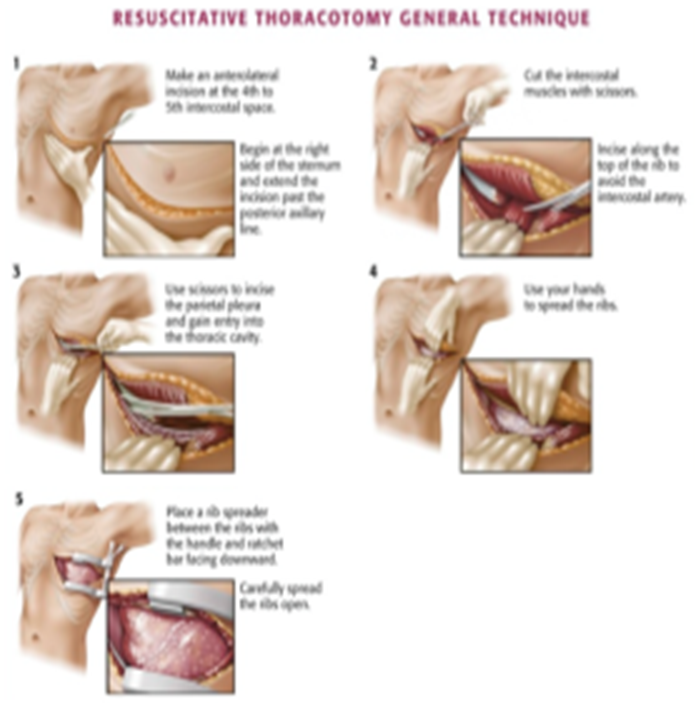
Figure 5. Performing a Thoracotomi [7]
The initial step for an emergency physician in treating a hemothorax is to diagnose it with imaging techniques like a chest X-ray, ultrasound, or computed tomography. When dealing with hemothoraces, a chest tube should be inserted to prevent the development of empyemas and fibrothorax. Massive hemothoraces require a thoracotomy, consultation with a trauma surgeon and volume resuscitation. The key to reducing morbidity and mortality from hemothoraces is prompt diagnosis and treatment [1,2,3].
The management of thorax trauma requires the participation of the medical team's multidisciplinary specialists in order to be successful. Damage to organs, as well as a high morbidity and mortality rate, are all associated with a stab wound to the thorax region.
Urgent and necessary interventions such as chest tube thoracostomy and thoracotomy procedures are imperative in managing critical medical conditions to ensure patient survival and minimize potential long-term complications. The optimal treatment modalities are determined based on the patient's clinical presentation, injury severity and concomitant injuries.
Bernardin, B. and J. Troquet. “Initial management and resuscitation of severe chest trauma.” Emergency Medicine Clinics of North America, vol. 30, 2012, pp. 377–400.
Eckstein, M. and S. Henderson. “Thoracic trauma.” Rosen’s Emergency Medicine, ch. 45, pp. 431–458.e3.
Meyer, D. “Hemothorax related to trauma.” Thoracic Surgery Clinics, vol. 47, 2007.
Kirsch, T. and J. Sax. “Tube thoracostomy.” Roberts and Hedges’ Clinical Procedures in Emergency Medicine, ch. 10, Elsevier Saunders, 2011, pp. 189–211.
Kortbeek, J. et al. “Advanced trauma life support, 8th edition: The evidence for change.” Journal of Trauma, vol. 64, no. 6, 2008, pp. 1638–1650.
Legome, E. and L. Shockley. Trauma: A Comprehensive Emergency Medicine Approach. Cambridge University Press, 2011.
Jones, R. and E. Rivers. “Resuscitative thoracotomy.” Roberts and Hedges’ Clinical Procedures in Emergency Medicine, ch. 18, Elsevier Saunders, 2011, pp. 325–339.
Sawhney, C. et al. “Management of a massive thoracoabdominal impalement: A case report.” Scandinavian Journal of Trauma, Resuscitation and Emergency Medicine, vol. 17, no. 1, 2009, pp. 1–4.
Chen, C.Y. et al. “Hemothorax in a medical intensive care unit: incidence, comorbidity and prognostic factors.” Journal of the Formosan Medical Association, vol. 109, no. 8, 2010, pp. 574–581.
Muchuweti, D. and E. Muguti. “Penetrating thoracoabdominal injuries from multiple-spiked spear stabbing: Case report and literature review.” Clinical Case Reports, vol. 8, no. 6, 2020, pp. 1002–1006. https://doi.org/10.1002/ccr3.2809.
Thiam, O. et al. “Traumatic DIAPHRAGMATIC INJURIES: EPIDEMIOLOGICAL, DIAGNOSTIC AND THERAPEUTIC ASPECTS.” SpringerPlus, vol. 5, no. 1, 2016, pp. 1–6. https://doi.org/10.1186/s40064-016-3291-1.
Petrowsky, H. et al. “A quarter century experience in liver trauma: A plea for early computed tomography and conservative management for all hemodynamically stable patients.” 2012.
Shanmuganathan, K. and J. Matsumoto. “Imaging of penetrating chest trauma.” Radiologic Clinics of North America, vol. 44, no. 2, 2006, pp. 225–238.
Shorr, R. et al. “Blunt thoracic trauma: Analysis of 515 patients.” Annals of Surgery, vol. 206, no. 2, 1987, pp. 200–205.
McEwan, K. and P. Thompson. “Ultrasound to detect hemothorax after chest injury.” Emergency Medicine Journal, vol. 24, no. 8, 2007, pp. 581–582.
