
+91 6002993949
submission@iarconsortium.org
Open Access
ISSN (Print) : 2709-1872
ISSN (Online) : 2709-1880
This study focused its objective on knowing the extent of complications that exist and generated by the type of anaesthesia on the patient. A study was conducted of 800 patients collected from different Hospitals Baghdad, Iraq. Complications were found in 120 patients. All statistical analyzes were performed for patients of age, gender and type of anesthesia used during in addition to that, the type of complications found in patients was identified and by relying on the statistical analysis program SPSS Soft 20 and MSEXCEL, the data and demographic characteristics of the patients were analyzed.
Anaesthesia complications are adverse events (including death) that are directly or indirectly related to general or RA. The concept of complications from Anaesthesia involves a loss of the ability to control Anaesthesia, which creates an immediate or potential threat to the patient's life [1-3].
One category of Anaesthesia quality is the degree of safety, which requires a determination of the risks of Anaesthesia. A rough estimate of the risks associated with Anaesthesia can be considered. Currently, the Anaesthesia -related mortality rate is 0.4 per 100,000 (1 in 250,000 anesthetics). This applies to patients without serious systemic disease [4-6].
Complications of Anaesthesia include apnea and it is more common in patients with general intravenous Anaesthesia without endotracheal intubation, especially those using thiopentone, propofol, or ketamine in outpatient minor surgery, ophthalmic surgery, induced abortion and various endoscopy; Clinical manifestations No thoracic and abdominal breathing in addition to upper airway obstruction: It appears in endotracheal intubation failure, severe obesity, intravenous Anaesthesia without endotracheal intubation, aspiration of gastric contents and laryngospasm. Patients often show "three concave signs" when breathing spontaneously and prevention should be first. If this occurs, it should be treated immediately: placement of the oral airway, nasopharynx or immediate artificial respiration and atelectasis of the lung is more common in patients after thoracic and upper abdominal surgery as it is mainly caused by ineffective sputum production and bronchial obstruction due to secretions after the operation, It can also be associated with atelectasis caused by unilateral bronchial intubation and inhaled anaesthesia. Prevention: Smoking is prohibited for 2 to 3 weeks before surgery, bronchial intubation is avoided, postoperative analgesia is effective and patients are encouraged to excrete phlegm and breathe deeply [7-10].
Anaesthesia refers to the inhibition of the central nervous system by inhalation or intravenous administration of anesthetic so that the patient enters a state of reversible functional inhibition with loss of consciousness, muscle relaxation, absence of pain and nausea and vomiting after surgery [11-14].
Anaesthesia can be broadly divided into general Anaesthesia and local Anaesthesia. The method of Anaesthesia is generally determined by the anesthesiologist depending on the surgical content of the patient and the time of surgery.
The decision should be made after thorough consideration of time, surgical site, preoperative examination and age, etc., but if requested by the patient, it can be discussed:
General Anaesthesia
Local Anaesthesia (spinal subarachnoid Anaesthesia, epidural Anaesthesia, conduction Anaesthesia (nerve block Anaesthesia)
Spinal, subarachnoid and epidural Anaesthesia is injected from the back or waist while the patient is conscious to relieve pain. Anaesthesia is an injection around the nerves innervating the surgical site to relieve pain
Combined use of general Anaesthesia and local Anaesthesia
The combined application of general and local Anaesthesia can reduce the physical burden of Anaesthesia on patients and increase the safety of surgery [15-20].
Patient and Method
Patient Sample: About 120 patients who underwent surgical procedures were collected and the effects of anaesthesia on the complications and complications were evaluated. Information and demographic data for patients were collected from different Hospitals Baghdad, Iraq.
Study Design
The aim of the study was to determine the extent of complications that occurred after anaesthesia.
Anesthesia is a good way to use prescription drugs to relieve a patient's pain during surgery. Doctors usually use general anesthesia in surgical procedures, where the patient does not feel pain stimuli.
The study was split into 60% men and 40% women and there are many potential side effects associated with the use of anesthesia in surgeries and procedures. These issues vary greatly from small issues to major and life-threatening problems. Fortunately, severe problems after receiving anesthesia are uncommon and the average patient will not have minor problems in the hours and days following their procedure.
The type of side effects an individual can experience with anesthesia will vary greatly based on the type of anesthesia they receive, the length of time they have been under anesthesia and the nature of the problem that made the anesthesia necessary.
Study Period
The study period related to the collection of patient characteristics and information from 6-6-2020 to 23-9-2021.
Aim of Study
The research aims to determine the frequency of complications that occur after anesthesia, in addition to knowing the instructions related to anesthesia (Figure 1).
After understanding general anesthesia, the risks and complications of general anesthesia are often closely related to these three steps. Postoperative nausea and vomiting: Many patients experience nausea and vomiting after surgery. This situation is mainly related to the following three aspects which are the effect of anesthetic drugs, many drugs can cause vomiting after surgery (Table 1).
The effect of the patient's special circumstances: Delayed gastric emptying, such as not fasting before surgery, shock pain and anxiety, patients with gastro-intestinal decompression tube placement have a higher chance of vomiting after surgery (Table 2, Figure 1).
For patients with complete intestinal obstruction and elevated intestinal obstruction, gastroesophageal reflux and airway aspiration are likely. The risk of bronchospasm, hypoxia, dyspnea and pneumonia is high. A notable complication is high blood pressure. Various factors during surgery can cause unstable blood pressure.
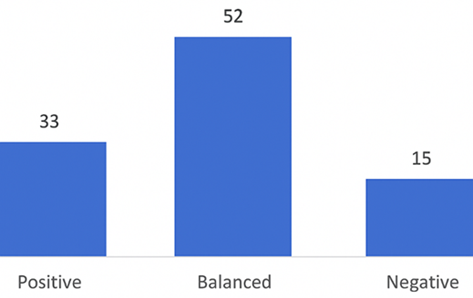
Figure 1: Frequency of Age
Table 1: Distribution of Patient According to Gender
| Age * gender Cross tabulation | ||||
| Count | ||||
| Gender | Total | |||
| f | m | |||
| Age | 20-24 | 4 | 3 | 7 |
| 25-29 | 11 | 12 | 23 | |
| 30-34 | 13 | 11 | 24 | |
| 35-39 | 13 | 16 | 29 | |
| 40-44 | 9 | 10 | 19 | |
| 45-50 | 9 | 9 | 18 | |
| Total | 59 | 61 | 120 | |
Table 2: Distribution of Patient According to Type of Anaesthesia
| Gender * anaesthesia * age Crosstabulation | ||||||
| Count | ||||||
| Age | Anaesthesia | Total | ||||
| General anesthesia | Local anaesthesia | Regional anesthesi | ||||
| 20-24 | Gender | f | 2 | 1 | 1 | 4 |
| m | 1 | 0 | 2 | 3 | ||
| Total | 3 | 1 | 3 | 7 | ||
| 25-29 | Gender | f | 5 | 3 | 3 | 11 |
| m | 10 | 0 | 2 | 12 | ||
| Total | 15 | 3 | 5 | 23 | ||
| 30-34 | Gender | f | 5 | 5 | 3 | 13 |
| m | 6 | 2 | 3 | 11 | ||
| Total | 11 | 7 | 6 | 24 | ||
| 35-39 | GENDER | f | 5 | 6 | 2 | 13 |
| m | 11 | 2 | 3 | 16 | ||
| Total | 16 | 8 | 5 | 29 | ||
| 40-44 | Gender | f | 2 | 5 | 2 | 9 |
| m | 8 | 1 | 1 | 10 | ||
| Total | 10 | 6 | 3 | 19 | ||
| 45-50 | Gender | f | 5 | 1 | 3 | 9 |
| m | 3 | 0 | 6 | 9 | ||
| Total | 8 | 1 | 9 | 18 | ||
| Total | Gender | f | 24 | 21 | 14 | 59 |
| m | 39 | 5 | 17 | 61 | ||
| Total | 63 | 26 | 31 | 120 | ||
Table 3: Frequency of Complication According to Anaesthesia
| Anaesthesia | ||||||||
| f | % | vp | cp | |||||
| Valid | 1 | 0.8 | 0.8 | 0.8 | ||||
| Acute bronchitis | 5 | 4.1 | 4.1 | 5.0 | ||||
| arterial hypertension | 5 | 4.1 | 4.1 | 9.1 | ||||
| bleeding | 4 | 3.3 | 3.3 | 12.4 | ||||
| headache | 17 | 14.0 | 14.0 | 26.4 | ||||
| Hypertension | 10 | 8.3 | 8.3 | 34.7 | ||||
| itching | 5 | 4.1 | 4.1 | 38.8 | ||||
| apnea | 1 | .8 | 0.8 | 39.7 | ||||
| Hipoxia | 8 | 6.6 | 6.6 | 46.3 | ||||
| Nausea | 5 | 4.1 | 4.1 | 50.4 | ||||
| Nausea + vomiting | 31 | 25.6 | 25.6 | 76.0 | ||||
| Nerve defect. | 4 | 3.3 | 3.3 | 79.3 | ||||
| Rapid inflammation in the heart rhythm | 2 | 1.7 | 1.7 | 81.0 | ||||
| Reintervention | 6 | 5.0 | 5.0 | 86.0 | ||||
| Pain and Burning | 5 | 4.1 | 4.1 | 90.1 | ||||
| shivering | 7 | 5.8 | 5.8 | 95.9 | ||||
| vomiting | 5 | 4.1 | 4.1 | 100.0 | ||||
| Total | 121 | 100.0 | 100.0 | |||||
Excessive blood loss during surgery without timely regeneration, surgical manipulation of internal organs, compression of large blood vessels, heart and parasympathetic reflexes caused by surgical manipulation leads to hypotension (Table 3).
We divide complications into local and systemic. Local complications appear at the site of needle injection or application of anesthesia, while systemic complications involve the whole organism. Local complications include needle fracture, headache and Nerve defect (Table 4).
Pain and Burning
Local anesthesia is the main method of pain control, it is impossible to imagine a day in surgical practice without these wonderful drugs that block harmful stimuli that occur during the operation and are interpreted as pain. While other methods of pain control are available.
These problems are almost always short-lived and usually preventable as slow administration of the local anesthetic improves the safety and comfort of the injection and the entire contents of the cartridge (1.8 or 2.2 mL) should be inserted within about 1 minute.
Table 4: Classification According To Type of Anaesthesia
VAR00003 | ||||
Count | General anesthesia | Local anesthesia | Regional anesthesi | Total |
Acute bronchitis | 5 | 0 | 0 | 5 |
arterial hypertension | 5 | 0 | 0 | 5 |
bleeding | 0 | 4 | 0 | 4 |
headache | 0 | 11 | 6 | 17 |
Hypertension | 2 | 0 | 8 | 10 |
itching | 1 | 0 | 4 | 5 |
apnea | 1 | 0 | 0 | 1 |
Hipoxia | 8 | 0 | 0 | 8 |
Nausea | 0 | 0 | 5 | 5 |
Nausea + vomiting | 31 | 0 | 0 | 31 |
Nerve defect. | 0 | 4 | 0 | 4 |
Rapid inflammation in the heart rhythm | 0 | 0 | 2 | 2 |
REINTERVENTION | 0 | 0 | 6 | 6 |
PAIN AND BURNING | 0 | 5 | 0 | 5 |
shivering | 7 | 0 | 0 | 7 |
vomiting | 3 | 2 | 0 | 5 |
Total | 63 | 26 | 31 | 120 |
Hypoxemia was the afrom most common postoperative complication. Although confirmation of the diagnosis is gas measurement (PaO2 less than 60 mmHg or less than expected for age: 102 minus ages multiplied by 0.33, in a patient ventilating air); for our study, it was considered as a blood oxygen saturation of less than 90% recorded by pulse oximetry. (4) All patients in the PACU in our Hospitals routinely monitor oxygen saturation and administer supplemental oxygen with a free flow mask.
The incidence of complications found in this study was 20%, a number comparable to most studies, which deal with a frequency of 6-7-30%. However, we should note that this result is close to the upper limit. In any case, it should be considered that studies use different criteria to identify complications.
Recommendation
The anesthesiologist must choose the dose carefully and stay during the operation to monitor the effect of the anesthesia on the patient and adjust its quantity when needed to avoid any complications
Monitor any side affects you experience for the first two days after discharge from the Hospitals and tell your doctor about them
Take a break and stay at home for at least two days after the procedure
Beecher, H.K and D.P. Todd. “A study of the deaths associated with anesthesia and surgery: Based on a study of 599,548 anesthesias in ten institutions 1948–1952, inclusive.” Annals of Surgery, vol. 140, 1954, pp. 2–34.
Li, G. et al. “Epidemiology of anesthesia-related mortality in the United States, 1999–2005.” Anesthesiology, vol. 110, 2009, pp. 759–65. https://doi.org/10.1097/ALN.0b013e31819b5bdc.
Cheney, F.W. “The American Society of Anesthesiologists Closed Claims Project: The beginning.” Anesthesiology, vol. 113, 2010, pp. 957–60. https://doi.org/10.1097/ALN.0b013e3181ef6786.
Cooper, J.B. et al. “Preventable anesthesia mishaps: A study of human factors.” Anesthesiology, vol. 49, 1978, pp. 399–406.
Bates, C.P and M. Fletcher. “Untitled.” Canadian Anaesthetists' Society Journal, vol. 30, 1983, p. 109.
Claeys, R.W and G.S. Decamp. U.S. Patent No. 4,853,521. U.S. Patent and Trademark Office, 1989.
O’Shea, E. “Factors contributing to medication errors: A literature review.” Journal of Clinical Nursing, vol. 8, 1999, pp. 496–504. https://doi.org/10.1046/j.1365-2702.1999.00284.x.
Craig, J and M.E. Wilson. “A survey of anaesthetic misadventures.” Anaesthesia, vol. 36, 1981, pp. 933–36. https://doi.org/10.1111/j.1365-2044.1981.tb08650.x.
Chopra, V., J.G. Bovill and J. Spierdijk. “Accidents, near accidents and complications during anaesthesia: A retrospective analysis of a 10-year period in a teaching hospital.” Anaesthesia, vol. 45, 1990, pp. 3–6. https://doi.org/10.1111/j.1365-2044.1990.tb14492.x.
Bowdle, T.A. “Drug administration errors from the ASA Closed Claims Project.” ASA Newsletter, vol. 67, 2003, pp. 11–13.
Cooper, L. et al. “Influences observed on incidence and reporting of medication errors in anesthesia.” Canadian Journal of Anesthesia, vol. 59, 2012, pp. 562–70. https://doi.org/10.1007/s12630-012-9696-6.
Waters, R.M. et al. “Endotracheal anesthesia and its historical development.” Anesthesia & Analgesia, vol. 12, 1933, pp. 196–203. https://doi.org/10.1213/00000539-193301000-00039.
Burkle, C.M. et al. “A historical perspective on use of the laryngoscope as a tool in anesthesiology.” Anesthesiology, vol. 100, 2004, pp. 1003–6. https://doi.org/10.1097/00000542-200404000-00034.
Mallampati, S.R. et al. “A clinical sign to predict difficult tracheal intubation: A prospective study.” Canadian Anaesthetists' Society Journal, vol. 32, 1985, pp. 429–34. https://doi.org/10.1007/BF03011357.
Apfelbaum, J.L. et al. “Practice guidelines for management of the difficult airway: An updated report by the American Society of Anesthesiologists Task Force on Management of the Difficult Airway.” Anesthesiology, vol. 118, 2013, pp. 251–70. https://doi.org/10.1097/ALN.0b013e31827773b2.
Punjabi, N.M. “The epidemiology of adult obstructive sleep apnea.” Proceedings of the American Thoracic Society, vol. 5, 2008, pp. 136–43. https://doi.org/10.1513/pats.200709-155MG.
Young, T. et al. “The occurrence of sleep-disordered breathing among middle-aged adults.” The New England Journal of Medicine, vol. 328, 1993, pp. 1230–35. https://doi.org/10.1056/NEJM199304293281704.
Biro, P. et al. “Anesthetic management of a patient with obstructive sleep apnea syndrome and difficult airway access.” Journal of Clinical Anesthesia, vol. 7, 1995, pp. 417–21. https://doi.org/10.1016/0952-8180(95)00036-H.
Chung, F. et al. “Validation of the Berlin questionnaire and American Society of Anesthesiologists checklist as screening tools for obstructive sleep apnea in surgical patients.” Anesthesiology, vol. 108, 2008, pp. 822–30. https://doi.org/10.1097/ALN.0b013e31816d91b5.
Hofer, R.E. et al. “Obesity as a risk factor for unanticipated admissions after ambulatory surgery.” Mayo Clinic Proceedings, vol. 83, 2008, pp. 908–13. https://doi.org/10.1016/S0025-6196(11)60767-2.
