
+91 6002993949
submission@iarconsortium.org
Open Access
ISSN (Print) : 2709-1872
ISSN (Online) : 2709-1880
Introduction: Rheumatoid arthritis is a chronic immune-inflammatory disease that affects synovial joints with possibility of extra articular manifestations. Prevalence of rheumatoid arthritis is about is 0.5–1 % [1-2] of population worldwide. Indian data suggest the prevalence to be around 0.65% to 0.75% [3]. Results: A total of 75 RA patients satisfying ACR criteria were enrolled in this study, which include 57 females (76%) and 18 males (24%). Male: female ratio was 1:3.2; Average age was 52.76 years. Conclusion: 1. Prevalence of peripheral neuropathy in RA was 35% 2. Male: female ratio of patients with peripheral neuropathy in RA is 1:2.7. 3. Most common pattern of peripheral neuropathy was pure sensory neuropathy (54%) followed by carpel tunnel syndrome (23 %), then Sensorimotor and Pure motor neuropathy 4. Peripheral Neuropathy is correlated to age, duration, Rheumatoid Factor, anti CCP antibody and ESR5.Peripheral Neuropathy is not correlated to gender, DAS 28 score, drugs, extra articular manifestation.
Rheumatoid arthritis is a chronic immune-inflammatory disease that affects synovial joints with possibility of extra articular manifestations. Prevalence of rheumatoid arthritis is about is 0.5–1% [1-2] of population worldwide. Indian data suggest the prevalence to be around 0.65% to 0.75% [3]. The presence of peripheral neuropathy in patients with rheumatoid arthritis is an often overlooked aspect or incorrectly assigned to peripheral arthritis unless the attending physician is aware of complications; however it contributes significantly to the functional limitation in patients. A sufferer from rheumatoid arthritis has enough to contend within attempting to live in rough harmony with their painful, stiff, weak and swollen joints. The addition of peripheral neurological features may make their life even more unbearable and may necessitate admission to hospital and a greater degree of disability and crippling in the future. It may be asymptomatic in the early stages or may present with wide variety of symptoms and signs ranging from subtle numbness in a hand, to quadriparesis and sudden death. Neurologic syndromes may appear suddenly or developed slowly through months, and emerge early or after years of having RA. Peripheral Neuropathy in Rheumatoid Arthritis is a not well studied aspect. There is a paucity of Indian literature on rheumatoid neuropathy.
Peripheral nerve involvement in rheumatoid arthritis can include compressive neuropathy vasculitis drug toxicities [4] and very rarely amyloidosis, resulting in distal sensory or combined sensory motor neuropathy. A few studies also attribute it to autoimmunity [4]. Although underlying pathology is unclear, ischemia secondary to vasculitis with characteristic axonal loss and humoral mechanism are thought to be important factors. The presence of peripheral neuropathy in RA is difficult to recognize as patient often relate neurological symptom to joint pain and it is also difficult to assess the neurological system in the presence of severe joint disease.
Hence this study is undertaken to evaluate the prevalence and pattern of neuropathy in RA and to correlate it with disease parameter and other extra articular involvement.
Aim
To study the prevalence of peripheral neuropathy in RA
To study the pattern of peripheral neuropathy in RA
To correlate the neuropathy with disease parameters and other extra articular manifestations
Study Design
Cross sectional study
Sample Size, Subjects, Centre and Period of Study
Study sample consist of consecutive seventy five rheumatoid arthritis patients with or without clinical evidence of neuropathy satisfying inclusion and exclusion criteria, attending outpatient department or admitted in the Department of Medicine, Government Medical College, Kozhikode, from January 2017 to December 2017.
Inclusion Criteria
Patients diagnosed as per ACR modified criteria 2010
Exclusion Criteria
Those who are not consenting to participate in study
Those with following disorder:
Diabetes Mellitus
Uremia
Chronic alcoholism
HIV positive cases
Pregnancy
Hypothyroidism
Malignancy
Those on any neurotoxic drugs
Those who underwent orthopedic surgery
Other auto immune disorder
Other neurologic disorder
A total of 75 Rheumatoid Arthritis patients are taken for study. All these patients are evaluated thoroughly by clinical history, physical examination, laboratory methods. The recorded parameters include age, gender, and duration of Rheumatoid Arthritis, lab test results, medication, neuropathic symptoms and disease severity. Severity of rheumatoid arthritis is assessed as per the disease activity score of 28 joints. (DAS28 of greater than 5.1 was considered as active disease). Patients are also examined for the presence of extra articular manifestation. Lab test include– ESR, RF, anti CCP antibody etc. All patients will undergo nerve conduction study of median nerve, ulnar nerve, common peroneal nerve and sural nerve. Compound muscle action potential, sensory nerve action potential, distal and proximal latencies and nerve conduction velocities are studied.
Das 28 Scoring
Count the number of swollen joints (out of the 28)
Count the number of tender joints (out of the 28),
Measure the erythrocyte sedimentation rate (ESR) or C reactive protein (CRP)
Ask the patient to make a ‘global assessment of health' (indicated by marking a 10 cm line between very good and very bad)
These results are then fed into a complex mathematical formula to produce the overall disease activity score. The formula for calculating DAS 28 score is:
DAS28 = 0.56*Ö(t28) + 0.28*Ö(sw28) + 0.70*Ln(ESR) + 0.014*VAS
A DAS28 of greater than 5.1 implies active disease, less than 3.2 low disease activity, and less than 2.6 remission.
Data was entered in Microsoft excel and statistical analyzed using SPSS software trial version (20.0).
A total of 75 RA patients satisfying ACR criteria were enrolled in this study, which include 57 females (76%) and 18 males (24%). Male: female ratio was 1:3.2; Average age was 52.76 years.
Table1: Distribution of Sample Based on Age Group
| Age group (years) | Frequency | Percentage (%) |
<30 | 2 | 2.67 |
31-40 | 5 | 6.67 |
41-50 | 24 | 32 |
51-60 | 28 | 37.33 |
>61 | 16 | 21.33 |
Total | 75 | 100 |
Table 2: Distribution of Pattern of Peripheral Neuropathy
Variables | Male | Female | Number of cases | Percentage |
Pure sensory | 2 | 12 | 14 | 54% |
Sensorimotor | 2 | 1 | 3 | 11.5% |
CTS | 2 | 4 | 6 | 23% |
Pure motor | 1 | 2 | 3 | 11.5% |
Total | 7 | 19 | 26 | 100% |
Table 3: Mean Age of Patients With and Without Peripheral Neuropathy
| Peripheral neuropathy | Mean age | Standard deviation |
| Present | 56.88 | 7.19 |
| Absent | 50.53 | 8.53 |
Mean difference- 6.35; p-value–0.002
Table 4: Comparison of Peripheral Neuropathy and Age
Variables | 50 and Below | Above 50 | Total |
PN+ | 6 | 20 | 26 |
PN- | 23 | 26 | 49 |
Total | 29 | 46 | 75 |
Table 5: Correlation of Peripheral Neuropathy and Duration of Ra
Peripheral Neuropathy | Mean Duration (years) | Standard Deviation |
Present | 6.58 | 4.01 |
Absent | 4.28 | 2.61 |
Table 6: Distribution of Symptoms in Peripheral Neuropathy
Symptoms | Frequency | Percentage (%) |
Burning sensation | 5 | 45.46 |
Pins and needle sensation | 4 | 36.36 |
Numbness | 1 | 9.09 |
Tingling sensation | 1 | 9.09 |
Total | 11 | 100 |
Table 7: Comparison of Peripheral Neuropathy and Deep Tendon Reflexes
| Variables | PN+ | PN- |
| DTR- | 10 | 2 |
| DTR+ | 16 | 47 |
p-value-0.0001
Figure 1: Distribution of Sample Based on Sex

Figure 2: Distribution of Pattern of Peripheral Neuropathy
Figure 3: Distribution of Ages in Those with Peripheral Neuropathy
Table 8: Comparison of Paraesthesia and Deep Tendon Reflexes
| Variables | Paresthesia + | Paresthesia - |
| DTR- | 6 | 4 |
| DTR+ | 5 | 11 |
p-value-0.15

Figure 4: Distribution of Males and Females With and Without Peripheral Neuropathy
Figure 5: Frequency of Distribution of Symptoms
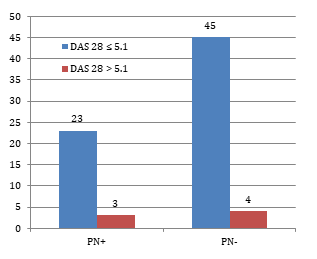
Figure 6: Comparison of Peripheral Neuropathy and DAS 28 Score
Table 9: Comparison of Peripheral Neuropathy and Das 28 Score
Variables | ≤5.1 | >5.1 | Total |
PN+ | 23 | 3 | 26 |
PN- | 45 | 4 | 49 |
p-value-0.63
Table 10: Comparison of Peripheral Neuropathy and Anti Ccp and Age 50 And Below
Age 50 and Below | |||
Variables | Anti Ccp | Total | |
Y | N | ||
Pn(+) | 3 | 3 | 6 |
Pn(-) | 6 | 17 | 23 |
Total | 9 | 20 | 29 |
Odds ratio is 2.83
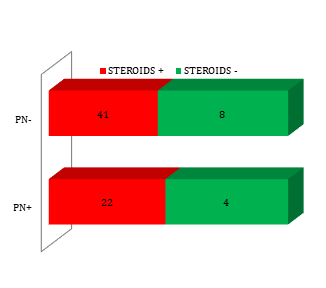
Figure 7: Comparison Of Peripheral Neuropathy and Steroid Intake
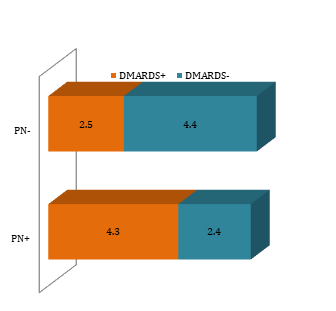
Figure 8: Comparison of Peripheral Neuropathy and DMARD Intake
Table 11: Comparison of Peripheral Neuropathy and Anti Ccp and Age Above 50
| Age - Above 50 | |||
| Variables | Anti Ccp | Total | |
| Y | N | ||
| Pn(+) | 17 | 3 | 20 |
| Pn(-) | 13 | 13 | 26 |
| Total | 30 | 16 | 46 |
Odds Ratio is 5.67
Table 12: Comparison of Peripheral Neuropathy and Esr
Peripheral neuropathy | Mean ESR | Standard deviation |
Present | 60.88 | 24.87 |
Absent | 41.37 | 21.07 |
Mean difference–19.51, p value-0.019
Table 13: Comparison of Peripheral Neuropathy and Ild
| Variables | ILD + | ILD- |
| PN+ | 3 | 23 |
| PN- | 2 | 47 |
p value-0.22
Table 14: Comparison of Peripheral Neuropathy and Scn
Variables | SCN + | SCN - |
PN+ | 1 | 25 |
PN- | 1 | 48 |
p value–0.64
This study was done among 75 patients attending OPD or admitted in the department of medicine, Govt Medical College, Kozhikode, over a period of 1 year, with the diagnosis of RA, with or without clinical evidence of neuropathy, satisfying inclusion and exclusion criteria.
Out of 75 patients 57 were females (76%) and 18 males (24%) with a Male: female ratio of 1:3.2; Females were more than males with RA in this study. It is in accordance with studies done by DeVries et al., Kvien et al. where RA is 3-4 times more frequent in females than males. Most patients were in the age group of 51- 60yrs (37.33%) with a mean age of 52.76 years 5
Peripheral neuropathy in electrophysiological testing was seen in 26 out of 75 patients. So prevalence of peripheral neuropathy in RA was 35%. This was similar to studies conducted by Mi Kyung Sim, et al. [6] where the prevalence of Ra was 30%, Biswas, et al. (39.19%) [7], Aneja et al. (37.87%) [8], Aktekin et al. (36%).
Most common pattern of peripheral neuropathy observed in this study was pure sensory neuropathy (54%) followed by carpel tunnel syndrome (23%), Sensorimotor (11.5%), Pure motor (11.5%). These finding are similar to studies by Albani et al. [10], Agarwal et al. The pattern of neuropathy in various studies is given below.
Among patients with peripheral neuropathy 19 were females and 7 were males. Male: female ratio – 1:2.7. Many studies report a gender bias in favor of males, in contrast to the females predomination in RA patients. The male to female ratio in various reports were found to be in the range from 0.5:1 to 2.6:1.Albani et al. found male gender to be significantly related to peripheral neuropathy but Sivri et al., Bharadwaj et al. and Lang et al. found gender not to be correlated to peripheral neuropathy. However, in our study, we found the male to female ratio of RA patients with neuropathy to be 1:2.7, which was almost similar to that of the study population (1:3.2). However we could not find any association between gender and peripheral neuropathy.
RA patients with peripheral neuropathy are older than those without peripheral neuropathy as maximum number of patients (9 out of 26) with peripheral neuropathy was in age group of age > 61, followed by age group of 51-60. Mean age of patients with peripheral neuropathy was 56.88±7.19 years. PN increases by 11 % with each year of age. In our study we found that patients with age greater than 50 has 2.95 times the risk of developing peripheral neuropathy compared to those with age less than 50. Albani et al. on the basis of multivariate analysis found that age is the most important independent predictor of peripheral neuropathy (P < 0.002) with probability increasing steadily after age 50. Even though age itself is a risk factor for peripheral neuropathy, prevalence of peripheral neuropathy is higher than expected, among patients with RA 18.
Mean duration of RA in those with peripheral neuropathy was 6.58±4.01 years which is significantly associated with the same. Duration of RA is more than 2 years in most of the series, which is consistent with our present study. But Mi Kyung Sim, et al., Biswas et al. and Aneja et al. found no statistically significant difference in the RA duration with peripheral neuropathy in contrast to our study.
Table 15: Comparison of Pattern of Peripheral Neuropathy in Various Studies
| Study and Year | Prevalence of Peripheral Neuropathy | Subclinical Neuropathy | Pure Sensory | Pure Motor | Sensorimotor | CTS |
| Present study | 26/75 | 15 | 14 | 3 | 3 | 6 |
| Biswas, et al.: | 29/74 | 24 | 15 | - | 8 | 3 |
| Agarwal et al. [4] | 62/108 | 46 | 28 | - | 25 | 11 |
| Bharadwaj et al. | 12/140 | 0 | - | - | - | - |
| Nadkar et al. | 10/31 | 5 | - | 4 | 6 | 1 |
| Sivri et al. | 8/33 | 8 | - | - | - | 2 |
| Lanzillo et al. | 26/40 | 26 | - | 26 | - | 5 |
| Lang et al. | 10/23 | 2 | - | - | - | 5 |
Only 42.3% of patients with PN were symptomatic. So majority of peripheral neuropathy (57.7 %) was subclinical. Of all symptoms, burning sensation was the most common complaints (45.46%). Agarwal et al. also describes a similar presentation of peripheral neuropathy [4]. Good et al. found subclinical neuropathy in 85% of RA patients [50], but almost 33% of their patients had diabetes mellitus and long disease duration. None of our patients had diabetes mellitus or other diseases that may predispose to peripheral neuropathy
Deep tendon reflexes were lost in 38.4% of patients with PN. Loss of DTR significantly correlated with the electrophysiological evidence of peripheral neuropathy but not with the presence of paraesthesias. This could be due to confounding effect of the pain in adjacent joints due to arthritis.
Our study showed rheumatoid factor and anti CCP positivity to be significantly related to peripheral neuropathy. It is similar to study conducted by Albani et al. However many studies like those done by Sivri et al. Bharadwaj et al. Nadkar et al. Lang et al. Aneja et al. Woo et al. found no relation between these two attributes. It might be due tertiary referral centre – based population and a small sample size in our study. When we compare the odds ratio of anti CCP antibody for peripheral neuropathy according to age, odd ratio was higher in older age group. So an important finding in our study is that those who are positive for serological marker are at increased risk of peripheral neuropathy and its effect seems to increase with age. In our study univariate analysis has shown a significant relationship between peripheral neuropathy and serological features like age, RF, anti CCP and ESR.
No statistical correlation obtained between peripheral neuropathy and DAS 28 score, drugs, extra articular manifestations. According to the study by Lanzillo et al. corticosteroids has preventive effect on peripheral neuropathy. But no such observations made in our study.
Peripheral nerve involvement seems to be one of the different aspects of rheumatoid arthritis. Electrophysiological testing should be included in the routine evaluation of rheumatoid arthritis as subclinical cases predominate.
Prevalence of peripheral neuropathy in RA was 35%
Male: female ratio of patients with peripheral neuropathy in RA is 1:2.7
Most common pattern of peripheral neuropathy was pure sensory neuropathy (54%) followed by carpel tunnel syndrome (23%), then Sensorimotor and Pure motor neuropathy
Peripheral Neuropathy is correlated to age, duration, Rheumatoid Factor, anti CCP antibody and ESR
Peripheral Neuropathy is not correlated to gender, DAS 28 score, drugs, extra articular manifestation
Age greater than 50 has 2.95 times the risk of developing peripheral neuropathy compared to those with age less than 50
Those who are positive for serological marker are at increased risk of peripheral neuropathy and its effect seems to increase with age
Majority of peripheral neuropathy was subclinical (57.7 %)
Subclinical neuropathy is rather high and more frequent than the other extra articular manifestations
McInnes I.B. and Schett G. "The pathogenesis of rheumatoid arthritis." New England Journal of Medicine, vol. 365, no. 23, 2011, pp. 2205–2219.
Turesson C. et al. "Extra-articular rheumatoid arthritis: prevalence and mortality." Rheumatology (Oxford), vol. 38, no. 7, 1999, pp. 668–674.
Malaviya A.N. et al. "Prevalence of rheumatoid arthritis in the adult Indian population." Rheumatology International, vol. 13, no. 4, 1993, pp. 131–134.
Agarwal V. et al. "A clinical, electrophysiological, and pathological study of neuropathy in rheumatoid arthritis." Clinical Rheumatology, vol. 27, no. 7, 2008, pp. 841–844.
Davies L. et al. "Vasculitis confined to peripheral nerves." Brain, vol. 119, 1996, pp. 1441–1448.
Sim M.K. and Kim D.Y. "Assessment of peripheral neuropathy in patients with rheumatoid arthritis who complain of neurologic symptoms." Annals of Rehabilitation Medicine, vol. 38, no. 2, 2014, pp. 249–255.
Biswas M. et al. "Prevalence, types, clinical associations, and determinants of peripheral neuropathy in rheumatoid patients." Annals of Indian Academy of Neurology, vol. 14, no. 3, 2011, pp. 194–197.
Raneja A. et al. "Prevalence of peripheral neuropathy in patients with newly diagnosed rheumatoid arthritis." Indian Journal of Rheumatology, vol. 2, no. 2, 2007, pp. 47–50.
