
+91 6002993949
submission@iarconsortium.org
Open Access
ISSN (Print) : 2709-1872
ISSN (Online) : 2709-1880
Regional anesthetic technique especially upper extremity surgery with using clonidine, opioids, tramadol, corticosteroid for prolongation of anesthesia and analgesia. When administered as adjunct to Clonidine with Dexamethasone adjuvant to Bupivacaine and Lignocain with adrenaline observed early onset and prolong duration of analgesia in interscalene brachial plexus block. Aim and objective is to compare the effect of addition of dexamethasone and clonidine to local anesthetic drug in (0.5% Bupivacaine+ 2% lignocaine with adrenaline) in peripheral nerve stimulator guided Interscalene brachial plexus block. Methodology: 90 patients presenting for upper limb surgery were in three groups. Group D receiving Dexamethasone 8 mg. as an adjuvant to Bupivacaine and lignocaine whereas Group C receiving Clonidine 75 mcg. as an adjuvant to bupivacaine and lignocaine and Group S as control group receiving saline as an adjuvant to bupivacaine and lignocaine with adrenaline in interscalene brachial plexus block. Results: The mean duration of motor block in group S was 5.74±0.384 hrs, whereas in group C was 8.86±0.846 hrs, and group D was 9.32±0.964 hrs on comparison showing significant difference. The mean duration of sensory block in group S was 6.86±0.38 hrs, in group C was 9.86±0.98 hrs, and group D was 10.68±0.88 hrs. with significant difference between the group. Onset of sensory and motor block was better in dexamethasone D group. Conclusions: The study conclude that dexamethasone added to bupivacaine plus lignocaine showing better efficacy in prolonging analgesia than clonidine and control group with better hemodynamic with no side effects.
Interscalene brachial plexus block is a common regional anesthetic technique used to provide anesthesia and analgesia for upper extremity surgery at our institution.[1,2] Several drugs like clonidine, opioids, tramadol are corticosteroid have been used for prolongation of anesthesia and analgesia.[3,4]
Clonidine is an alpha-2 receptor agonist that provides a distinct benefit as adjunct to Brachial plexus block at doses of up to 150 µg without major side effects. [5,6] The time for rescue analgesia was the longest in patients who received 1.5 μg/kg of clonidine compared with tramadol and 21 min when compared with 1 μg/kg clonidine. 25 ml 0.5%bupivacaine and 30μgm (0.2 ml) which also prolongs block and enhances brachial plexus blockade compared addition of 150mcg of clonidine. [7,8]
Several studies have observed early onset and prolong duration of analgesia with the use of Dexamethasone, in Brachial Plexus Block.Dexamethasone is also a better adjuvant compared to clonidine with local anesthetics in brachial plexus block without significant side effects. Dexamethasone use as adjuvant to 1.5%lignocaine with adrenaline in brachial plexus block has increasing success rate, block characteristics and post-operative analgesic requirement. The difference in onset time in other studies used lignocaine-bupivacaine as local anaesthetics was also obsereved.[9-11]
This prospective study was conducted at Rajshree Medical Research Institute & Hospital, Bareilly, on 90 patients undergoing upper limb surgery and were divided into three groups of thirty patients each (n=30).
Group – C: Patients received 0.5% Bupivacaine plus lignocaine with adrenaline and clonidine 75 micro grams making it total volume of 35ml
Group – D: Patients received 0.5% Bupivacaine plus lignocaine with adrenaline and dexamethasone 8 mg making it total volume of 35ml.
Group – S: patients received 0.5% Bupivacaine plus lignocaine and saline making it total volume of 35ml.
Patient of age group of 18-60 years with ASA class – I and Class –II for upper limb surgery of fracture clavicle, proximal humerus Fracture were included in the study.
However, Refusal patient, ASA grade: grade III & IV, Bleeding disorders and patient on anticoagulants, local infection at injection site of injection and history of allergy to local anesthetics were excluded from the study. Informed consent was obtained from every patient and explanations and reassured about the procedure were made. In pre-operative room IV cannulation and premedication consisted of 1–2 mg IV midazolam given to all patients. The patients were shifted to operation theater and monitored ECG, SPO2 and noninvasive blood pressure to the patients. Interscalene block was done using nerve stimulation technique in the supine position with the head turned 45 degrees to the opposite side and arm placed by the side of the chest.
When muscle contractions were seen at stimulation current between 0.2 mA and 0.5mA at 2Hz frequency with pulse width of 0.1ms, drugs were injected.
The following parameters were studied:
The onset of sensory block was assessed by pinprick using the blunt 27-gauge needle. The sensory block was graded according to the following scale:
= no block (normal sensation),
= partial block (decreased sensation), and
= complete block (no sensation).
The Onset of motor block was measured by assessing the motor functions such as:
The motor block was graded in the following scale:
= no block (full muscle activity),
= partial block (decreased muscle activity),
= complete block (no muscle activity).
Duration of sensory block of analgesia was noted according to 0-10 Visual Analogue Score (VAS) for pain. When the patients began to experience the worst pain (VAS =8-10), was considered that analgesic action of the drugs was terminated and rescue analgesic of Diclofenac 75mg IM was given.
The duration of motor block postoperatively was assessed by asking the patients to move their fingers and to see whether they were able to raise the hand or not. This time was recorded and taken as cessation of motor block effect.
All the patients were monitored continuously throughout the procedure and during surgery with Temperature, Pulse, Non-invasive Blood Pressure, Respiratory rate, SPO2 and ECG.
Statistical analysis was done by using SPSS Statistical Software Version 20.0. Mean and standard deviation were calculated. p value of < 0.05 was considered statistically significant and p value <0.001 was considered statistically highly significant.
Figure-1:Age wise distribution of study subjects
In Figure-1 group D the mean age of the study subjects was 43.37±4.53 yrs., whereas in group C the mean age of the study subjects was 44.77±5.96 yrs., mean age of Group S 43.93±6.21 on comparing there is non-significant difference among the three groups with p value 0.63.
Table 1: The mean duration of motor block in both the study groups
group | Mean(hr.) | N | Std. Deviation | ANOVA test applied, p value- <0.001, significant |
Group D | 10.68 | 30 | 0.88 | |
Group C | 9.86 | 30 | 0.98 | |
Group S | 6.86 | 30 | 0.38 |
In Table 1 the mean duration of motor block in group S was 5.74±0.384 hrs. whereas in group C it was 8.86±0.846 hrs., and in Group D it was 9.32±0.964 hrs., on comparing with groups, there is significant difference with p value< 0.001.
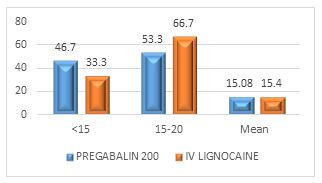
Table 2: The mean duration of sensory block in both the study groups
Table 2 shows the mean duration of sensory block in both the study groups, the mean duration of sensory block in group S was 6.86±0.38 hrs., in group D was 10.68±0.88 hrs., whereas in group C it was 9.86±0.98 hrs., on comparing with groups there is significant difference among three group, with p value< 0.001
Table 3: The mean time for onset of sensory block
Table 3 shows the mean time for onset of sensory block in three groups, the mean time for onset of sensory block in group D was 8.67±0.48 min, in group C was 11.42±1.12 min, and for group S was 11.55±2.49 min, having the groups there is significant difference with p value< 0.001.
Table 4: The mean time for onset of motor block
group | Mean(min) | N | Std. Deviation | anova test applied, p value- <0.001, significant |
Group D | 7.34 | 30 | .472 | |
Group C | 9.56 | 30 | .78 | |
Group S | 9.50 | 60 | 0.98 |
Table 4 shows the mean time for onset of motor block in three study groups, the mean time for onset of motor block in group D was 7.34±0.472 in group C was 9.56±0.877 min, and Group S was 9.50±0.98 min, there is significant difference between two group, with p value< 0.001.
In the present study, It was associated with rapid onset, provides consistent and reliable anesthesia with analgesia, and was proven to be a safe technique. The mean time for onset of sensory block in group D was 8.67±0.48 min, group C was 11.42±1.12 min, and group S was 11.55±2.49 min, on comparing there is significant difference among the three group, with p value< 0.001. The mean time for onset of motor block in group D was 7.34±0.472, in group C was 9.56±0.877 min, and for Group S was 9.50±0.98 min, there is significant difference between two group, with p value< 0.001. The experience of the anesthetist was significantly less with the Truview laryngoscope as compared with Macintosh laryngoscope are limitations of this study. [1] reported that Dexamethasone added to the local anesthetic is an efficient and safe choice for rapid onset and increased the duration of sensory and motor block in brachial plexus block. [2] found that addition of dexamethasone in brachial plexus block prolonged duration of sensory and motor block with faster onset. [4] also found that dexamethasone significantly increases the duration of action of motor and sensory block. [5] reported that Dexamethasone prolongs the duration of motor block and analgesia and Dexamethasone has clearly outperformed clonidine as a potent adjuvant (in terms of onset and duration of analgesia and anesthesia). [6] reported cffect of Clonidine as adjuvant in bupivacaine supraclavicular Brachialplexus block. [7] compared two different doses of Clonidine added to bupivacaine Brachial plexus block. The present study are comparable with a recent meta-analysis done [8] using clonidine as an adjuvant to local anesthetic for peripheral nerve and plexus blocks in a meta-analysis of randomized trials. [9] studied addition of clonidine to local anesthetic for peripheral nerve blockade and documented a significant prolongation of sensory and motor blockade without any alteration in hemodynamic stability with the addition of clonidine. [10] reported that Dexamethasone has clearly outperformed clonidine as a potent adjuvant in terms of onset and duration of analgesia and anesthesia when used in supraclavicular brachial plexus block. Corticosteroids have been shown to prolong the nerve block effect by impeding the transmission of pain-carrying type-c myelinated fibers and repressing the ectopic neuronal discharge. [9] reported adding clonidine to intermediate or long-acting local anesthetics prolong the duration of analgesia and motor block for peripheral nerve or plexus blocks. [10] compared dexamethasone and clonidine as an adjuvant in ultrasound guided supraclavicular brachial plexus block. [11] conclude that Clonidine provides the fastest onset of sensory as well as motor block and the longest duration of postoperative analgesia compared to tramadol and a good additive to local anesthetic solutions for brachial plexus blocks. Clonidine augments the sodium channel blockade action of local anesthetics by opening up the potassium channels, leading to membrane hyperpolarization, a state in which the cell becomes unresponsive to any excitatory input.
The recent studies have highlighted the importance of the use of Dexamethasone and Clonidine as an adjuvant to Bupivacaine and Lignocain with adrenaline in peripheral nerve stimulator guided Interscelene Brachial plexus block and dexamethasone proves to be a better adjuvant as compared to clonidine given its availability, cost-effectiveness, longer duration of analgesia, lack of adverse effects, lesser requirement of postoperative analgesia, and more patient satisfaction. In terms of the onset of sensory and motor blocks and maintaining hemodynamics. Dexamethasone is higher to clonidine in effectiveness. The study concluded that dexamethasone added to bupivacaine plus lignocaine are of better efficacy in prolonging analgesia and duration and faster onset of motor and sensory block than clonidine.
The authors declare that they have no conflict of interest
No funding sources
The study was approved by the Rajshree Medical Research Institute, Bareilly, Uttar Pradesh.
Anupama, M. K., & Alur, T. R. Dexamethasone as an adjuvant in brachial plexus block: Supraclavicular approach: An observational randomized double-blind clinical study. [Publication details missing].
Bindal, D., Narang, N., Mahindra, R., et al. Effect of dexamethasone on characteristics of supraclavicular nerve block with bupivacaine and ropivacaine: A prospective, double-blind, randomized control trial. Anesthesia Essays and Research, 2018, 12(1), 234–239. doi:10.4103/aer.aer_40_18.
Estebe, J. P., Le Corry, P., Clement, R., Duplessis, L., Chevenne, F., et al. (2003). Effect of dexamethasone on motor brachial plexus block with bupivacaine and bupivacaine-loaded microspheres in a sheep model. European Journal of Anaesthesiology, 20(4), 305-310. doi:10.1017/S0265021503000161.
Cummings, K. C., Napierkowski, D. E., Parra-Sanchez, A., Kurz, A., Dalton, J. E., Brems, J. J., & Sessler, D. I. (2011). Effect of dexamethasone on the duration of interscalene nerve blocks with ropivacaine or bupivacaine. British Journal of Anaesthesia, 107(3), 446-453. doi:10.1093/bja/aer159.
Chakraborthy, S., Chakraborthy, J., & Mandal, M. C. (2010). Effect of clonidine as an adjuvant in bupivacaine supraclavicular brachial plexus block: A randomized controlled trial. Indian Journal of Pharmacology, 42(2), 74-77. doi:10.4103/0253-7613.60793.
Kohli, M. S., & Sahoo, S. (2013). Brachial plexus block: Comparison of two different doses of clonidine added to bupivacaine. Journal of Anaesthesiology and Clinical Pharmacology, 29(4), 469-473. doi:10.4103/0970-9185.117243.
Popping, D. M., Elia, N., Marret, E., Wenk, M., & Tramèr, M. R. (2009). Clonidine as an adjuvant to local anaesthetic for peripheral nerve and plexus blocks: A meta-analysis of randomized trials. Anesthesiology, 111, 406-415. doi:10.1097/ALN.0b013e3181a327fc.
McCartney, C. J. L., Duggan, E., & Apatu, E. (2007). Should we add clonidine to local anesthetic for peripheral nerve blockade? A qualitative systematic review of the literature. Regional Anesthesia and Pain Medicine, 32(4), 330-338. doi:10.1016/j.rapm.2007.02.010.
Kumar, C. P. N., & Smitha, Y. (2019). Comparison of dexamethasone and clonidine as an adjuvant in ultrasound-guided supraclavicular brachial plexus block: A prospective, randomized study. MedPulse International Journal of Anesthesiology, 12, 234-237. doi:10.26611/10161234.
Kelika, P., & Jamkar, M. A. (2017). Evaluation of clonidine as an adjuvant to brachial plexus block and its comparison with tramadol. Journal of Anaesthesiology and Clinical Pharmacology, 33(2), 197–202. doi:10.4103/0970-9185.205156.
Prakash Kelika, Jamkar Maya Arun: Evaluation of clonidine as an adjuvant to brachial plexus block and its comparison with tramadol J Anaesthesiol Clin Pharmacol.2017 Apr-Jun; 33(2): 197–202.
