
+91 6002993949
submission@iarconsortium.org
Open Access
ISSN (Print) : 2709-1872
ISSN (Online) : 2709-1880
The purpose of this placebo-controlled, double-blind study was to see how magnesium sulphate and clonidine affected perioperative hemodynamics, propofol consumption, and postoperative recovery. Ninety ASA I–II patients undergoing elective laparoscopic surgery were randomized into three groups. Group M Patients received Inj. magnesium sulphate (40mg/kg) in 20 ml saline infused over a period of 15 minutes before induction. Group C received Patients received Inj. Clonidine (3mcg/kg) before induction. The Group S (Control group) received 20ml normal saline over 15mind before induction. Propofol was used for induction of anaesthesia and for maintenance propofol infusion was used which was adjusted as per bispectral index along with intermittent fentanyl bolus and vecuronium as muscle relaxant According to type of data, different tests of statistical significance like Chi-square test, Kruskal Wallis test and one-way ANOVA were used. In the presence of magnesium sulphate and clonidine, propofol induction was rapid. The time it took for BIS to reach 60 was significantly shorter in groups M and C (P0.0001), and compared to clonidine and control group post-operative recovery was more delayed in magnesium sulphate group (P0.0001). There was no statistically significant difference between the groups in heart rate or arterial blood pressure. Preoperative use of magnesium sulphate and clonidine resulted in significant reduction in propofol requirements for induction as well as for maintenance (P0.0001). To conclude use of magnesium sulphate caused delayed recovery and hypotension and bradycardia was observed with clonidine, but both can be used as adjuvants with caution.
The use of intravenous anaesthesia has been pestered by two parallel problems, the unavailability of satisfactory drugs and inadequate methods of administration, resulting in either under dosage or over dosage and almost invariably in excessively long recovery times. Both of these problems have now been resolved. With the introduction of computerized infusion pumps, short acting hypnotics, opioids, and muscle relaxant and with our sophisticated monitoring devices and anaesthesia delivery system, we can provide truly balanced anaesthesia with TIVA. As a result of this enthusiasm for total intravenous anaesthesia (TIVA) has markedly increased.
With TIVA it is possible to provide balanced anaesthesia by selecting a pure short acting hypnotic such as propofol and opioid together with a muscle relaxant. By titrating each of these different drugs independently to achieve the desired levels of hypnosis, analgesia and relaxation it is possible to adjust anaesthesia as per the needs of individual patient according to surgical stimulation. [1]
Clonidine is alpha-2 adrenoreceptor agonists, it produces both preoperative sedation and anxiolysis. The potential benefits of using alpha-2 agonists during anaesthesia include, reduced sympathoadrenal responses to laryngoscopy, decreased intraoperative need for volatile and intravenous anaesthetics, improved intraoperative hemodynamic stability, and decreased postoperative pain. [2]
Intravenous magnesium sulphate has been used empirically for many years as an antiarrhythmic agent and for seizure prevention in pre-eclampsia. [3] Various authors have suggested that magnesium has got the potential to treat and prevent pain by acting as an antagonist of N-methyl-D-aspartate (NMDA) receptors. [4, 5] Magnesium has been shown in clinical studies to reduce analgesic requirements during the postoperative period. [6]
Various authors have already demonstrated efficacy of clonidine and magnesium sulphate as adjunct to general anaesthesia in providing intraoperative hemodynamic stability and decreased anaesthetic consumption, their use can lead to reduced cost of anaesthesia as result of decreased anaesthetic consumption, hence they can provide us a good and economic alternative to traditional inhalational anaesthesia.
Hence this randomized, placebo-controlled study was designed to assess the effects of I.V. magnesium sulphate and I.V clonidine when used as adjuvant agents, they have an effect on intraoperative hemodynamics, propofol consumption, and postoperative recovery.
Informed consent was obtained from each patient once the hospital ethics committee approved the study. The study included 90 ASA I–II patients (47 female, 43 male) undergoing elective laparoscopic surgery who were randomly assigned to one of three groups: Group M (magnesium sulphate group), Group C (clonidine group) and Group S (control group). Exclusion criteria included ASA grade III –V hypertension, morbid obesity, drug or alcohol abuse, and severe hepatic, endocrine and cardiac dysfunction. Pre-anaesthetic preparation of patients included a period of overnight fasting. All patients received 10mg diazepam orally at night before surgery. Patients were educated regarding use of Visual Analogue Scale.
A meticulous airway assessment was also carried out. Before the induction of anaesthesia, routine monitoring (ECG, pulse oximetry, Non-invasive blood pressure NIBP) was started and an I.V. line was secured. The level of anaesthesia was monitored with bispectral index (BISTM). After thorough cleaning the forehead, the BIS electrodes were put on the patient's forehead and then attached to an A-2000 BIS monitoring system (Aspect Medical Systems, Framingham, MA, USA). For surgical anaesthesia, a BIS of 40–60 was the target range. Group M: Patients received Inj. magnesium sulphate (40mg/kg) in 20 ml saline infused over a period of 15 minutes before induction. Group C: Patients received Inj. Clonidine (3mcg/kg) in 20 ml saline infused over a period of 15 minutes before induction. Group S: Control group patient received Normal saline 20ml infused over a Period of 15 minutes before induction, Premedication in the form of inj. glycopyrrolate 4 mcg/kg of body weight IV and inj. fentanyl 2mcg/kg of body weight IV was given 10 min before induction.
After premedication patients were preoxygenated for 5 minutes, Patient were then induced with inj. Propofol 2-2.5mg/kg IV as induction agent in all groups over 30 sec- 1min till BIS was below 60 this time was noted (eye lash reflex was absent by this time). Inj. succinylcholine chloride 1.5 – 2 mg/kg IV was given as depolarising muscle relaxant to facilitate the tracheal intubation, maintenance of anaesthesia was done with 50:50 O2: Air mixture and continuous propofol infusion (by B- Braun infusion pump), started at the rate of 10mg/kg/hr and titrated to maintain BIS in the range of 40-60. Muscular relaxation was achieved by vecuronium bromide. Propofol consumption was noted every hour.During intraoperative period while BIS was between 40 to 60, if patient developed tachycardia or hypertension then it was assumed that it was because of insufficient analgesia and fentanyl 1mcg/kg bolus was given.
Intraoperatively pulse rate, systolic blood pressure, diastolic blood pressure, SpO2, BIS (Bispectral index) and EtCO2 were continuously recorded. The changes in clinical parameters were noted at following times 0,5,10,15 minutes during study drug infusion Before premedication, After premedication, After induction, At the time of laryngoscopy and intubation, At 0,2,4,6,8, 10 minutes after intubation, Every 5 minutes thereafter.
At the end of the surgical procedure, propofol infusion was stopped. Total intraoperative propofol consumption excluding induction dose was calculated and divided by patient’s body weight and total duration of surgery and calculated as mg/kg/hr and noted as intraoperative maintenance dose of propofol. After stopping propofol infusion time for BIS to reach 80 was noted. Residual neuromuscular block was reversed with appropriate doses of inj. Neostigmine 0.05mg/kg and inj. glycopyrrolate 8mcg/kg I.V. after ensuring patients spontaneous respiratory efforts and once he met all the extubation criteria’s tracheal extubation was performed and following times were noted down from stopping propofol infusion, i) Time to tracheal extubation, ii) Time to respond to verbal commands, iii) time for Orientation (to recollect name, date of birth and location), the time it took to respond to a verbal command and time for orientation were measured as recovery time. Clinical parameters such as pulse rate, blood pressure, SpO2, respiratory rate was measured postoperatively, before the patient was transferred to recovery.
Recovery characteristics like orientation, consciousness, reflexes, limb movement and respiratory rate were noted. Fulfilling these criteria and patients with normal parameters were shifted to recovery room. In recovery along with basic clinical parameters, Aldrete recovery scoring and visual pain analogue scale were noted. Patients’ vital parameters were evaluated at 0, 1, 2 and 3 hrs in the recovery room and corresponding score was calculated from above mentioned parameters and was noted.
Post-operative pain intensity was also noted as per Visual analogue scale where 0- no pain and 10- excruciating pain. Patients who complained of severe pain with VAS score of >6 received inj. diclofenac sodium 1.5mg/kg intramuscularly. Patients were also observed for any adverse events or side effects during the postoperative period, Patient were then discharged from recovery room to post-surgical ward after ensuring stable vital parameters, no nausea, no vomiting, and no drowsiness and were considered to be acceptable by using standard wetchler criteria for discharge.
The results were assimilated and subjected to statistical analysis. According to type of data, different tests of statistical significance Chi-square test, Kruskal Wallis test and one-way ANOVA were used. Statistical software used in the analysis was SPSS 17.0 version and graph pad prism 5.
The three groups were analogous in terms of age, weight, height, ASA status and duration of surgery. (Table 1)
When magnesium and clonidine were used preoperatively, group M and group C had Induction time (time for BIS< 60) significantly less (p<0.001) (Table 2) compared to control group S. Between group M and group C there was no statistically significant difference (p>0.05).
When all three groups were compared for requirement of propofol as induction agent it was significantly less in group M 1.76 (0.21) mg/kg and group C 1.65 (0.15) mg/kg compared to group S 2.16 (0.23) mg /kg.
Overall requirement of induction agent (Dose of propofol) Group M 1.76 (0.21) mg/kg, Group C 1.65 (0.15) mg/kg and Group S 2.16 (0.23) mg /kg) was significantly less in group M and group C (p<0.001) compared to control group S.
The intraoperative propofol requirement was calculated by dividing total amount of propofol used intraoperatively by no of hours of surgery and labelled as mg/kg/hr dose, mean propofol requirement was calculated in all three groups and it was significantly less in group M (4.76 ± 0.54 mg/kg/hr) and group C (4.02 ± 0.52 mg/kg/hr) compared to control group S (6.78 ± 1.44 mg/kg/hr) (p<0.001). There was no statistically significant difference found between group M and C (p>0.05).
After premedication and study drug infusion mean pulse rate decreased in all three groups but it was statistically not significant (p> 0.05). Post induction we observed that pulse rate increased in control group S and decreased in group M and group C and this difference was statistically significant (p< 0.05). Post intubation and pneumoperitoneum pulse rate raised significantly in control group S (p<0.001) but though pulse rate had also increased in group M and group C it was statistically not significant (p> 0.005). intraoperatively pulse rate remained higher side in control groups S, on the other hand it gradually reduced in group M and group C and this difference was statistically significant (p<0.05). Figure 1
After premedication and study drug infusion we observed that SBP decreased in group M and C and this reduction in SBP was statistically significant (p<0.05) also there was statistically significant fall in SBP post induction in group M and group C (p<0.001) compared to control group S. Post intubation we observed statistically significant rise in SBP in control group S (p<0.001) though SBP also increased in group M and group C the values were comparable to their preoperative levels. Similar increased SBP we observed in group S, 10 minutes post intubation during pneumoperitoneum (p<0.001) which was statistically significant compared to group M and group C, During the rest of the intraoperative period SBP reduced gradually in all three study groups but there was statistically significant difference among the groups (p<0.05). Figure 2
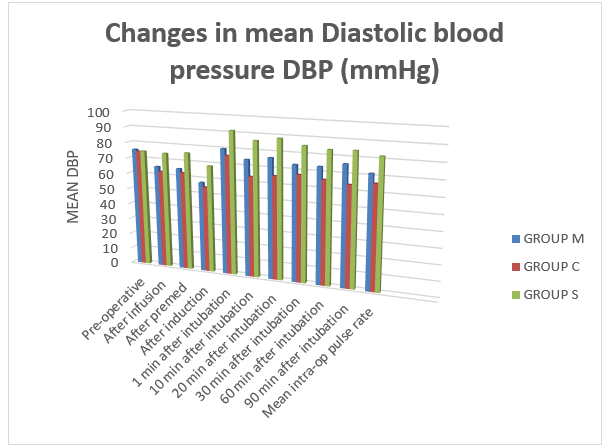
Similar to SBP we observed that post premedication and study drug infusion there was statistically significant reduction in DBP in group M and group C compared to group S (p<0.05), during laryngoscopy and intubation there was significant rise in mean DBP in group S (p<0.001) whereas though mean DBP also increased in group M and group C this rise was not statistically significant (p>0.05). During the rest of the intraoperative period DBP reduced gradually in all three study groups but there was statistically significant difference among the groups (p<0.05). Figure 3
Time for BIS to increase above 80 after stopping propofol infusion (Recovery time) was noted down in all three study drugs and we observed that mean recovery time was prolonged significantly in group M and compared to other two groups and this difference was statistically significant (p<0.001), among the group C and group S difference was statistically insignificant (p>0.05) Table 2.
We compared all three study groups for recovery parameters, extubation time, time for orientation and response to verbal commands and we observed that all recovery parameters were significantly prolonged in group M compared to other two groups and this difference was statistically significant (p<0.001), among the group C and group S difference was statistically insignificant (p>0.05) Table 3.
Table 1: Patient characteristics. Mean (SD)
| Group M | Group C | Group S | P-value | ||||
Age (yrs) | 32.6 ± 9.01
| 33.03 ± 9.97
| 30.87 ± 7.2
|
| ||||
Gender (M/F) | 13/17 | 16/14 | 14/16 | p>0.05 | ||||
Weight (kg) | 55.2 ± 7.36
| 56.2 ± 7.69
| 53.9 ± 6.03
| p>0.05
| ||||
Duration of surgery (min) | 66.5 ± 20.82
| 65.17 ± 24.54
| 68.33 ± 21.85
| p>0.05 |
Table 2: Induction and recovery periods for BIS. Mean (SD). P values were determined by comparing control (CT), magnesium (M) and clonidine (CL) groups. *Significant difference within groups
(P<0.0001)
| Group M | Group C | Group S | P-value | ||
Induction period BIS <60 (s) |
| 59.7 ± 10.7
| 82.33 ± 12.65
| P<0.001
| ||
Recovery period BIS >80 (min) |
| 6.86 ± 1.56 | 7.36 ± 2.05
| p<0.001 |
Table 3 Recovery time (min). Mean (SD). P values were determined by Comparing control, magnesium and clonidine groups. ***Significant difference Within groups (P<0.001)
| Group M | Group C | Group S | P-value | |||
Extubation time (mins) |
| 7.27 ± 1.65
| 6.4 ± 1.47 | p<0.001 | |||
Response to verbal commands(mins) |
| 8.53 ± 1.47
| 8.3 ± 1.72
| p<0.001 | |||
Time for orientation (mins) |
11.36 ± 2.28 *** |
10.66 ± 1.97 |
9.46 ± 1.71 | p<0.001 |
Figure 1: Mean pulse rate {beats/min} at various time intervals
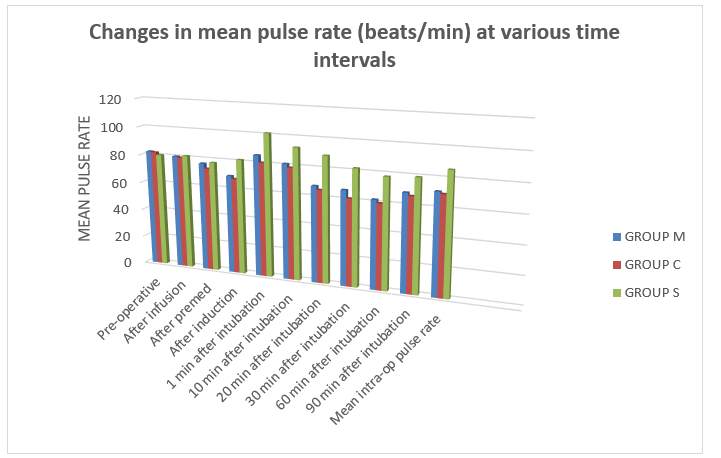
Figure 2: Showing changes in mean systolic blood pressure (mmHg)
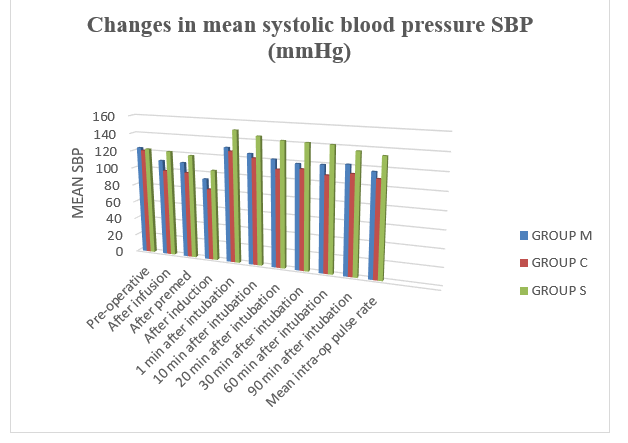
Fig 3 Showing changes in mean Diastolic blood pressure (mmHg)
Laparoscopic procedures are widely accepted in the clinical practice, now-a-days with various advantages as compared to open procedures. But, laparoscopy procedures are also associated some disadvantages like greater alteration in hemodynamic parameters intraoperatively, primarily due to extra peritoneal or intraperitoneal CO2 insufflation to achieve pneumoperitoneum and secondarily due to position given in some laparoscopic procedures, So, the drugs given during laparoscopic procedures should be such that it should not compromise the advantage of laparoscopy and at the same time minimizes hemodynamic changes due to CO2 insufflation.
Clonidine is an imidazoline derivative that acts as an alpha 2 agonist. It has analgesic properties and induces preoperative anxiolysis and sedation. clonidine not only has potential to attenuate sympathoadreanl response to laryngoscopy and tracheal intubation but it also improves the intraoperative hemodynamic stability along with reduction in the intraoperative requirement of anaesthetic agents and postoperative pain. [2] Clonidine inhibits release of catecholamine’s and vasopressin and thus modulates hemodynamic changes associated with pneumoperitoneum. [38]
Magnesium inhibits catecholamine release from both the adrenal gland and adrenergic nerve terminals . By acting as an antagonist of N-methyl d-aspartate (NMDA) receptors, magnesium (Mg) has the potential to treat and prevent pain. [4–5] Mg suppressed NMDA-induced adverse behavioural reactions and hypersensitivities caused by nerve injuries in animals. Magnesium's role in reducing analgesic requirements during the postoperative period was demonstrated in a clinical study.[6] Magnesium administration, according to Koinig et al [15], resulted in a significant reduction in fentanyl consumption during the perioperative period. Intravenous magnesium sulphate reduces catecholamine release during tracheal intubation. It also has direct action on blood vessels causing vasodilation and at higher doses, it reduces vasopressin-mediated vasoconstriction.
Various studies have been carried out to find out efficacy of clonidine and magnesium sulphate as adjunct to general anaesthesia in providing intraoperative hemodynamic stability and decreased anaesthetic consumption like Kodaka M. et al 13, Imai Y et al 16, Fehr S.B. et al 8, Telci L. et al 9, Altan A. et al 10, Ray M. et al 30 and the results of these studies are quite favourable.
In this study group, clonidine was used in doses of 3 mcg/kg of body weight this dose was used considering its favourable results as per study of Altan and Turgut et al 10 in 2005 they used clonidine 3 mcg/kg in 20 ml saline intravenously over a period of 15 minutes before induction and 2mcg/kg /hour by continuous infusion intraoperatively, in their study, they found significant rates of bradycardia and hypotension. 4.5 mcg/kg clonidine significantly reduced mean arterial pressure prior to anaesthesia induction, according to Aho M. et al 40. As a result, they advised 3 mcg/kg of clonidine for perioperative hemodynamic stability. Based on these findings, we gave clonidine 3 mcg/kg intravenously 15 minutes before induction and did not use continuous infusion intraoperatively.
Seyhan T.O. et al 11 2006 used 40mg/kg magnesium sulphate as bolus before induction followed by infusion at 10mg/kg/hr or 20mg/kg/hr for next 4 hours they observed that increasing magnesium doses did not offer advantages intraoperatively, but rather induced hemodynamic consequences, Elsharnouby N.M. et al 41 used magnesium sulphate 40mg/kg intravenously over a period of 15 minutes before induction and 15mg/kg/hr by continuous infusion intraoperatively they noticed more episodes of severe hypotension using this dose of magnesium sulphate taking into consideration the results of the above mentioned studies in our study we only used a single bolus dose of magnesium sulphate 40mg/kg before induction and we did not used any magnesium infusion intraoperatively the dose selected by resulted in a steady and smooth reduction of blood pressure and heart rate.
After study drug infusion patients were premedicated with inj. glycopyrrolate 4μg/kg IV as routine anticholinergic premedication to protect from vagal reflexes and as antisialogue and inj. fentanyl citrate 2mcg/kg of body weight IV 10 min. before induction. Propofol was used as inducing agent in all three groups, time for BIS to decrease more than 60 noted as induction period.[10] The mean induction period was significantly less in Group M and C, The overall mean requirement of Propofol dose for induction was significantly less in magnesium sulphate and clonidine group (p<0.001) compare to control group. Similar findings were observed by Richards M.J. et al 7, Goyagi T. et al 17 , Marinangeli F. et al 19, Fehr S.B.et al 8, Altan A. et al 2005 10, Paris A. et al 29, and Ray M. et al. 30, The reduced induction dose of propofol in clonidine pretreated group can be considered as an additive hypnotic effect of clonidine.
The overall mean requirement of Propofol infusion for maintenance was significantly less (p<0.001) in magnesium sulphate and clonidine group compare to control group Our findings were similar to, Fehr S.B. et al 8, Telci L. et al 9, Morris J. et al 24, Altan A.et al 10, Seyhan T.O.et al 11, Ryu J.H.et al 27, Ray M. et al30.
In our study, propofol requirements were significantly lower in both Group C and Group M compared to Group S. Kulka P.J. et al 42 reported that studies with rat model showed, at clinical concentration clonidine partially inhibits voltage-gated Na+ and K+ channels and suppresses the generation of action potentials in tonic firing spinal dorsal horn neurons. This may contribute to the reduction of propofol and fentanyl requirements. [30]
James M.F. et al 3 stated that MgSO4 has been reported to produce general anaesthesia and enhance the activity of local anaesthetic agents. Depressant effects of MgSO4 on the central nervous system (CNS) of animals have been reported too.[4] Woolf C.J. et al 5 stated that magnesium antagonized NMDA receptors in the CNS. Another mechanism could be that magnesium decreases peripheral nociceptor sensitisation or the stress response to surgery by reducing catecholamine release via sympathetic stimulation. However, these mechanisms do not explain the decrease in propofol requirements, so more research on the interaction of magnesium and propofol as sole agents is needed. By acting as an antagonist of NMDA receptors, magnesium has the potential to prevent pain.[5] Koinig H. et al 15 first evaluated the effect of magnesium on perioperative analgesic requirement in patients with identical level of surgical stimulation. Shulz-Stubher et al.43 also confirmed this in their study.
Laryngoscopy and intubation is considered to be stress response and increase in pulse rate, systolic blood pressure and diastolic blood pressure is expected during these events. Pre-treatment with magnesium sulphate and clonidine provided better protection against sympathetic stimulation due to laryngoscopy and intubation and leading to blunting of intubation response. Kodaka M. et al 13, Imai Y. et al 16, Altan A. et al 10, Seyhan T.O. et al 11, Ray M. et al 30 and Das M. et al. [44].
After co2 insufflation there was increase in pulse rate in all three groups but it was significantly increased more in control group (Group S) rise in pulse rate was due to activation of sympathoadrenal or humoral response but pulse remained on stable side in group M and group C due to pre-treatment with magnesium sulphate and clonidine which lead to attenuation of the hemodynamic response to pneumoperitoneum. Kalra N.K. et al 31, Das M. et al 44, Singh S. et al.45
Pulse remain stable and on lower side in group M & C throughout intraoperative period whereas it was on higher side in control group there was significant difference among the three groups (p<0.05), suggesting that Clonidine and magnesium lead to hemodynamic stability intraoperatively. Altan A. et al 10, Ray M. et al 30, Kalra N.K. et al 31, Das M. et al 44, Singh S. et al.45
Preoperative premedication with magnesium sulphate and clonidine lead to stable hemodynamic after intubation. [19,10,11,30,45]
Fehr S.B. et al 8 reported that clonidine administration resulted in a lower propofol requirement for certain level of anaesthesia to be achieved as defined by similar BIS values. The fact that no explicit intraoperative awareness occurred and no signs of implicit memory were observed indicates that the anaesthetic state induced by a clonidine and low dose propofol may be similar to the anaesthetic state induced by a larger dose of propofol alone. It is evident that larger trials will be necessary to show conclusively that lower dose of propofol combined with clonidine is as safe as a larger dose of propofol in preventing intraoperative awareness. Lee D.H. et al 46 stated that, recent studies have demonstrated that magnesium administration significantly reduces anaesthetic drug requirements and attenuation of BIS increases, suggesting that magnesium sulphate may have a sedative effect and thus might be beneficial.
Hence, in our study titrating propofol infusion rate with BIS monitoring during balanced anaesthesia decreased propofol use and significantly improved recovery in our study. These findings indicate that the use of BIS may be valuable in guiding the administration of propofol intraoperatively. Gan T.J. et al 14, Fehr S.B. et al 8, Altan A. et al 10, Seyhan T.O. et al11, and Ray M. et al.3
Time for BIS to rose up to 80 after stoppage of propofol infusion was recorded as recovery time in each group as per Altan A. et al.[10]The mean recovery time was found to be 9.23 ± 2.45 min in group M, 6.86 ± 1.56 min in group C and 7.36 ± 2.05 min in group S. It was significantly prolonged in magnesium group (p<0.001). Mean recovery time was comparable in group C and group S (p>0.05). Similar findings were observed by Altan A. et al 10, Ray M. et al.30
Extubation time was calculated from stoppage of propofol infusion stopped till the tracheal extubation of patient after ensuring adequate reversal, sustained (>5sec) head lift and a forceful hand grip.We observed that recovery time was faster in clonidine and was prolonged in magnesium group due to central depressant effect of magnesium sulphate.
Richards M.J. et al 7 found significant delay in recovery in clonidine premedicated patients due to the use of high dose of clonidine (8.5μg/kg) in combination with a benzodiazepine. Guglielminotti J. et al 2 with the 5μg/kg dose of oral clonidine failed to detect any delay in recovery from patients leading to early extubation compare to magnesium and control group. This was also consistent with the data of Kumar A. et al 47 and Ghingone M. et al 48, who have reported a faster recovery in elderly patients undergoing intraocular surgery and premedicated with 5μg/kg clonidine when compare with patients premedicated with diazepam.
Magnesium group was associated with delayed recovery this could be due to central depressant action of magnesium sulphate. Guglielminotti J et al 2, Altan A. et al 10, Seyhan T.O. et al 11, Ray M. et al 30and Kalra N.K. et al.31
When the groups were compared for the parameters of recovery; response to verbal commands and orientation time as per Altan A. et al 10 we found that these parameters were longer with group M (P<0.001) there were no significant difference between other two groups (P>0.05) this delay in recovery in magnesium group may be due to CNS depressant effect of magnesium sulphate. Peck C.H. et al 49 in their study attempted anaesthesia by magnesium sulphate infusion in three patients of herniorrhaphy and reported a narcotic state. However, Aldrete J.A. 50et al suggested that this was actually a sleep like state caused by cerebral hypoxia from progressive respiratory and cardiac depression. When ventilation was maintained even very high level of serum Mg produced no central nervous system depression. Kalra N.K. et al 31 stated that magnesium sulphate potentiates neuromuscular blockade induced by non-depolarizing neuromuscular agents and this possible was the cause of prolongation in recovery. Patient in clonidine group had early recovery except for delayed orientation time this could be due to known sedative action of clonidine. Telci L. et al 9, Altan A. et al 10, Seyhan T.O. et al 11, Ray M. et al 30, and Karla N.K. et al.31
The mean pain score in the immediate post-op period was found to be lower in group M and group C compared to group S which was statistically significant (p<0.001). Noxious stimulation leads to the release of neurotransmitters, which bind to various subclasses of excitatory amino acid receptors, including NMDA receptors. Activation of these receptors leads to calcium entry into the cell and initiates a series of central sensitization such as wind-up and long term potentiating in the spinal cord in the response of cells to prolonged stimuli.[52] Woolf C.J. et al 5 stated that NMDA receptor signaling may be important in determining the duration of acute pain. Magnesium blocks calcium influx and noncompetitively antagonizes NMDA receptor channels. [53] Non-competitive NMDA receptor antagonists can have an effect on pain when used alone. [54] As magnesium sulphate has NMDA receptor antagonist action this may lead to postoperative pain relief in magnesium pre-treated group. Clonidine induces dose-dependent spinal cord antinociception, mainly through stimulation of α2-adrenoceptors in the dorsal horn, mimicking the activation of descending inhibitory pathways.[55]Koining H. et al 15, Seyhan T.O. et al 11, Ryu J.H. et al 27, Tramer M.R. et al.6
Wadhwa et al [56] suggested that magnesium sulphate infusion reduces the shivering threshold in humans, and IV magnesium sulphate has been reported previously to suppress post- anaesthetic shivering.[57] Shivering causes discomfort and aggravates postoperative pain [58 ] and the prevention of shivering may attenuate postoperative pain and enhance patient’s satisfaction.
PONV was a common side effect observed in all the groups in the recovery room. Mikawa et al 59 and Handa et al 60 have reported a reduced incidence of PONV after premedication with clonidine in children undergoing strabismus surgery and Oddby M.E. et al 61also reported antiemetic effect of clonidine after breast surgery in adults. Singh S. et al 45 in their study reported decreased Incidence of nausea and vomiting in clonidine group compare to control group (28% Vs 52%).
A general reduction in sympathetic outflow caused by clonidine [62], could also attributed to the reduction of PONV, since a high sympathetic tone and catecholamine release may trigger nausea and vomiting.[63,64] Further studies are necessary to gain better understanding regarding which of the afore-mentioned mechanisms that is most important with regard to the antiemetic effects of clonidine.
Delayed recovery associated with magnesium due to its CNS depressant action also the potent sedative activity of clonidine is associated with greater degree of sedation and drowsiness in post-operative period. Telci L. et al 9, Altan A. et al 10, Seyhan T.O. et al 11, Ray M. et al 30, and Karla N.K. et al.31
It was thus observed that pre-treatment with magnesium sulphate and clonidine lead to better obtundation of pressor response and also provided optimum hemodynamic stability throughout the laparoscopic surgical procedure and also reduced propofol consumption for induction as well as for maintenance. Both clonidine and magnesium sulphate caused bradycardia and hypotension and magnesium sulphate caused delay in recovery. Therefore, both clonidine and magnesium sulphate need careful management, to be used as adjuvant agents to general anaesthesia.
So to conclude Clonidine and magnesium sulphate both reduced propofol consumption and the haemodynamic response to tracheal intubation. Clonidine was linked to bradycardia and hypotension, while magnesium sulphate slowed recovery.
CONFLICT OF INTEREST: Nil declared by the authors
FUNDING: No funding was received for this paper
Bovill, J. G. "Total intravenous anesthesia--a pharmacokinetic approach." Middle East Journal of Anaesthesiology 13.1 (1995): 37-60..
Guglielminotti, J., et al. "Effects of premedication on dose requirements for propofol: comparison of clonidine and hydroxyzine." British journal of anaesthesia 80.6 (1998): 733-736. https://doi.org/10.1093/bja/80.6.733 .
James, Michael FM. "Clinical use of magnesium infusions in anesthesia." Anesthesia & Analgesia 74.1 (1992): 129-136.
Feria, Manuel, et al. "Magnesium sulphate injected subcutaneously suppresses autotomy in peripherally deafferented rats." Pain 53.3 (1993): 287-293. https://doi.org/10.1016/0304-3959(93)90225-E .
Woolf, Clifford J., and Stephen WN Thompson. "The induction and maintenance of central sensitization is dependent onN-methyl-d-aspartic acid receptor activation; implications for the treatment of post-injury pain hypersensitivity states." Pain 44.3 (1991): 293-299. DOI: 10.1016/0304-3959(91)90100-C.
Tramer, Martin R., et al. "Role of magnesium sulfate in postoperative analgesia." Anesthesiology 84.2 (1996): 340-347. https://doi.org/10.1097/00000542-199602000-00011 .
Richards, M. J., et al. "Total iv anaesthesia with propofol and alfentanil: dose requirements for propofol and the effect of premedication with clonidine." BJA: British Journal of Anaesthesia 65.2 (1990): 157-163. https://doi.org/10.1093/bja/65.2.157 .
Fehr, S. B., et al. "Clonidine decreases propofol requirements during anaesthesia: effect on bispectral index." British journal of anaesthesia 86.5 (2001): 627-632.https://doi.org/10.1093/bja/86.5.627 .
Telci, Lütfü, et al. "Evaluation of effects of magnesium sulphate in reducing intraoperative anaesthetic requirements." British journal of anaesthesia 89.4 (2002): 594-598. https://doi.org/10.1093/bja/aef238 .
Altan, A., et al. "Effects of magnesium sulphate and clonidine on propofol consumption, haemodynamics and postoperative recovery." British journal of anaesthesia 94.4 (2005): 438-441. https://doi.org/10.1093/bja/aei070.
Seyhan, T. O., et al. "Effects of three different dose regimens of magnesium on propofol requirements, haemodynamic variables and postoperative pain relief in gynaecological surgery." British journal of anaesthesia 96.2 (2006): 247-252. https://doi.org/10.1093/bja/aei291 .
Nora, Fernando Squeff. "Total intravenous anesthesia as a target-controlled infusion: an evolutive analysis." Revista Brasileira de Anestesiologia 58 (2008): 179-192. https://doi.org/10.1590/S0034-70942008000200011 .
Kodaka, M., et al. "The effects of premedication on induction doses of propofol and hemodynamic responses during induction." Masui. The Japanese Journal of Anesthesiology 46.10 (1997): 1347-1353..
Gan, Tong J., et al. "Bispectral index monitoring allows faster emergence and improved recovery from propofol, alfentanil, and nitrous oxide anesthesia. BIS Utility Study Group." Anesthesiology 87.4 (1997): 808-815. https://doi.org/10.1097/00000542-199710000-00014 .
Koinig, Herbert, et al. "Magnesium sulfate reduces intra-and postoperative analgesic requirements." Anesthesia & Analgesia 87.1 (1998): 206-210. DOI: 10.1213/00000539-199807000-00042 .
Imai, Yuichirou, et al. "The effects of preanesthetic oral clonidine on total requirement of propofol for general anesthesia." Journal of clinical Anesthesia 10.8 (1998): 660-665.https://doi.org/10.1016/S0952-8180(98)00111-1 .
Goyagi, Toru, Makoto Tanaka, and Toshiaki Nishikawa. "Oral clonidine premedication reduces propofol requirement for laryngeal mask airway insertion." Canadian journal of anaesthesia 47 (2000): 627-630.
Friedberg, Barry L., and Jeffrey C. Sigl. "Clonidine premedication decreases propofol consumption during bispectral index (BIS) monitored propofol-ketamine technique for office-based surgery." Dermatologic surgery 26.9 (2000): 848-852. DOI: 10.1046/j.1524-4725.2000.00074.x.
Marinangeli, F., et al. "Haemodynamic effects of intravenous clonidine on propofol or thiopental induction." Acta anaesthesiologica scandinavica 44.2 (2000): 150-156. https://doi.org/10.1034/j.1399-6576.2000.440204.x .
Matot, Idit, et al. "The effect of clonidine premedication on hemodynamic responses to microlaryngoscopy and rigid bronchoscopy." Anesthesia & Analgesia 91.4 (2000): 828-833. DOI: 10.1097/00000539-200010000-00011.
Higuchi, Hideyuki, et al. "The interaction between propofol and clonidine for loss of consciousness." Anesthesia & Analgesia 94.4 (2002): 886-891. DOI: 10.1097/00000539-200204000-00021 .
Higuchi, H., et al. "Oral clonidine premedication reduces the EC50 of propofol concentration for laryngeal mask airway insertion in male patients." Acta anaesthesiologica scandinavica 46.4 (2002): 372-377. https://doi.org/10.1034/j.1399-6576.2002.460407.x .
Choi, Jae Chan, et al. "Intravenous magnesium sulfate administration reduces propofol infusion requirements during maintenance of propofol-N2O anesthesia: part I: comparing propofol requirements according to hemodynamic responses: part II: comparing bispectral index in control and magnesium groups." Anesthesiology 97.5 (2002): 1137-1141. https://doi.org/10.1097/00000542-200211000-00017 .
Morris, J., et al. "Effect of clonidine pre-medication on propofol requirements during lower extremity vascular surgery: a randomized controlled trial." British journal of anaesthesia 95.2 (2005): 183-188. https://doi.org/10.1093/bja/aei172 .
Cizmeci, Pelin, and Zerrin Ozkose. "Magnesium sulphate as an adjuvant to total intravenous anesthesia in septorhinoplasty: a randomized controlled study." Aesthetic plastic surgery 31 (2007): 167-173..
Khafagy, Hanan F., Emad S. Osman, and Amr F. Naguib. "Effects of different dose regimens of magnesium on pharmacodynamics and anesthetic requirements of balanced general anesthesia." J Egypt Soc Parasitol 37.2 (2007): 469-82.
Ryu, J-H., et al. "Effects of magnesium sulphate on intraoperative anaesthetic requirements and postoperative analgesia in gynaecology patients receiving total intravenous anaesthesia." British journal of anaesthesia 100.3 (2008): 397-403. https://doi.org/10.1093/bja/aem407 .
Ghosh, Indranil, et al. "Both clonidine and metoprolol modify anesthetic depth indicators and reduce intraoperative propofol requirement." Journal of anesthesia 22 (2008): 131-134..
Paris, Andrea, et al. "Effects of clonidine and midazolam premedication on bispectral index and recovery after elective surgery." European Journal of Anaesthesiology| EJA 26.7 (2009): 603-610.
Ray, Manjushree, et al. "Effect of clonidine and magnesium sulphate on anaesthetic consumption, haemodynamics and postoperative recovery: A comparative study." Indian Journal of anaesthesia 54.2 (2010): 137-141. DOI: 10.4103/0019-5049.63659.
Kalra, Nand Kishore, et al. "Comparative study of intravenously administered clonidine and magnesium sulfate on hemodynamic responses during laparoscopic cholecystectomy." Journal of Anaesthesiology Clinical Pharmacology 27.3 (2011): 344-348. DOI: 10.4103/0970-9185.83679.
Antihypertensive drugs. In: Pharmacology & Physiology in Anesthetic Practice. Stoelting RK, Hillers SC, editors 4th ed. Philadelphia: Lippincott Williams and Wilkins,2006.p.338-352.
The comprehensive resource for physicians, drug and illness information [Online]. Available from: URL:http://www.rxmed.com/b.main/b2.pharmaceutical/b2.1.monographs/CPS-%20Monographs/CPS-%20(General%20Monographs-%20M)/MAGNESIUM%20SULFATE.html
Non barbiturates intravenous anesthetic drugs. In: Pharmacology & Physiology in Anesthetic Practice. Stoelting RK, Hillers SC, editors 4th ed. Philadelphia: Lippincott Williams and Wilkins,2006.p.155-179.
Reves JG, Glass P, Lubarsky DA, McEvoy MD, Ruiz RM. Intravenous anesthetics. In: Miller’s Anesthesia. Miller RD, Eriksson LI, Fleisher LA,Wiener- Kronish JP, Young W, editors. 7th ed. Philadelphia: Elsevier Churchil Livingstone, 2010.p.719-768.
Opioid agonists and antagonists In: Pharmacology & Physiology in Anesthetic Practice. Stoelting RK, Hillers SC, editors 4th ed. Philadelphia: Lippincott Williams and Wilkins,2006.p.87-126.
Miller RD, Eriksson LI, Fleisher LA, Wiener- Kronish JP, Young W, editors. 7th ed. Philadelphia: Elsevier Churchil Livingstone, 2010.
Joris, J., J. D. Chiche, and M. Lamy. "Clonidine reduces the haemodynamic changes induced by pneumoperitoneum during laparoscopic cholecystectomy." BRITISH JOURNAL OF ANAESTHESIA 74 (1995): A-124..
Flaishon, R., et al. "Recovery of consciousness after thiopental or propofol. Bispectral index and isolated forearm technique." Anesthesiology 86.3 (1997): 613-619. https://doi.org/10.1097/00000542-199703000-00013 .
Aho, M., et al. "Intramuscularly administered dexmedetomidine attenuates hemodynamic and stress hormone responses to gynecologic laparoscopy." Anesthesia & Analgesia 75.6 (1992): 932-939..
Elsharnouby, N. M., and M. M. Elsharnouby. "Magnesium sulphate as a technique of hypotensive anaesthesia." BJA: British Journal of Anaesthesia 96.6 (2006): 727-731. https://doi.org/10.1093/bja/ael085 .
Kulka, P. J., et al. "Does clonidine modify the hypnotic effect of propofol?." Der Anaesthesist 42.9 (1993): 630-637..
Schulz-Stübner, S., et al. "Magnesium as part of balanced general anaesthesia with propofol, remifentanil and mivacurium: a double-blind, randomized prospective study in 50 patients." European journal of anaesthesiology 18.11 (2001): 723-729..
Das, Mrinmoy, Manjushree Ray, and Gauri Mukherjee. "Haemodynamic changes during laparoscopic cholecystectomy: Effect of clonidine premedication." Indian Journal of Anaesthesia 51.3 (2007): 205-210..
45Singh, Shivinder, and Kapil Arora. "Effect of oral clonidine premedication on perioperative haemodynamic response and postoperative analgesic requirement for patients undergoing laparoscopic cholecystectomy." Indian journal of anaesthesia 55.1 (2011): 26-30. DOI: 10.4103/0019-5049.76583.
Lee, D. H., and I. C. Kwon. "Magnesium sulphate has beneficial effects as an adjuvant during general anaesthesia for Caesarean section." British journal of anaesthesia 103.6 (2009): 861-866. https://doi.org/10.1093/bja/aep265 .
Kumar, A., et al. "Oral clonidine premedication for elderly patients undergoing intraocular surgery." Acta anaesthesiologica scandinavica 36.2 (1992): 159-164. https://doi.org/10.1111/j.1399-6576.1992.tb03444.x .
Ghignone, Marco, et al. "Anesthesia for ophthalmic surgery in the elderly: the effects of clonidine on intraocular pressure, perioperative hemodynamics, and anesthetic requirement." Anesthesiology 68.5 (1988): 707-716.
PECK, CHARLES H., and SAMUEL J. MELTZER. "Anesthesia in human beings by intravenous injection of magnesium sulphate." Journal of the American Medical Association 67.16 (1916): 1131-1133..
Altan, A., et al. "Effects of magnesium sulphate and clonidine on propofol consumption, haemodynamics and postoperative recovery." British journal of anaesthesia 94.4 (2005): 438-441..
Aldrete, Antonio J. "Post-anesthetic recovery score." Journal of the American College of Surgeons 205.5 (2007): e3-e4. DOI: 10.1016/j.jamcollsurg.2007.07.034.
Pockett, Susan. "Spinal cord synaptic plasticity and chronic pain." Anesthesia & Analgesia 80.1 (1995): 173-179..
53Fawcett, W. J., E. J. Haxby, and D. A. Male. "Magnesium: physiology and pharmacology." British journal of anaesthesia 83.2 (1999): 302-320. https://doi.org/10.1093/bja/83.2.302 .
Bilir, A. Y. T. E. N., et al. "Epidural magnesium reduces postoperative analgesic requirement." British journal of anaesthesia 98.4 (2007): 519-523. https://doi.org/10.1093/bja/aem029 .
Ossipov, Michael H., Linda J. Suarez, and Theodore C. Spaulding. "Antinociceptive Interactions Between Alphha2-Adrenergic and Opiate Agonists at the Spinal Level in Rodents." Anesthesia & Analgesia 68.3 (1989): 194-200..
Wadhwa, Anupama, et al. "Magnesium sulphate only slightly reduces the shivering threshold in humans." British journal of anaesthesia 94.6 (2005): 756-762. https://doi.org/10.1093/bja/aei105 .
Kizilirmak, Sevda, et al. "Magnesium Sulfate Stops Postanesthetic Shivering a." Annals of the New York Academy of Sciences 813.1 (1997): 799-806. https://doi.org/10.1111/j.1749-6632.1997.tb51784.x .
Alfonsi, Pascal. "Postanaesthetic shivering: epidemiology, pathophysiology, and approaches to prevention and management." Drugs 61 (2001): 2193-2205..
Mikawa, Katsuya, et al. "Oral clonidine premedication reduces vomiting in children after strabismus surgery." Canadian journal of anaesthesia 42 (1995): 977-981..
Handa, Fumi, and Yoshitaka Fujii. "Retracted: The efficacy of oral clonidine premedication in the prevention of postoperative vomiting in children following strabismus surgery." Pediatric Anesthesia 11.1 (2001): 71-74. https://doi.org/10.1046/j.1460-9592.2001.00615.x .
Alizadeh, Reza, et al. "Oral clonidine premedication reduces nausea and vomiting in children after appendectomy." Iranian journal of pediatrics 22.3 (2012): 399..
Maze, Mervyn, and William Tranquilli. "Alpha-2 adrenoceptor agonists: defining the role in clinical anesthesia." Anesthesiology 74.3 (1991): 581-605..
Watcha, Mehernoor F., and Paul F. White. "Postoperative nausea and vomiting. Its etiology, treatment, and prevention." Anesthesiology 77.1 (1992): 162-184. https://doi.org/10.1097/00000542-199207000-00023 .
