
+91 6002993949
submission@iarconsortium.org
Open Access
ISSN (Print) : 2709-1872
ISSN (Online) : 2709-1880
Background: Today, both general and regional anesthesia (spinal, epidural and combined spinal-epidural) techniques are applied to the patients who will be applying cesarean section. Both anesthesia techniques used in the cesarean section have their own advantages and disadvantages. In our study, we aimed to compare the maternal and neonatal effects of spinal anesthesia and general anesthesia using remifentanil. Materials and Methods: Sixty-six pregnant women with ASA I-II physical status were included in the study. Patients were randomly divided into two groups general anesthesia and spinal anesthesia. A computer-generated randomization program using a random block size was used. The age, height, weight and gestational week of each patient were recorded in the operation room. Systolic Arterial Pressure (SAP), Diastolic Arterial Pressure (DAP), Mean Arterial Pressure (MAP), Peripheral Oxygen Saturation (SPO2) and Heart Rate (HR) were measured and the values were recorded as baseline values. The 1st and 5th min. Activity-Pulse-Grimace-Appearance-Respiration (APGAR) values of the newborns were evaluated by the same pediatrician. Umbilical artery blood gas, 2nd-hour and 24th-hour Neurologic and Adaptive Capacity Scoring System (NACS) values of all newborns were recorded. Anesthesia since newborn hatching, uterine incision-infant hatching, duration of anesthesia and neonatal resuscitation (mask ventilation or intubation) were recorded in both groups. Postoperatively the first time the newborn can receive their mother's breast as effectively as the absorption time was recorded. Results: SAB values were higher in the general anesthesia group and there was a statistically significant difference between the groups (p-value = 0.00 *). In the same way, after the patients undergoing spinal/intubation, 5th, 10th and 15th min. Mean Arterial Pressure (MAP) and Diastolic Arterial Pressure (DAB) values were higher in the general anesthesia group and there was a statistically significant difference between the groups (p-value = 0.00*). Conclusion: We think that general anesthesia performed with remifentanil and thiopental used in the elective cesarean section may be applied as an alternative to spinal anesthesia in terms of mother and newborn health.
Today, both general and regional anesthesia (spinal, epidural and combined spinal-epidural) techniques are applied to the patients who will be applying cesarean section. In a normal surgical procedure, only one person's safety and optimal conditions should be ensured and the fetus affected by any changes in the mother and mother must be secured during the cesarean section. This gives a distinctive feature to cesarean anesthesia [1]. Both anesthesia techniques used in a cesarean section have their own advantages and disadvantages. Advantages of general anesthesia in cesarean section; providing fast induction, less hypotension and less cardiovascular depression, allowing better airway and respiratory control. In recent years, the more frequently preferred regional anesthesia is cesarean section; The patient has advantages such as being conscious, not carrying the risk of aspiration, not causing a respiratory depression in the newborn and not causing uterine atony [2,3].
The risks of general anesthesia in cesarean operations are a pulmonary aspiration of gastric contents and difficulty in intubation [4,5]. Difficult intubation is the leading cause of maternal mortality due to anesthesia. In patients undergoing obstetric surgery under general anesthesia, there is a higher rate of intubation compared to other surgical patients [6,7]. However, hypotension due to sympathetic blockade in spinal anesthesia applied in cesarean may adversely affect uteroplacental blood flow and may cause fetal distress. The inhalation anesthetics and Intravenous (IV) anesthetics used in general anesthesia reduce blood pressure and, ultimately, uterorelaxant. They also cause fetal depression in very few cases. Because of the rapid onset and rapid termination of the remifentanil effect, which is metabolized independently of the organ by nonspecific plasma esterases, it may be possible to prevent maternal hemodynamic stability and to be aware of it without neonatal depression [6,7].
In our study, we aimed to compare the maternal and neonatal effects of spinal anesthesia and general anesthesia using remifentanil.
Patients
An elective cesarean section was included in 60 pregnant women with ASA I-II status who were 18 years and older. Case reports, fetal anomaly, fetal growth retardation, Rh incompatibility and congenital malformations such as obstetric complications and cases less than 2500 grams of the fetus were excluded from the study.
Study Protocol
The study was carried out with the approval of the Ethics Committee of Meram Medical Faculty of the University of Selcuk (2011/017 dated 27.01.2011). All patients were informed about the preoperative operation and their approvals were obtained. Patients were randomly divided into two groups general anesthesia and spinal anesthesia. A computer-generated randomization program using a random block size was used. After all, patients were taken to the operation room, IV injection was performed with an 18 G cannula and 10 mL/kg isotonic was given and they were kept in a 15° left lateral tilt position until the end of the operation. In both groups, 100% O2 and 3-5 minutes of preoxygenation were applied to the cases. The age, height, weight and gestational week of each patient were recorded in the operation room. Systolic Arterial Pressure (SAD), Diastolic Arterial Pressure (DAB), Mean Arterial Pressure (MAP), Peripheral Oxygen Saturation (SPO2) and Heart Rate (HR) were measured and the values were recorded as baseline values. The same measurements were recorded after intubation in the general anesthesia group, 5 minutes after the operation started and repeated every 5 minutes until the end of the operation. 10IU oxytocin was slowly given IV in both groups. 10-20 units of oxytocin were added into 1000 ml of isotonic.
The 1st and 5th min APGAR values of the newborns were evaluated by the same pediatrician. Umbilical artery blood gas 2nd-hour and 24th-hour NACS values of all newborns were recorded. In both groups, the onset of anesthesia-infant hatching, uterine incision, infant hatching and anesthesia duration, resuscitation requirement of the newborn (mask ventilation or intubation) was recorded.
The patients in the Spinal Anesthesia group were recorded 5 minutes after the operation was started and every 5 minutes at the end of the operation. After the skin disinfection with the appropriate antiseptic solution was provided to all pregnant women, a 25 G atraumatic spinal needle from the L3-L4 interval was entered into the subarachnoid space. Bupivacaine 10mg was given after the free, clear CSF flow. In the case of significant hypotension in the spinal anesthesia group (starting from 20-30% of the initial SOD), ephedrine 5-10 mg IV bolus was performed. 20 mg IV tenoxicam was administered to the spinal anesthesia group after the delivery of the baby for postoperative analgesia.
In the general anesthesia group, a dose of 0.5 μg/kg remifentanil was given as a bolus in 30 sec and then infused at 0.2 μg/kg/min. İntravenously. The induction was completed with 1.5 mg/kg thiopental and 1 mg/kg succinylcholine. Endotracheal intubation was performed after muscle relaxation. Anesthesia was maintained with remifentanil infusion (0.2 μg/kg/min) at 50% O2 + 50% N2O. At the end of the operation, remifentanil infusion was closed when the fascia was closed, N2O was closed and 100% O2 was given. In order to provide postoperative analgesia, 2 mg/kg tramadol and a 20 mg IV bolus of tenoxicam were administered to the general anesthesia group.
When there was a sign of wakefulness in the general anesthesia group (eye-opening, eye wrinkling, hand-foot motor response) or SAB increased by 25% compared to baseline, remifentanil dose was increased by 25%; The remifentanil dose was reduced by 25% when SAB was 25% below baseline or below 90 mmHg. The reduction of HR to less than 50 per minute was accepted as bradycardia and a bolus of atropine 0.5 mg was planned.
In both groups, the onset of anesthesia, infant hatching, uterine incision, infant hatching and anesthesia duration, resuscitation requirement of the newborn (mask ventilation or intubation) was recorded. In the postoperative period, the first time that the newborn could effectively receive the mother's breast was recorded as sucking time. All neonates were monitored by a pediatrician for 30 min after cesarean section. In terms of side effects that may develop in the newborn, physical conditions, masking devices and all kinds of resuscitation equipment were made available for mask ventilation and endotracheal intubation.
Statistical Analysis
SPSS 22 (IBM, Armonk, NY) version was used for statistical analysis. In the case of the normal distribution of quantitative data, it is compared with the student’s t-test. Otherwise, the Mann-Whitney U test was used. Qualitative data were compared with Pearson's chi-square test. A p-value of less than 0.05 was considered statistically significant.
Sixty patients were enrolled in the study and these patients were divided into two equal groups. Demographic data of both groups were compared in terms of age, weight, height and gestational week (Table 1).
Table 1: Demographic Data of Cases (Mean±SD)
| Variables | Spinal Anesthesia Group (n = 30) | General Anesthesia Group (n = 30) | p-value |
| Age (year) | 30,73±4,99 | 29,00±5,05 | 0,18 |
| Height (cm) | 159,80±20,37 | 162,10±6,27 | 0,55 |
| Weight (kg) | 79,73±12,00 | 77,03±11,33 | 0,37 |
| Gestational (week) | 38,23±0,81 | 38,10±0,71 | 0,50 |
Table 2: Comparison of SAP Mean Values of Groups (mmHg) (Mean±SD)
| Variables | Spinal Anesthesia Group (n = 30) | General Anesthesia Group (n = 30) | p-value |
| Baseline | 132,13±17,23 | 134,27±12,34 | 0,58 |
| After Spinal/Int. | 128,57±18,44 | 142,40±20,76* | 0,00* |
| 5. min. | 115,20±19,58 | 134,90±16,70* | 0,00* |
| 10. min. | 123,47±12,83 | 133,33±14,14* | 0,00* |
| 15. min. | 116,70±14,04 | 126,57±13,75* | 0,00* |
* p-value <0,01 Significant Difference
Table 3: 1st and 5th min. APGAR Values (Mean±SD)
| Variables | Spinal Anesthesia Group (n = 30) | General Anesthesia Group (n = 30) | p-value |
| APGAR 1st | 8,00±1,08 | 8,00±1,35 | 0,56 |
| APGAR 5th | 10,00±0,50 | 9,00±0,54 | 0,10 |
Table 4: 2nd and 24th min. NACS Values (Mean±SD)
| Variables | Spinal Anesthesia Group (n = 30) | General Anesthesia Group (n = 30) | p-value |
| NACS 2nd h. | 38,00±1,58 | 37,50±1,63 | 0,51 |
| NACS 24th h. | 40,00±0,98 | 39,00±1,17 | 0,06 |
Table 5: Comparison of Groups Anesthesia, Infant Hatching and Absorption Times (Mean±SD)
| Variables | Spinal Anesthesia Group (n = 30) | General Anesthesia Group (n = 30) | p-value |
| Anesthesia time (min.) | 37,60±6,52* | 31,30±5,14 | 0,00* |
| Spinal/Induction- infant hatching (sec.) | 806,57±204,60* | 331,47±66,56 | 0,00* |
| Uterus incision infant hatching (sec.) | 29,23±6,35 | 29,60±6,06 | 0,82 |
| Breast-feeding (min.) | 60,43±27,58* | 47,47±21,59 | 0,04* |
*p-value <0,01 Significant Difference
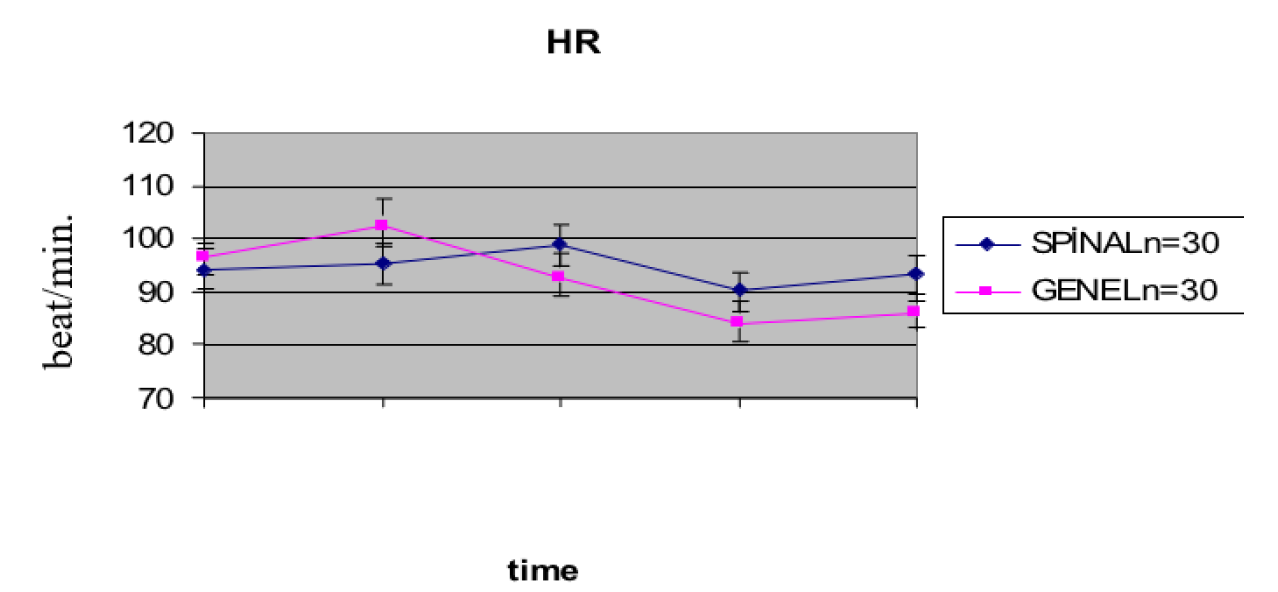
Figure 1: Comparison of Mean Values of HR in Groups (Beat/min.) (Mean±SD)
There was no statistically significant difference between the groups in terms of demographic data (p-value > 0.05).
There was no significant difference between spinal and general anesthesia groups in the baseline, after spinal/intubation, Heart Rate (HR) values of the 5th, 10th and 15th minutes of operation (p-value >0.05) (Figure 1).
Systolic Arterial Pressure (SAP) values of the cases are shown in Table 2. There was no statistically significant difference between the groups in terms of basal SAP values (p-value >0.05). After spinal/intubation, 5th, 10th and 15th min. SAP values were higher in the general anesthesia group and there was a statistically significant difference between the groups (p-value <0,01). In the same way, after the patients undergoing spinal/intubation, 5th, 10th and 15th min. of Mean Arterial Pressure (MAP) and Diastolic Arterial Pressure (DAP) values were higher in the general anesthesia group and there was a statistically significant difference between the groups (p-value <0,01).
APGAR and NACS values of newborns are shown in Table 3 and Table 4. There was no significant difference between the 1st and 5th minute APGAR values and the 2nd and 24th hour NACS values (p-value >0.05).
Total anesthesia time, spinal/induction-infant hatching and suction time were shorter in the general anesthesia group and there was a statistically significant difference between the groups (p-value <0.01) (Table 5)
In the spinal anesthesia group, 3 (10%) neonates and 4 (13%) newborns in the general anesthesia group received mask ventilation. There was no statistically significant difference between the groups (p-value >0.05). None of the newborns in both groups required endotracheal intubation, intensive care follow-up and naloxone.
In this study, it has been concluded that the use of remifentanil at the doses specified in the induction in general anesthesia is not affected by APGAR values, NACS values, respiratory depression status, or umbilical artery blood gas values.
In recent years, there have been reports that remifentanil can be used safely at appropriate doses in pregnant women. The fetal and neonatal effects of the anesthetic agents given to the mother in general anesthesia depend on the amount of the drug reaching the fetus [8]. Intravenous agents and inhalation agents used in general anesthesia may cause fetal depression, low APGAR and NACS values, fetal acidosis and late absorption [9] and prevent being aware.
Hypotension is the biggest problem encountered in spinal anesthesia in pregnant women. The sudden disappearance of sympathetic activation in regional anesthesia results in hypotension. In addition, inferior vena cava compression and aortic occlusion of the uterus in the supine position cause a decrease in the venous return to the heart, resulting in deeper hypotension [10].
Mueller et al. reported that maternal arterial hypotension was the most common complication in cesarean section by regional anesthesia in 5806 case epidemiological studies. They also stated that hypotension might cause fetal acidosis due to its negative effect on uteroplacental blood flow [11]. In obstetric spinal anesthesia, methods such as tilting the uterus to the left to prevent hypotension, using compression sock, preoperative volume loading and vasopressor are used [12].
In our study, 10 mL/kg isotonic was given to all pregnant women undergoing spinal anesthesia. Hypotension (falling below baseline from 20-30%) occurred in 5 pregnant women who underwent spinal anesthesia. In order to correct hypotension in these pregnant women, maintenance fluid was increased, or 5-10 mg ephedrine was applied.
Kavak et al., in their study investigating the effects of general and spinal anesthesia on umbilical cord blood gas in 84 patients, found that pH, PO2, PCO2 and HCO3 values were similar in both groups [13]. In our study, no difference was found between the pH, PCO2, PO2 and HCO3 values in umbilical blood gas compared to the general anesthesia group of the spinal anesthesia group. The results of this study were consistent with the results of Kavak et al., Marx et al. [13].
Data et al., Hodgson et al. and Dyer et al. investigated the effects of general and spinal anesthesia on fetal well-being. They found that APGAR values in 1st min. were higher in the spinal anesthesia group and APGAR values in 5th min. were similar in both groups. In our study, APGAR values of 1st and 5th min. of all newborns were evaluated. No statistically significant difference was found between the APGAR values at the 1st and 5th min. When comparing both types of anesthesia. The number of newborns with APGAR values below seven was found to be 4 in the general anesthesia group and 3 in the spinal anesthesia group. The APGAR values of all newborns at the 5th min. were higher than 7 [14-16].
In Özden et al.’s studies, it was given a dose of 0.5 µg/kg remifentanil bolus in general anesthesia and continued to infuse at a dose of 0.2 µg/kg/min. There was no difference between APGAR, NACS and umbilical blood gases between the group used with remifentanil and the unused group [17]. In our study, NACS values of newborns were evaluated at the 2nd and 24th hours. There was no difference between NACS values at the 2nd and 24th hours between the two groups. NACS values of all newborns at the 2nd and 24th hours were over 35 in both groups.
In a study by Sener et al., The time that the newborn first absorbed the mother was shorter in the regional anesthesia group than in the general anesthesia group [18]. In our study, the time that the newborn first absorbed the mother was shorter in the general anesthesia group than in the spinal anesthesia group. We believe that this may be due to the lower dose of the drugs used in the general anesthesia group and the rapid metabolization of remifentanil in the fetus due to the fact that the newborn is less affected by general anesthetic drugs.
In addition, the reason for the prolongation of the newborn first absorbed the mother's time undergoing spinal anesthesia is that the pregnant women are kept in the operating room or in the wake room after the operation because this situation causes mothers to reach their babies late.
As a result, it was concluded that remifentanil infusion and thiopental use in general anesthesia in cesarean operations compared to spinal anesthesia, umbilical artery blood gases, APGAR values and NACS values were not different. In addition, it was found that neonates absorbed the mother's breast earlier due to the use of remifentanil and thiopental in cesarean operations. We think that general anesthesia performed with remifentanil and thiopental used in the elective cesarean section may be applied as an alternative to spinal anesthesia in terms of mother and newborn health.
Reporting Checklist
We present the following article in accordance with the CONSORT reporting checklist.
Conflict of Interest
All authors have completed the IARC uniform disclosure form. The authors have no conflicts of interest to declare.
M. Erdem et al. "Temel Kadın Hastalıkları ve Doğum Bilgisi. Ankara : Melisa Matbaacılık," Obstetrik Anestezi ve Analjezi. 1996, pp. 173–186.
F.G. Cunningham et al. Williams Obstetrics. Vol. 21, McGraw-Hill Professional, New York, 2005.
T. Purtuloğlu et al. "Elektif sezaryen uygulanan olgularda genel ve spinal anestezinin maternal ve fetal etkilerinin karşilaştirilması." Gülhane Tıp Dergisi, vol. 50, 2008, pp. 91–97.
T. Cook et al. "Major complications of airway management in the UK: Results of the fourth national audit project of the royal college of anaesthetists and the difficult airway society. Part 1: Anaesthesia." British Journal of Anaesthesia, vol. 106, no. 5, 2011, pp. 617–631.
S. Kinsella "Anaesthetic deaths in the CMACE (Centre for Maternal and Child Enquiries) saving mothers’ lives report 2006–08." Anaesthesia, vol. 66, no. 4, 2011, pp. 243–246.
M. Van de Velde et al. "General Anaesthesia with target-controlled infusion of propofol for planned caesarean section: maternal and neonatal effects of a remifentanil-based technique." International Journal of Obstetric Anesthesia, vol. 13, no. 3, 2004, pp. 153–158.
W.D.N. Kee et al. "Maternal and neonatal effects of remifentanil at induction of general anesthesia for cesarean delivery: A randomized, double-blind, controlled trial." Anesthesiology: The Journal of the American Society of Anesthesiologists, vol. 104, no. 1, 2006, pp. 14–20.
J. Littleford "Effects on the fetus and newborn of maternal analgesia and anesthesia: A review." Canadian Journal of Anesthesia, vol. 51, no. 6, 2004, pp. 586–609.
F. Moya et al. "Influence of maternal hyperventilation on the newborn infant." American Journal of Obstetrics and Gynecology, vol. 91, no. 1, 1965, pp. 76–84.
A. Jadon "Complications of regional and general anaesthesia in obstetric practice." Indian Journal of Anaesthesia, vol. 54, no. 5, 2010, pp. 415–415.
M.D. Mueller et al. "Higher rate of fetal acidemia after regional anesthesia for elective cesarean delivery." Obstetrics and Gynecology, vol. 90, no. 1, 1997, pp. 131–134.
W. Gogarten "Spinal anaesthesia for obstetrics." Best Practice and Research Clinical Anaesthesiology, vol. 17, no. 3, 2003, pp. 377–392.
Z.N. Kavak et al. "Short-term outcome of newborn infants: spinal versus general anesthesia for elective cesarean section: A prospective randomized study." European Journal of Obstetrics and Gynecology and Reproductive Biology, vol. 100, no. 1, 2001, pp. 50–54.
S. Datta et al. "Neonatal effect of prolonged anesthetic induction for cesarean section." Obstetrics and Gynecology, vol. 58, no. 3, 1981, pp. 331–335.
C. Hodgson et al. "A comparison of spinal and general anaesthesia for elective caesarean section: Effect on neonatal condition at birth." International Journal of Obstetric Anesthesia, vol. 3, no. 1, 1994, pp. 25–30.
R.A. Dyer et al. "Prospective, randomized trial comparing general with spinal anesthesia for cesarean delivery in preeclamptic patients with a nonreassuring fetal heart trace." Anesthesiology: The Journal of the American Society of Anesthesiologists, vol. 99, no. 3, 2003, pp. 561–569.
M. Özden et al. "Maternal and neonatal effects of remifentanil at induction and maintenance of anesthesia for cesarean delivery." Turkiye Klinikleri Journal of Anesthesiology and Reanimation, vol. 9, no. 1, 2011, pp. 7–7.
E.B. Sener et al. "Comparison of neonatal effects of epidural and general anesthesia for cesarean section." Gynecologic and Obstetric Investigation, vol. 55, no. 1, 2003, pp. 41–45.
